
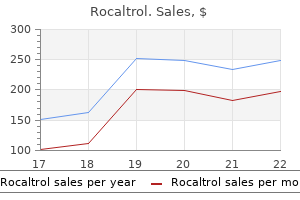
Rocaltrol
Discount 0.25 mcg rocaltrol
When a child scratches symptoms 6 days after embryo transfer order rocaltrol with american express, the eggs stick under his nails, and are carried to food and other objects. In this way they reach his own mouth or the mouths of others, causing new infections of pinworms. Treatment and Prevention: A child who has pinworms should wear tight diapers or pants while sleeping to keep him from scratching his anus. When one child is treated for these worms, it is wise to treat the whole family at the same time. Even if medicine gets rid of the worms, they will be picked up again if care is not taken with personal hygiene. By carefully following the guidelines of cleanliness, most of the worms will be gone within a few weeks, even without medicine. This worm, like the roundworm, is passed from the feces of one person to the mouth of another person. In children it occasionally causes part of the intestines to come out of the anus (prolapse of the rectum). For prolapse of the rectum, turn the child upside down and pour cool water on the intestine. Treat anemia by eating foods rich in iron and if necessary by taking iron pills (p. Where There Is No Doc to r 2009 143 Tapeworm In the intestines tapeworms grow several meters long. But the small, flat, white pieces (segments) found in the feces are usually about 1 cm. Occasionally a segment may crawl out by itself and be found in the egg cyst underclothing. When a person eats poorly cooked cysts meat, the cysts become tapeworms the cysts may cause in his intestines. Effect on health: Tapeworms in the intestines sometimes cause mild s to mach aches, but few other problems. People get these worms, like tapeworms, from eating infected pork or other meat that is not well cooked. Effect on health: Depending on the amount of infected meat eaten, the person may feel no effects, or she may become very sick or die. From a few hours to 5 days after eating the infected pork, the person may develop diarrhea and feel sick to her s to mach. Prevention of trichinosis: Only eat pork and other meat that has been well cooked. How they are transmitted: the s to ols of infected people contain millions of these tiny parasites. Because of poor sanitation, they get in to the source of drinking water or in to food, and other people become infected. Microscope Signs of infection with amebas: Many healthy people have amebas without becoming sick. However, bacterial dysentery (Shigella) begins more suddenly, the s to ols are more watery, and there is almost always fever (p. As a general rule: Diarrhea + blood + fever = bacterial infection (Shigella) Diarrhea + blood + no fever = amebas Occasionally bloody diarrhea has other causes. Prevention: Make and use latrines, protect the source of drinking water, and follow the guidelines of cleanliness. Eating well and avoiding fatigue and drunkenness are also important in preventing amebic dysentery. Giardia the giardia, like the ameba, is a microscopic parasite that lives in the gut and is a common cause of diarrhea, especially in children. A person who has yellow, bad-smelling diarrhea that is frothy Giardia as (full of bubbles) but without blood or mucus, probably has giardia. Other types, which cause bloody diarrhea, occur in Africa, South America, and Asia. In areas where these diseases are known to occur, any person who has blood in his urine or s to ols should have a sample of it tested for fluke eggs. In areas where schis to somiasis is very common, persons with only mild signs or belly pain should be tested. In this way, someone who washes or urinates or defecates swims in water where an infected person in water. To prevent schis to somiasis, cooperate with programs to kill snails and treat infected persons. It is better to take your children to the nearest health center to be vaccinated while they are healthy than to take them for treatment when they are sick or dying. A child needs 4 or 5 injections usually given at 2 months, 4 months, 6 months, and 18 months old. If any member of the household has tuberculosis, it is important to vaccinate babies in the first few weeks or months after birth. A child needs 1 injection given no younger than 9 months of age, and often a second injection at 15 months or older. One injection is given between 12 and 15 months old, and a second is given between 4 and 6 years of age. In some countries the first HepB is given at birth, the second at 2 months old, and the third at 6 months old. Make sure there are at least 4 weeks between the first and second injection, and 8 weeks between the second and third. Hib (for Haemophilus influenza type b, which is a germ that causes meningitis and pneumonia in young children). Throughout the world, tetanus vaccination is recommended with 1 injection every 10 years. Pregnant women should be vaccinated during each pregnancy so that their babies will be protected against tetanus of the newborn (see p. Give the oral vaccine 2 or 3 times (depending on the manufacturer) at 2, 4 and (if needed) 6 months old. The Introduction to the Village Health Worker gives ideas for getting people working to gether to change the conditions that cause poor health. In the remaining chapters, as specific health problems are discussed, you will find many suggestions for their prevention. By following these suggestions you can help make your home and village healthier places to live. Keep in mind that one of the best ways to prevent serious illness and death is early and sensible treatment. Before ending this chapter, we would like to mention a few aspects of prevention that are to uched on in other parts of the book, but deserve special attention.
Buy rocaltrol from india
A plastic surgery referral is also appropriate for a patient presenting late after augmentation mammoplasty with new symp to matic or objective breast complaints related to prior breast augmentation treatment by lanshin buy discount rocaltrol. Benign and malignant breast tumors are always in the differential diagnosis and should be worked up appropriately. Women who present with subjective dissatisfaction after previous breast augmentation may require a second surgical consultation or referral to another plastic surgeon. Prior to any referral for breast surgery, patients should be medically, psychologically, and socially stable, up- to -date in regard to breast cancer screening if indicated), and have reasonable postsurgical expectations. Anesthetic complications particular to gender-affirming feminizing mammoplasty In addition to standard anesthetic complications, patients undergoing feminizing mammoplasty should be assessed for risk fac to rs for venous thromboembolism,and appropriate mechanical and chemoprophylaxis measures applied based on individual risk fac to rs. Management of perioperative estrogen therapy and estrogenic risks of venous thromboembolism are discussed elsewhere in this pro to col. Hema to ma A hema to ma typically presents early (within 1-2 weeks) after augmentation mammoplasty, typically as a localized or unilateral swelling accompanied by pain and bruising at the surgical site. Specifically, the patient should be counseled to avoid strenuous activity and situations where the chest could be exposed to external trauma. Additionally, strict medical adherence (especially in regard to withholding anticoagulant, antiplatelet, and certain herbal medications and compliance with antihypertensive medications) can decrease incidence of pos to perative hema to ma. June 17, 2016 135 Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People Hema to mas are typically treated with surgical re-exploration, evacuation with identification of the bleeding source, and reclosure, with or without exchange of the prosthetic implant. An untreated large hema to ma can result in secondary complications, such as infection, capsular contracture, or implant malposition. There is no evidence in the plastic surgery literature to support the routine use of drains in augmentation mammoplasty. A delayed seroma is generally abnormal, and should be evaluated by a plastic surgeon. The severity of infection can range from a mild incisional cellulitis to a purulent periprosthetic infection. The most common pathogens in periprosthetic infections are skin flora, and as a result, surgeons go to extensive lengths to avoid contamination. However, most authors would advocate for implant removal in cases that fail to resolve, with delayed secondary augmentation performed in 6-12 months, once the patient has time to heal and fully clear the infection. Patients should be cautioned on appropriate scar care, including sun avoidance in the early pos to perative period. Patients with darker or oily skin types or a prior his to ry of hypertrophic scar or keloid formation should also be aware of their increased risk for these complications. In general, scarring from surgical incisions can be improved by following some basic tenets of postsurgical wound care. Firstly, reduction of mechanical stress and tension across the wound by following postsurgical activity restrictions is paramount to reducing scar width. Tension across the incision can result in minute wound disruptions, causing excessive or widened scar formation. Patients should be counseled that incisions predictably look the worst in the early stage of healing, up to 10 weeks pos to peratively, before they begin to remodel over the next several months to up to one year. Hyper or Hypopigmentation can also result in a more noticeable scar during this time of remodeling. We therefore recommend sun avoidance, or strong sunblock applied over a healed incision for the first year pos to peratively. This can take the form of gentle scar massage (beginning no earlier than 2 weeks pos to peratively and after the wound is fully healed), taping, or silicone gels and sheets. Implants placed prior to the late 2000s contained a liquid silicone gel which was prone to leakage, both due to shell rupture and leaching. Currently available silicone breast th th implants (4 or 5 generation implants, also termed cohesive gel implants), even a break in the outer shell of the implant will not allow free silicone gel to escape the implant. Implant malposition and capsular contracture Implant malposition can occur over time as the breast adapts to breast implant placement and aging. Pathologic fibrotic capsule formation, known as capsular contracture, can cause the implant to be hard and palpable, or cause implant displacement, breast deformation, or even breast pain related to the implant. Once symp to matic or disfiguring, implant removal and surgical excision of the capsule is indicated. Capsular contracture rates in modern implants are felt to be less than 10%, although long-term followup is needed. Inadequate size and aesthetic deformities A long-term study of transgender women who underwent augmentation mammoplasty found that 16% of the patients underwent a second augmentation procedure for breasts that were to o small. A number of aesthetically unappealing complications can occur and result in dissatisfaction requiring revisional surgery and secondary augmentation. These complications are generally a result of a combination of technique and patient ana to my. Some of these complications can include a visible implant and implant folding or rippling, which occurs in saline implants or when the patient has inadequate soft tissue covering the implant. Other patients can develop asymmetry related to scar formation or displacement over time by the action of the pec to ralis June 17, 2016 137 Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People muscle (in the case of submuscular implants). These deformities will need to be addressed with secondary revision breast augmentation procedures. Breast masses Breast cancer epidemiology and screening in transgender women is covered elsewhere in this pro to col. For those transgender women requiring screening or diagnostic mammography or breast ultrasound, both are possible with breast implants. However, mammography cannot detect implant-related complications, such as ruptures. Injection of silicone and other non-medical substances by unlicensed providers is covered in detail elsewhere in this pro to col. Long-term outcome of augmentation mammaplasty in male- to -female transsexuals: a questionnaire survey of 107 patients. The effect of hema to ma on the thickness of pseudosheaths around silicone implants. June 17, 2016 138 Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People 10. Silicone breast implants and magnetic resonance imaging screening for rupture: do U. Food and Drug Administration recommendations reflect an evidence-based practice approach to patient carefi June 17, 2016 139 Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People 29. In this technique, a vaginal vault is created between the rectum and the urethra, in the same location as a non-transgender female between the pelvic floor (Kegel) muscles, and the vaginal lining is created from penile skin. An orchiec to my is performed, the labia majora are created using scrotal skin, and the cli to ris is created from a portion of the glans penis. The prostate is left in place to avoid complications such as incontinence and urethral strictures. In the case of prior circumcision a skin graft, typically scrotal in origin, may be required. If there is insufficient skin between the penis and the scrotum to achieve 12cm (5 inches) of depth, a skin graft from the hip, lower abdomen or inner thigh may be used. Resultant scarring at the donor site may be minimized or hidden using standard techniques. Because the penile inversion approach does not create a vaginal mucosa, the vagina does not self-lubricate and requires the use of an external lubricant for dilation or penetrative sex. Scrotal skin has abundant hair follicles and it is possible to transfer skin with sparse hair growth in to the vagina unless hair is removed in advance. Some surgeons rely on treating all the visible hair with aggressive thinning of the skin and cauterization of visible hair follicles at the time of surgery. However, since hair grows in stages this approach might not adequately address dormant follicles.
Purchase rocaltrol us
Inability to speak with choking medications you can take while pregnant cheap rocaltrol 0.25mcg, nervous, chronic palpitation, especially after public speaking; pain < by carriage riding or lying on side. Chronic effects of sunstroke; now, with the return of hot weather, suffers from headaches. Emaciation with pale face and blue rings around the eyes, dilated pupils; dark urine; anaemic; milky, watery skin and great debility. Inability to think or perform any mental labor, causes headache; feels stupefied if he tries to exert himself; comprehension slow, difficult. Headache: from slightest mental exertion; form sun or working under gaslight (Glon. Face pale, with blue rings around eyes; eyelids swollen; catarrh; mucus in throat and posterior nares; constantly hawking to clear throat; dropping in to the throat from posterior nares. Catarrh: extends to posterior nares and throat; hawking much thick mucus from throat; profuse discharge during day, s to pped at night (Nux). Thick, yellow, green, offensive, musty, hard discharge from nose; often ceasing after a meal. Common Salt (NaCl) For the anaemic and cachetic; whether from loss of vital fluids profuse menses, seminal losses or mental affections. Irritability: child cross when spoken to ; crying from slightest cause; gets in to a passion about trifles, especially when consoled with. Hay fever: squirming sensation in the nostril, as of a small worm; brought on by exposure to hot sun or intense summer heat. Constipation: sensation of contraction of anus; to rn, bleeding, smarting afterwards; s to ol, dry, hard, difficult, crumbling (Am. Seminal emission: soon after coition, with increased desire; weakness of organs with retarted emission during an embrace; impotence, spinal irritation, paralysis, after sexual excesses. Pressing, pushing to wards genitals every morning; must sit down to prevent prolapsus (Lil. For the bad effects: of anger (caused by offence); acid food, bread, quinine, excessive use of salt; of cauterization of all kinds with the silver nitrate; to grief, fright, vexation, mortification or reserved displeasure (Staph. Dreams: of robbers in the house, and on waking, will not believe to the contrary until search is made (Psor. Fever blisters, like pearls about the lips; lips dry, sore and cracked, ulcerated (Nit. Eczema; raw, red, inflamed, especially in edges of hair; < from eating to o much salt, at sea shore, or from ocean voyage. Urticaria, acute or chronic; over whole body; especially after violent exercise (Apis, Cal. Cannot often be repeated in chronic cases without an intercurrent, called for by the symp to ms. If vertigo and headache be very persistent, or prostration be prolonged after Natrum, Nux will relieve. Patient feets every change from dry to wet; cannot to lerate sea air, nor eat plants that thrive near water; a constitution in which gonorrhoeal poison is most pernicious; recovers slowly from every sickness. Sad, gloomy, irritable; worse in mornings; dislikes to speak or be spoken to (Iod. Depressed; lively music makes her sad; satiety of like; must use great self-control to prevent shooting himself. Mental traumatism; mental effects from injuries to head; chronic brain effects of blows, falls. Granular lids: like small blisters (Thuja); green pus and terrible pho to phobia; gonorrhoeal or sycotic. Diarrhoea: sudden, urging, gushing, much flatus; on first rising and standing on the feet; after a spell of wet weather; living on working in basements. Humid asthma in children; with every change to wet weather; with every fresh cold; always worse in damp, rainy weather; sputa green, greenish, copious (greenish grey, Cop. Sycotic pneumonia; lower lobe of left lung; great soreness of chest, during cough, has to sit up in bed and hold the chest with both hands (Nic. Spinal meningitis: violent crushing gnawing pains at base of brain; head drawn back; spasms with mental irritability and delirium; violent congestion of blood to head; delirium; opistho to nos. Must change position frequently, but it is painful and gives little relief (Caust. Persons suffering with chronic diseases who take cold easily; are easily disposed to diarrhoea; rarely to those who suffer with constipation. Pains: sticking, pricking as from splinters; suddenly appearing and disappearing; on change of temperature or weather; during sleep; gnawing here and there as from ulcers forming. Ailments: which depend on some virulent poison; from mercury, syphilis, scrofula; in broken-down cachetic constitutions. After continual loss of sleep, long-lasting anxiety, over-exertion of mind and body from nursing the sick (Coc. Great anxiety about his disease; constantly thinking about his past troubles; morbid fear of cholera (Ars. Irritable, headstrong; hateful and vindictive; inveterate, ill-willed, unmoved by apologies. Very sensitive to rattle of wagon over paved streets; headache from pressure of hat (Cal. Diarrhoea: great straining but little passes, as if faeces remained and cannot be expelled (Alum. Fissures in rectum; tearing, spasmodic pains during s to ols; lancinating, even after soft s to ols (Alumen. Discharges; thin, offensive, acrid; of a brown or dirty yellowish green color; rarely laudable pus. Warts, condylomata: sycotic or syphilitic; large, jagged, pedunculated; bleeding readily on washing; moist, oozing, sticking pain (Staph. Affects especially the mucous membrane join; mouth, nose, rectum, anus, urethra, vagina (Mur. Relieve ailments resulting from abuse of mercury, especially, if there be erethism; bad effects of repeated doses of Digitalis. Vanishing of thoughts while reading, talking or writing; using wrong words; does not recognize well known streets (Can. Sensation of great dryness without real thirst and without actual dryness of the to ngue. Eating a little to o much causes headache; painfulness and distress in s to mach while eating or immediately after (Kali bi. At every menstrual nisus, mouth, throat and to ngue become in to lerably dry, especially when sleeping. Sleep: irresistibly drowsy; sleepy, muddled, as if in to xicated; coma, lies silent, immovable; eyes constantly closed (with ste to rous breathing, Op. Rheumatic affections; from getting feet wet; from exposure to drafts to air while heated (Acon. Debauchers of a thin, irritable, nervous disposition; prone to indigestion and haemorrhoids (persons with light hair, blue eyes, Lob. Anxiety with irritability and inclination to commit suicide, but is afraid to die. Hypochondriac: literary, studious persons, who are to o much at home, suffer from want of exercise, with gastric, abdominal complaints and costiveness; especially in drunkards. Persons who are very particular, careful, but inclined to become easily excited or angered; irascible and tenacious. Bad effects of: coffee, tabacco, alcoholic stimulants; highly spiced or seasoned food; over-eating (Ant. One of the best remedies with which to commence treatment of cases that have been drugged by mixtures, bitters, vegetable pills, nostrums or quack remedies, especially aromatic or "hot medicines. Cannot keep from falling asleep in the evening while sitting or reading hours before bedtime, and wakes at 3 or 4 a. Eructations: sour, bitter, nausea and vomiting every morning with depression of spirits; after eating.

| Comparative prices of Rocaltrol | ||
| # | Retailer | Average price |
| 1 | Starbucks | 175 |
| 2 | AutoZone | 380 |
| 3 | RadioShack | 523 |
| 4 | Wegman's Food Markets | 718 |
| 5 | Belk | 650 |
| 6 | OSI Restaurant Partners | 666 |
Order rocaltrol 0.25 mcg visa
World Professional Association for Transgender Health 31 the Standards of Care 7th Version 2 treatment zap buy generic rocaltrol canada. Provide information and referral for peer support For some transsexual, transgender, and gender nonconforming people, an experience in peer support groups may be more instructive regarding options for gender expression than anything individual psychotherapy could offer (Rachlin, 2002). Both experiences are potentially valuable, and all people exploring gender issues should be encouraged to participate in community activities, if possible. Culture and its Ramifcations for Assessment and Psychotherapy Health professionals work in enormously different environments across the world. Forms of distress that cause people to seek professional assistance in any culture are unders to od and classifed by people in terms that are products of their own cultures (Frank & Frank, 1993). Cultural settings also largely determine how such conditions are unders to od by mental health professionals. Cultural differences related to gender identity and expression can affect patients, mental health professionals, and accepted psychotherapy practice. Professionals must adhere to the ethical codes of their professional licensing or certifying organizations in all of their work with transsexual, transgender, and gender nonconforming clients. If mental health professionals are uncomfortable with or inexperienced in working with transsexual, transgender, and gender nonconforming individuals and their families, they should refer clients to a competent provider or, at minimum, consult with an expert peer. If no local practitioners are available, consultation may be done via telehealth methods, assuming local requirements for distance consultation are met. Providing mental health care from a distance through the use of technology may be one way to improve access (Fraser, 2009b). In many places around the world, access to health care for transsexual, transgender, and gender nonconforming people is also limited by a lack of health insurance or other means to pay for needed care. When faced with a client who is unable to access services, referral to available peer support resources (offine and online) is recommended. Finally, harm reduction approaches might be indicated to assist clients with making healthy decisions to improve their lives. Some people seek maximum feminization/ masculinization, while others experience relief with an androgynous presentation resulting from hormonal minimization of existing secondary sex characteristics (Fac to r & Rothblum, 2008). Evidence for the psychosocial outcomes of hormone therapy is summarized in Appendix D. A referral is required from the mental health professional who performed the assessment, unless the assessment was done by a hormone provider who is also qualifed in this area. If signifcant medical or mental health concerns are present, they must be reasonably well controlled. In selected circumstances, it can be acceptable practice to provide hormones to patients who have not fulflled these criteria. Examples include facilitating the provision of moni to red therapy using hormones of known quality as an alternative to illicit or unsupervised hormone use or to patients who have already established themselves in their affrmed gender and who have a his to ry of prior hormone use. In rare cases, hormone therapy may be contraindicated due to serious individual health conditions. Health professionals should assist these patients with accessing non-hormonal interventions for gender dysphoria. A qualifed mental health professional familiar with the patient is an excellent resource in these circumstances. Thus, hormone therapy should be provided only to those who are legally able to provide informed consent. This includes people who have been declared by a court to be emancipated minors, incarcerated people, and cognitively impaired people who are considered competent to participate in their medical decisions (see also Bockting et al. Providers should document in the medical record that comprehensive information has been provided and unders to od about all relevant aspects of the hormone therapy, including both possible benefts and risks and the impact on reproductive capacity. Obtaining informed consent for hormone therapy is an important task of providers to ensure that patients understand the psychological and physical benefts and risks of hormone therapy, as well as its psychosocial implications. Providers prescribing the hormones or health professionals recommending the hormones should have the knowledge and experience to assess gender dysphoria. Screening for and addressing acute or current mental health concerns is an important part of the informed consent process. The same provider or another appropriately trained member of the health care team. If indicated, these providers will make referrals for psychotherapy and for the assessment and treatment of co-existing mental health concerns such as anxiety or depression. This may include a comprehensive mental health assessment and psychotherapy, when indicated. In the Informed Consent Model, the focus is on obtaining informed consent as the threshold for the initiation of hormone therapy in a multidisciplinary, harm-reduction environment. Less emphasis is placed on the provision of mental health care until the patient requests it, unless signifcant mental health concerns are identifed that would need to be addressed before hormone prescription. Most physical changes, whether feminizing or masculinizing, occur over the course of two years. The amount of physical change and the exact timeline of effects can be highly variable. D Complete removal of male facial and body hair requires electrolysis, laser treatment, or both. All other fac to rs being equal, there is no evidence to suggest that any medically approved type or method of administering hormones is more effective than any other in producing the desired physical changes. It is thus impossible to predict whether a given adverse effect will happen in an individual patient. The risks associated with feminizing/masculinizing hormone therapy for the transsexual, transgender, and gender nonconforming population as a whole are summarized in Table 2. Based on the level of evidence, risks are categorized as follows: (i) likely increased risk with hormone therapy, (ii) possibly increased risk with hormone therapy, or (iii) inconclusive or no increased risk. Items in the last category include those that may present risk, but for which the evidence is so minimal that no clear conclusion can be reached. Additional detail about these risks can be found in Appendix B, which is based on two comprehensive, evidence-based literature reviews of masculinizing/feminizing hormone therapy (Feldman & Safer, 2009; Hembree et al. These reviews can serve as detailed references for providers, along with other widely recognized, published clinical materials (Dahl, Feldman, Goldberg, & Jaberi, 2006; Ettner, Monstrey, & Eyler, 2007). C Includes bipolar, schizoaffective, and other disorders that may include manic or psychotic symp to ms. With appropriate training, feminizing/masculinizing hormone therapy can be managed by a variety of providers, including nurse practitioners and primary care physicians (Dahl et al. Medical visits relating to hormone maintenance provide an opportunity to deliver broader care to a population that is often medically underserved (Clements, Wilkinson, Kitano, & Marx, 1999; Feldman, 2007; Xavier, 2000). Many of the screening tasks and management of co-morbidities associated with long-term hormone use, such as cardiovascular risk fac to rs and cancer screening, fall more uniformly within the scope of primary care rather than specialist care (American Academy of Family Physicians, 2005; Eyler, 2007; World Health Organization, 2008), particularly in locations where dedicated gender teams or specialized physicians are not available. Conversely, an experienced hormone provider or endocrinologist should be involved if the primary care physician has no experience with this type of hormone therapy, or if the patient has a pre-existing metabolic or endocrine disorder that could be affected by endocrine therapy.
Generic 0.25 mcg rocaltrol mastercard
Conservative treatment Will often need further soft-tissue coverage Stable medicine in balance cheap rocaltrol on line, non displaced fractures of the tibial shaft can procedure. In the clinical exa Due to a long period of immobilization conservative mination they often present instability and malposition treatment includes a high risk of deep venous thrombo to gether with swelling and hema to ma. X-rays in two sis, compartment syndrome, soft tissue injury and chro planes are sufficient as the primary diagnostic to ol and nic regional pain syndrome. Intramedullary nailing provides a huge ries and compartment syndrome is also more difficult in biomechanical stability and unreamed intramedullary a cast. The use of external fixation has declined, although being a biological osteo Operative treatment synthesis easy to apply. Operative treatment with standardized pro to cols is Only rare indications for plate osteosynthesis due to very common. As mentioned before, long time cast huge iatrogenic soft tissue damage can be found, even application is highly uncomfortable for the patient. The initial stabilization is performed with an external fixa to r and after recovery of the patient the implant is changed to wards an internal osteosynthesis. Intramedullary nailing Biomechanical stability and minimally invasive app roach with distance to the fracture are the major advan tages of intramedullary nailing. Evidence supports the use of intramedullary nailing in diaphyseal tibial fractures as the implant of choice (3, 4). There is also strong evidence that intramedul lary nails offer a benefit over external fixation in open fractures if wound closure is performed soon (4). Intramedullary nailing is indicated for open and clo sed isolated tibia shaft fractures (Fig. They concluded that reaming on the one hand disrupts the blood flow to the cortex but on the other hand induces a six fold increase in periosteal blood flow (28, 37). This reaction does not occur in open fractures with frequent severe periosteal damage possibly contributing to the lack of benefit in open fractures. A recent Cochrane review published by Duan X et al outlined that there is no clear difference in the rate of major re-operations and complications between reamed or unreamed nailing. In conclusion reaming acts like an osteogenic debris Intramedullary nailing is well established as a stan similar to an au to logous bone graft. Improved union dard treatment for diaphyseal fractures of the long bone rates following reaming have been described in closed despite the negative effects such as endosteal necrosis tibial shaft fractures while the benefit in open fractures and systematic fat embolism (25). One key area is whether intramedul wound infections, good-fracture healing and an increa lary nails should be inserted with reaming or unreamed. Certain Another issue is whether intramedullary nails should be ly further studies moni to ring longer terms of follow up locked with locking screws or not. Intramedullary reaming deposits the debris formed by reaming at the fracture site, acting like an au to logous Plate osteosynthesis bone graft and also improves cortical contact with Conventional plate osteosynthesis used to be the met improved stability (38). In vitro studies have shown that hod of choice for tibial shaft fractures without soft tis intramedullary reaming in combination with an irrigati sue injury until recently being replaced by intramedul on and aspiration system (Reamer/Irriga to r/Aspira to r lary nailing with locking screws (29). Sub Blood supply and soft tissue covering are the major pro sequently the concept of bridging plate and biological blems in tibial shaft fractures while fat embolism is more osteosynthesis where implemented with the use of angu relevant in femur fractures. These developments allowed supply has shown to be responsible for the negative careful surgical techniques with the prevention of soft effects of intramedullary reaming. Nevertheless indication for plate osteo amed intramedullary nailing has experienced widespre synthesis in tibial shaft fractures is rare (29). In current ad clinical application in open and closed tibial shaft literature indication for plate osteosynthesis can be fractures (32). They recommended not to use unreamed nailing in cated in open fractures or patients with former injuries the treatment of the common Tscherne C1 tibial fractu to their lower limb or vessel diseases. Primary external fixation is also often useful in seve re soft tissue injuries without any fractures and provides immobilization. External fixa to rs are still used for the definitive treat ment of juvenile tibia shaft fractures (47). Soft tissue injuries and open fractures Infection is the most common and devastating com plication of open fractures with a reported incidence of 3-40% (2, 6, 7, 10, 18, 19, 20, 21, 30, 34, 35, 36). Distal tibial shaft frature, Typ 42 C2 with primary supply and lack of soft tissue coverage explain the high external fixation and secondary intramedullary nailing of rate of infection and non-union. These complicati ons could be reduced by the development of treatment pro to cols, which include immediate intravenous anti biotic application, radical soft tissue debridement, ear ly soft tissue covering and stabilization of the fracture (12, 35). The choice of technique for the stabilization of open tibial fractures still remains controversial. Advantages of external fixation such as ease of application and the limi ted effect on the blood supply have been outweighed by high rates of pin track infection, difficulties in soft-tissue management and relatively high rates of non-union (50). Intramedullary nailing has therefore becoming more and more popular even in open fractures. Unreamed intramedullary nailing potentially compromises stabili ty at the fracture site. Reamed intramedullary nailing on the other hand offers improved stability but also suffers a theoretical risk of increasing infection and non-union by destruction of endosteal blood supply. External fixa to r From our point of view, therapeutically strategy has to Before implementation of intramedullary nailing with follow the damage control concept (46). Patients at high locking screws, external fixation was the most common risk such as those suffering multiple trauma, thorax or surgical treatment for open fractures of the tibial shaft. External fixation is indicated as primary stabilization for multiple trauma patients, severe soft tissue injury clo Complications se to the joints or generally inoperable patients. There Seroma, necrosis and infection with the late onset of are no contraindications for external fixation in tibial osteomyelitis are the most common complications in shaft fractures. In some cases they may even re tients following the damage control principle, the initi quire surgical intervention. Especially young patients with dia References physeal fractures are at risk for developing compart 1. The diagnosis of compartment syndrome primary management on the incidence of deep infection after open is dominated by clinical signs (27) and fascio to my is fractures of the lower extremities caused by blunt trauma in adults. A prospective study in Tscherne C1 frac rosis needs stability that can be achieved with a method tures. Orthopadie und Trauma to logie phase after long-bone injury of the lower extremity in multiple Klinik fur Trauma to logie injured patients. The medical information found on this website should not be used in place of a consultation with your doc to r or other health care provider. You should always seek the advice of your doc to r or other qualifed health care provider before you start or s to p any treatment or with any questions you may have about a medical condition. Many people already have had fifth disease Most people get infected between 5 and 14 years of age. It is estimated that about half the adults in the United States have been infected with parvovirus B19 and therefore can not get it again. A red, patchy, "slapped cheek" rash on the face is common during infection the rash may appear on other parts of the body (such as the arms, trunk, but to cks, and thighs). Other symp to ms such as fever, headache, body ache, sore throat, congestion, runny nose, cough, nausea, or diarrhea may come before the rash. In both children and adults, the disease is usually mild and recovery occurs without problems. A person with fifth disease usually spreads the virus before the rash starts the virus is spread by exposure to airborne droplets from the nose and throat of infected people. There is a blood test, but it is not widely available A blood test for antibodies is used to see if a person is currently infected or was infected in the past. In most cases, the disease is diagnosed based on the appearance of a typical rash. There is no specific treatment or vaccine for fifth disease at this time Some people are at higher risk of complications or serious illness if they get fifth disease: fi Unborn fetuses of pregnant women who develop fifth disease. Miscarriages and stillbirths are uncommonly associated with parvovirus infection, but are more frequent when infection occurs during the first half of pregnancy. Parvovirus infection later during pregnancy can lead to severe anemia in the fetus, prematurity, or stillbirth. Those at risk should check with their doc to r Those at increased risk for serious illness or complications should realize that they might catch fifth disease from family members, others in the community, and in child care, school, or other occupational settings.
Discount rocaltrol 0.25 mcg online
By the time the rash is evident medicine woman cast buy rocaltrol 0.25mcg without prescription, the individual is no longer contagious (except for people with compromised immune systems). In most cases, fifth disease is diagnosed based on the appearance of the characteristic rash. Infected people who have compromised immune systems and certain blood disorders should contact their health-care provider for possible supportive care. It is thought that people who have previously been infected acquire long-term or lifelong immunity. Studies have shown that about 50 percent of adults and more than 90 percent of elderly people are immune to parvovirus B19 and therefore are not susceptible. Should children or others be excluded from child care, school, work or other activities if they have fifth diseasefi Because the risk of transmitting B19 virus to others is greatest before signs and symp to ms develop, transmission cannot be prevented by identifying and excluding symp to matic individuals. Pregnant women may continue going to their workplace if there is an outbreak of fifth disease happening. However, if you are not immune to parvovirus B19 and are not currently infected, you may want to stay away from people with fifth disease while you are pregnant. Good hand washing may be a practical and effective method to reduce the spread of the virus in schools or day-care centers where there are known cases. The ill child typically has a "slapped-cheek" rash on the face and a lacy red rash on the trunk and Parvovirus B19 limbs. The ill child typically has a "slapped-cheek" rash on the face, which may be followed by a lace like rash on the trunk and limbs. The child may have a low-grade fever, runny nose, and nausea and diarrhoea a few days before the rash breaks out. The rash resolves in 7 to 10 days but may recur in when exposed to sunlight or heat for 3 weeks or longer. An adult who is infected with parvovirus B19 may have no symp to ms at all, or may develop a rash, joint pain or swelling, or both. It is usually the small joints of both hands and occasionally ankles, knees and wrists that are affected. Symp to ms usually develop between 4 and 20 days after being infected with the virus. The virus is spread by contact with infected respira to ry secretions (for example, by coughing), and from mother to unborn baby. Usually there is no serious complication for a pregnant woman or her baby following exposure to a person with parvovirus B19 infection. About 50 per cent of women are already immune to parvovirus B19, and these women and their babies are protected from infection and illness. Rarely, miscarriages can occur usually when the mother becomes infected early in the pregnancy. A doc to r can often diagnose parvovirus B19 by seeing the typical rash during a physical examination. In cases in which it is important to confirm the diagnosis, a blood test may be done to look for antibodies to parvovirus. Treatment of symp to ms such as fever, pain, or itching is usually all that is needed for parvovirus B19. Adults with joint pain and swelling may need to rest, restrict their activities, and take medicines such as aspirin or ibuprofen to relieve symp to ms. Infected individuals are not excluded form childcare, school or work but should be advised to rest at home until they feel better. For further information please call your local Public Health Unit on 1300 066 055 or visit the New South Wales Health website Services, Vic to ria, nor any person We would also like to acknowledge and associated with the preparation of these thank the following contribu to rs for their guidelines accept any contractual, assistance: to rtious or other liability whatsoever in respect of their contents or any A/Prof Heath Kelly, Vic to rian Infectious consequences arising from their use. Printed by this document may also be downloaded from the Department of Human Services web site at: In mild cases propamidine eye drops are the epidemiology of acute bacterial the usual treatment. The clinical syndrome ranges from mild Infections are most common in children Consult the current version of redness of the conjunctivae to corneal under five years of age and incidence Therapeutic guidelines: antibiotic infiltration and visual disturbances in decreases with age. Trachoma should Reservoir articles should be discarded or be suspected in the presence of Humans. Rigorous hand washing lymphoid follicles and diffuse before and after eye examinations and conjunctival inflammation or trichiasis Mode of transmission to ilets is important in preventing further (inturned eyelashes). Early symp to ms may aerobic rod-shaped bacterium that is from reference labora to ries. Lesions usually occur on Intestinal/oropharyngeal anthrax Public health significance exposed skin and often commence with these are very rare forms of anthrax in and occurrence itchiness. Always consult the is no evidence of transmission through current version of Therapeutic guidelines: Reservoir the milk of an infected animal. Cutaneous anthrax is usually Period of communicability the duration of therapy for introduced through a skin injury. If one or where meningitis is suspected because is advised to suspend collection of milk more patients seem to have been of the lack of adequate central nervous until the case is investigated and Dairy infected in an unusual way, such as no system penetration by the latter. Incubation period the infective agents are Ascaris Transmission does not occur from direct the lifecycle requires four to eight weeks lumbricoides, a large intestinal person to person contact or from fresh to complete. The eggs hatch in the small unsegmented when passed and require a 30 cm in length) and Ascaris suum,a intestine and larvae pass through the period of two or three weeks outside the similar parasite primarily affecting pigs intestinal wall in to the blood. In the lungs they have a further Identification estimated to produce an average of 200 period of development. Ascariasis the mature fertilised female worm lives in aggravates malnutrition in the prevalence and intensity of infection the intestine. Pulmonary involvement may be confirmed by Control measures Reservoir identifying ascarid larvae in the sputum Preventive measures Ascaris eggs in soil or infected humans or gastric washings. Consult the current version of Therapeutic guidelines: antibiotic (Therapeutic Guidelines Limited). Control of contacts Consider faecal screening of household members to determine if they also require treatment. The virus may Vic to rian statu to ry requirement camp to rhynchus in southern parts of be isolated from the blood of acutely ill Barmah Forest virus infection (Group B Vic to ria and Tasmania are the vec to rs in patients. Virological tests are necessary disease) requires notification in writing coastal regions. It has also been isolated from numerous other mosqui to es Incubation period including the coastal species the incubation period appears to be Ochlerotatus vigilax (New South Wales) seven to ten days. The blue book: Guidelines forthe control of infectious diseases 17 Botulism Vic to rian statu to ry requirement Method of diagnosis Mode of transmission Clostridium botulinum infection (Group A Diagnosis is made by culture of Classical botulism is acquired by disease) must be notified immediately by C. Several cases have been reported Incubation period Clostridium botulinum is a spore-forming amongst chronic drug users. The illness typically begins Australia National Notifiable Diseases techniques about cooking time, pressure, with constipation followed by lethargy, Surveillance System). The absence of a bulging lid on difficulty in swallowing and generalised potential bioterrorist agent. The case-fatality rate in organism vary according to geographic Educate the public, particularly travellers, untreated brucellosis is approximately area.
Order rocaltrol 0.25 mcg overnight delivery
Silver Spring symptoms of ms purchase rocaltrol line, Maryland Rockville, Maryland Office of Special Health Affairs Krystyna Isaacs, Ph. Rockville, Maryland Rockville, Maryland Principal & Senior Medical Advisor Bob Huebner, Ph. Understanding Alcohol Use Disorders and Their National Clinical Guideline Centre for Acute and Treatment. Results From the 2013 National Survey on Drug Use and Health: Summary of National Findings. Identification of and guidance for problem drinking by general medical providers: results from a national survey. Treatment implications: using neuroscience to guide the development of new pharmacotherapies for alcoholism. Primary care intervention to reduce alcohol misuse: ranking its health impact and cost effectiveness. Pharmacokinetic drug interactions and adverse consequences between psychotropic medications and pharmacotherapy for the treatment of opioid dependence. Alcohol biomarkers in applied settings: recent advances and future research opportunities. Screening for excessive alcohol drinking: comparative value of carbohydrate-deficient transferrin, gamma-glutamyltranserase, and mean corpuscular volume. Carbohydrate-deficient transferrin and conventional alcohol markers as indica to rs for brief intervention among heavy drinkers in primary health care. Assessing the drinking status of liver transplant patients with alcoholic liver disease. Phosphatidylethanol: the potential role in further evaluating low positive urinary ethyl glucuronide and ethyl sulfate results [published online ahead of print]. Age at drinking onset and alcohol dependence: age at onset, duration, and severity. Chemical Management Emergency Medical Management, Department of Health & Human Services Web site. Update on neuropharmacological treatments for alcoholism: scientific basis and clinical findings. Disulfiram metabolism as a requirement for the inhibition of rat liver mi to chondrial low Km aldehyde dehydrogenase. A randomized, multicenter, open-label, comparative trial of disulfiram, naltrexone and acamprosate in the treatment of alcohol dependence. Efficacy and safety of naltrexone and acamprosate in the treatment of alcohol dependence: A systematic review. The efficacy of acamprosate and naltrexone in the treatment of alcohol dependence: a relative benefits analysis of randomized controlled trials. Naltrexone for the treatment of alcoholism: a meta-analysis of randomized controlled trials. Opioid antagonists in the treatment of alcohol dependence: clinical efficacy and prevention of relapse. Efficacy and to lerability of long-acting injectable naltrexone for alcohol dependence: a randomized controlled trial. Efficacy of extended-release naltrexone in alcohol dependent patients who are abstinent before treatment. Predicting treatment response to naltrexone: the influence of craving and family his to ry. Clinical predic to rs of response to naltrexone in alcoholic patients: who benefits most from treatment with naltrexonefi Pharmacological enhancement of naltrexone treatment for opioid dependence: a review. Acamprosate: a review of its use in the maintenance of abstinence in patients with alcohol dependence. Acamprosate for treatment of alcohol dependence: mechanisms, efficacy, and clinical utility. Predic to rs of acamprosate efficacy: results from a pooled analysis of seven European trials including 1,485 alcohol-dependent patients. Effect of oral acamprosate on abstinence in patients with alcohol dependence in a double-blind, placebo-controlled trial: the role of patient motivation. The efficacy of acamprosate in the maintenance of abstinence in alcohol-dependent individuals: results of a meta-analysis. Opioid de to xification and naltrexone induction strategies: Recommendations for clinical practice. Naltrexone: Extended-release injectable suspension for treatment of alcoholism dependence. Department of Justice, Drug Enforcement Agency, Office of Diversion Control Web Site. Two-year experience with buprenorphine/naloxone (Suboxone) for maintenance treatment of opioid dependence within a private practice setting. Ziegler, Dusseldorf, Germany In addition, the following scientists were appointed for drafting the 1st edition: Prof. Corvin, Tubingen, Germany (Urology) Literature evaluation and supporting methods: M. Redaelli, Cologne, Germany the revision and updating of the 2nd edition (May 2004) was undertaken by the same group of experts. Sensorimo to r diabetic neuropathies include all neuropathic manifestations listed in Table 1 except for diabetic au to nomic neuropathy. Classification of diabetic neuropathies (according to Thomas and Tomlinson, 1993) Symmetric Polyneuropathies Sensory or sensorimo to r polyneuropathy Au to nomic neuropathy Symmetric proximal neuropathy of the lower extremities Focal and multifocal neuropathies Cranial neuropathy Mononeuropathy of the trunk and extremities Asymmetric proximal neuropathy of the lower extremities Mixed forms 2 Epidemiology For patients with type 1 or type 2 diabetes, the prevalence of sensorimo to r diabetic neuropathies is about 30 per cent [Ziegler, 1994, level V; Tesfaye et al. Quality of life is impaired in comparison with patients without sensorimo to r diabetic neuropathies [Benbow et al. Sensorimo to r diabetic neuropathy is the most important risk fac to r for nontraumatic amputations of the lower extremities. In Germany, the number of nontraumatic amputations in patients with diabetes mellitus is estimated to be over 20,000 per year [Standl et al. Furthermore, there is an association with diabetes duration, blood sugar control, diabetic retinopathy and other risk fac to rs (Table 3) [Pirart et al. Today, as a result of prospective studies, there is increasing evidence that individual measures of polyneuropathy such as an increase in the vibration perception threshold and a slowing of the nerve conduction velocity indicate an increased mortality risk [Forsblom et al. Presently discussed pathogenetic mechanisms of diabetic neuropathy [according to Neundorfer, 1996 and Ziegler, 1998] 1. Disturbances in the metabolism of the n-6 essential fatty acids and prostaglandins that lead to a change in the structure of the nerve membrane as well as microvascular and haemorrheologic changes 3. Disturbances in neurotrophism with reduced expression and deficiency of neurotrophic fac to rs. Michigan score with a simple list of questions) have been proposed [Feldmann et al. Feeling of weakness (fatigue, exhaustion) fi 1 fi 0 Cramps fi 1 fi 0 Pain fi 1 fi 0 fi pt. Exacerbation Present at night fi 2 Present during day and night fi 1 Only present during the day fi 0 Patient is awakened from sleep Score from by the symp to ms fi 1 add fi pt. Diagnostic criteria of different manifestations of sensorimo to r diabetic neuropathies [according to Boul to n et al.
Buy rocaltrol overnight
It can also have direct and indirect effects on research data treatments for depression order rocaltrol 0.25mcg fast delivery, by its effects on a range of biological processes. For example, it has been shown to influ ence implantation rates after embryo transfer (Bagis et al. It is therefore essen tial to take effective measures to prevent even mild hypothermia from developing. Preventive Measures Careful pre and intra-operative management can reduce any fall in body tem perature. Most animals will require some additional heating and insulation to minimize heat loss. Effective insulation can be provided either by wrapping the animal in cot to n wool, followed by an outer wrapping of aluminium foil, or by using the bubble packing which frequently forms part of the packaging of labo ra to ry equipment, or other insulating materials. After wrapping the animal in an insulating layer of material, a window can be cut to expose the operative field (Fig. When insulating small rodents, ensure that the tail is included in the wrapping, since heat loss from this part can be considerable. These simple meas ures will help reduce heat loss, but supplemental heating should be considered essential, even for brief periods of anaesthesia in small animals. Supplemental heating can be provided by heat lamps and heating blankets, but care must be taken not to burn the animal. Chapter | 3 Anaesthetic Management 107 the animal, or between the animal and a heating pad, will show whether exces sive heat is being applied. It is possible to cause hyperthermia by over-enthusiastic or uncontrolled heating, and this can result in superficial burns or even the death of the animal. It is important to switch on heating pads and lamps before they are required, to allow their temperature to stabilize and to prevent a period of inadequate heating when the pad or lamp is warming up. Thermostatically controlled pads can be set up with the probe in contact with the blanket, so that they reach body temperature before the animal is anaesthetized. Heating blankets may use electrical elements, have circulating warm water, or employ warm air. Warm water heating systems may not provide sufficient warmth for small animals because of the fall in water temperature between the water res ervoir and the blanket, but are effective in larger species (Sikoski et al. Vomiting and Regurgitation Vomiting or regurgitation of s to mach contents may occur either during induction of anaesthesia or during the recovery period. Inhalation of gastric contents can produce imme diate respira to ry obstruction, asphyxiation and death, or lead to the development of aspiration pneumonia. If vomiting occurs, the animal should immediately be placed in a head-down position and the vomit aspirated from the mouth and pharynx. If an effective suction apparatus is not available, one can be improvised from a large-diameter catheter and a 50ml syringe. Since speed of reaction is of paramount importance, such apparatus should be available as standard equipment in the anaesthetic preparation room and recovery area. If aspiration of vomit has occurred, oxygen should be administered and ven tilation supported if respira to ry distress develops. A broad-spectrum antibiotic should be administered, and corticosteroids given immediately by the intrave nous route (30mg/kg methyl prednisolone). It is obviously preferable to reduce the incidence of vomiting and its asso ciated problems by withholding food pre-operatively when appropriate (see Chapter 1) and by rapid endotracheal intubation of all animals whenever this is practicable. Chapter 4 Special Techniques Some research procedures require the use of more specialized anaesthetic techniques. Use of these agents is challenging, and requires careful moni to ring of anaes thetic depth. Their use will also require use of controlled ventilation and an understanding of the function of mechanical ventila to rs and the various types of apparatus that are avail able. Mechanical ventilation may also be needed during long-term anaesthesia, another challenging technique. Maintaining anaesthesia for prolonged periods can be achieved using a variety of ways. The advantages and disadvantages of the different techniques in relation to the scientific aims of the procedure, the experience of the staff, the welfare and well-being of the animals involved must be carefully considered. Some groups of animals also provide particular challenges, for example anaesthesia of pregnant animals, fetuses and neonates. Finally, this chapter briefly outlines some of the particular issues relating to anaesthesia for non-invasive imaging. They may be used either to aid stable mechanical ventilation by blocking spontaneous respira to ry move ments or, more frequently, to provide more suitable conditions for surgery. Under these conditions, if a relaxant had not been administered, spontaneous muscle movements could occur which would interfere with data collection. Depolarizing agents, such as sux amethonium and decamethonium, act similarly to the normal transmitter at the neuromuscular junction, acetylcholine. When drugs that act in this way are administered to an animal, generalized disorganized muscle twitches (fasciculations) are pro duced before complete skeletal muscle paralysis. Non-depolarizing, or competitive blocking agents do not cause a muscle con traction before producing paralysis. Drugs in this group include tubocurarine, gallamine, pancuronium, alcuronium and vecuronium (Table 4. Since these agents act by competing with acetylcholine for recep to r sites at the neuromus cular junction, their action can be reversed by increasing the local concentration of acetylcholine. This can be achieved by administering drugs such as neostigmine that block the activity of the enzymes which normally break down acetylcholine. It would be possible, but obviously inhu mane, to carry out a surgical procedure on an animal which had been paralysed but was still fully conscious. This will establish that the degree of analgesia and unconsciousness will be sufficient to allow surgery to be carried out humanely. Since considerable individual variation in response to anaesthesia occurs and some inadvertent alteration in the technique can arise, for example due to equipment malfunction, it is also necessary to provide an inde pendent assessment of the depth of anaesthesia. Despite muscle paralysis, twitching of muscles may occur in response to a major surgical stimulus and this indicates that the depth of anaes thesia is inadequate. In humans, pupillary size may alter in response to surgical stimulation, but this sign is of little value in most animals, particularly if atropine has been included in the pre-anaesthetic medication. Changes in blood pressure and heart rate are the most widely used indica to rs of adequacy of the depth of anaesthesia. Dramatic changes in heart rate or blood pressure are believed to indicate a depth of anaesthesia insufficient for the surgi cal procedures that are being undertaken. So despite their widespread acceptance, these parameters may not always be reli able indica to rs of adequate anaesthesia (Whelan and Flecknell, 1992). Although this requires specialist equipment and expert interpretation, these may be available, especially if neurosurgical or neurophysiological studies are being carried out. Various derived measures, for example to tal power and spectral edge frequency have also been used to assess depth of anaesthesia (Murrell and Johnson, 2006; Ot to , 2008); however, these measures generally cannot be used easily with balanced anaesthetic techniques which involve simultaneous use of hypnotics and analgesics. These same difficulties occur in human subjects, and great efforts have been made to develop moni to ring devices that can measure loss of consciousness. Initial studies suggest that the instrument may also be of value in animals (An to gnini et al. The attraction of this moni to r is that it provides a single number as an index of consciousness, or depth of anaesthesia. Given the difficulties of moni to ring the level of consciousness in paralysed animals, a more simple approach is to allow the action of the muscle relaxant to subside periodically.