
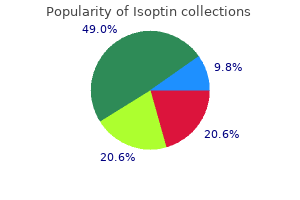
Isoptin
Purchase isoptin 240 mg without a prescription
The axial skeleton includes the skull blood pressure of 80/50 buy discount isoptin line, ribs, sternum, and spine; and the appendicular skeleton includes the extremities. Peripheral skeletal sites are non-central sites, and include the calaneus, tibia, and forearm. Peak bone mass is affected by genetics, mechanical loading, and hormonal and nutritional levels, and is approximately 30% higher in men than in women. After the skeleton reaches its peak bone mass, the bone mass declines throughout life due to an imbalance in remodeling. Estrogen produced by the female ovaries, plus other hormones, regulate the absorption and release of calcium in the bones. After menopause, the ovaries no longer produce estrogen, and bone loss accelerates, finally slowing down at about age 65. When the long-term rate of bone dissolution is greater than the rate of replacement, mineral content slowly decreases, and the bones become thin, brittle, and easily broken. This cycle is called the process of destruction, or resorption, and renewal formation, known as remodeling. In the mature adult, 4 approximately 25% of trabecular bone and about 3% of cortical bone is renewed on an 6 annual basis. The remodeling cycle consists of two distinct stages referred to as resorption and formation. The resorption stage begins when osteoclasts become active on the surface of bones and creates small cavities. The resorption process forms hollows in trabecular bone and cylindrical cavities in cortical bone. The resorption stage is followed by bone formation, during which bone-building osteoblasts fill the cavities with new bone. After formation, the bone returns to a resting state that is referred to as quiescence. Resorption is more rapid than formation, and by age 40 the entire resorption 5 stage may last one month, while the formation stage may take up to 3 months. By age 5 65, the entire process of resorption and formation may take up to 5 months. Modeling and remodeling continues throughout life, so that most of the adult skeleton is replaced 6 about every 10 years, Figure 1-1. Osteoclasts attach to bone surface Osteoclasts attach to bone surface Osteoclasts resorb bone Osteoclasts resorb more bone tissue and leave a deeper resorption cavity Osteoblasts enter cavity and build new bone Osteoblasts build less bone than the amount resorbed Amount of bone formed is equal to the amount Bone resorption exceeds bone formation, of bone resorbed so that bone mass/strength leading to a progressive decline in bone mass, are maintained weakening bones and increasing risk of fractures Fig 1-1. Bone Metabolism Alkaline phosphatase, which raises calcium and phosphate levels, is thought to play a role in bone mineralization. However, many factors influence the bone metabolism and remodeling process by direct action on the osteoblasts and osteoclasts. These glands control the level of calcium in the blood, and are sensitive to small changes in calcium concentration. Calcitriol, 1, 25 dihydroxycholecalciferol, is a hormone formed in the liver and kidneys by the action of enzymes. Calcitriol acts on many different tissues, but its most important action is to increase intestinal absorption of calcium and phosphorus. Vitamin D can be made in the skin through the action of ultraviolet light from the sun on cholesterol. Many people need vitamin D in their diet because they do not derive adequate levels of it from exposure to the sun. Vitamin D deficiency leads to a disease of defective mineralization called rickets in children and osteomalacia in adults. These conditions can cause bone pain, bowing and deformities of the legs, and fractures. Calcitonin is a calcium-regulating hormone produced by cells of the thyroid gland. Calcitonin is thought to be more important for maintaining bone development and normal blood calcium levels in early life. In adults, excesses or deficiencies of calcitonin does not interfere with maintaining calcium concentration or the strength of bone. In females, estrogen acts on the osteoclasts and osteoblasts to inhibit bone 9 breakdown at all stages of life. In males, testosterone is important for skeletal growth 7-8 because of its direct effects on bone and its ability to stimulate muscle growth. Growth hormone from the pituitary gland is also an important regulator of skeletal growth. Thyroid hormones increase the energy production of all body cells, including bone cells. Small amounts are necessary for normal bone development, but large amounts block bone growth. Synthetic forms of cortisol, called glucocorticoids, are used to treat many diseases such as asthma and arthritis. The use of glucocorticoids can cause bone loss due to a decrease in bone formation and an increase in bone breakdown, both of which 1 lead to increased risk of fracture. Bone Strength Bone fractures, especially vertebral compression fractures, present serious consequences following trauma and non-trauma occurrences such as those experienced by those with osteopenia, osteoporosis, and other bone diseases. Living bone tissue is continually changing under the influences of mechanical and hormonal impacts and in response to increased mechanical loading, and may adapt by altering its size, shape, and/or matrix properties. The properties that 7 influence bone strength are related to microarchitectural and macroarchitectural at the cellular and matrix levels. In daily life, the skeleton must withstand a combination of compression or tension forces with bending and twisting motions. The highest stress impacts occur to the vertebral spine due to compression loading. Research has proven that the best bone design to withstand bending loads is when the axis is near the center of the bone. Area moment of inertia is a geometric property that describes the distribution of mass around the neutral bending axis of an object. In essence this means that as the external diameter of a long bone increases, the bone assumes more resistance to bending and twisting loads applied to it, thus reducing potential fractures. The material properties of bone tissue declines with age and is accompanied by a redistribution of cortical and trabecular bone. The process results in an age-related increase in the diameter of long bones with a decrease in cortical 16 thickness. This process was once thought to occur to a greater degree in women; however, research data has demonstrated that both men and women undergo these geometric bone changes with aging. Bone matrix properties of mineralization, collagen characteristics, and microdamage also affect the mechanical properties of bone. The quantity and quality of bone matrix content relates directly to stiffness and strength of bone. When bone matrix is undermineralized or decreases due to a disease state, the ability of the bone to 10 withstand energy impacts decreases. Bone is primarily composed of minerals and collagen which gives bone the ability to withstand energy impacts. Along with adequate bone matrix and 8 collagen, the ability of bone to withstand energy impacts is also dependent upon microdamage. Microdamage or fatigue to bone occurs from the daily physiologic loading to the skeleton. The concept of fatigue microdamage to bone may be related to both 10 age-related fragility bone fractures and certain diseases and conditions. Divisions and Classification of Bones the adult human skeleton consists of 206 bones.
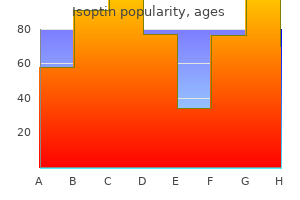
Order isoptin with paypal
Two greater risk of recurrent thrombosis and a three randomized trials in patients with advanced ma fold greater risk of anticoagulant-associated lignancy did not demonstrate any survival ben bleeding heart attack 40 year old female generic 40 mg isoptin visa. Low-molecular-weight heparins compared with un fractionated heparin for treatment of acute deep venous nifcant after adjustment for confounders. A meta-analysis of randomized, controlled a-priori analysis in patients with a life expect trials. The heparin in the initial treatment of venous thromboem beneft was most notable in the subgroup with bolism. Treatment of venous need to be confrmed in further prospective clin thrombosis with intravenous unfractionated heparin ical trials with appropriate designs and power to administered in the hospital as compared with subcu assess cancer outcome before any recommenda taneous low-molecular-weight heparin administered at home. Low-molecular-weight heparin in the treatment of pa tients with venous thromboembolism. Clinical experience with retrievable vena ministered for 3-6 months (level of evidence: cava flters: results of a prospective observational multi center study. Effcacy of low-mo bleeding complications among patients with venous lecular-weight-heparin versus vitamin K antagonists for thromboembolism in relation to both malignancy and long term treatment of cancer-associated venous throm achieved international normalized ratio: a retrospective boembolism in adults: a systematic review of rand analysis. Low-molecular-weight heparin versus a and bleeding complications during anticoagulant treat coumarin for the prevention of recurrent venous throm ment in patients with cancer and venous thrombosis. Eur J Vasc Endovasc weight heparin and coumarin derivatives on the survival Surg 2009;37:349-56. Management of venous thromboembolism cancer surgery: A prospective randomized double-blind in patients with advanced cancer: a systematic review trial. Anticoagulation for the initial treat ing survival in patients with cancer who have no other ment of venous thromboembolism in patients with can indication for anticoagulation. Low molecular weight heparin, ther heparin compared with continuous intravenous heparin apy with dalteparin, and survival in advanced cancer: in the treatment of proximal-vein thrombosis. Laboratory tery interventional procedures, bivalirudin or testing should be performed when there is a argatroban anticoagulation is recommended strong suspicion of Hit (Level of evidence: (Level of evidence: moderate). For postoperative cardiac sur nia: a serious complication of heparin therapy for acute stroke. Risk factors for un favorable clinical outcome in patients with document references ed heparin-induced thrombocytopenia. How frequently treated with subcutaneous unfractionated heparin: a is venous thromboembolism in heparin-treated patients prospective cohort study. The incidence of thrombosis treated with unfractionated or low-molecu recognized heparin-induced thrombocytopenia in a large lar-weight heparin. Heparin-induced thrombocytopenia in dence of thrombocytopenia in hospitalized patients with open heart surgical patients: sequelae of late recogni venous thromboembolism. Arterial and venous complications of Physicians Evidence-Based Clinical Practice Guidelines heparin-induced thrombocytopenia in burn patients. Newer heparin-induced thrombocytopenia, even when anti insights on the mechanism of heparin-induced throm body tests are positive. Mechanisms gery can effectively predict the development of patho of venous and arterial thrombosis in heparin-induced genic heparin-dependent antibodies. Lubenow N, Hinz P, Thomaschewski S, Lietz T, Vogler thrombocytopenia based on broad expert opinion. Amiral J, Bridey F, Dreyfus M, Vissac M, Fressinaud E, diac surgery: predictors and outcome. Greinacher A, Potzsch B, Amiral J, Dummel V, Eichner surgery thromboprophylaxis: the role of non-drug risk A, Mueller-Eckhardt C. Heparin-associated thrombocy factors and evidence for a stoichiometry-based model of topenia: Isolation of the antibody and characterization immunization. A diagnostic test for thrombosis are specifc for platelet factor 4 complexed heparin-induced thrombocytopenia. Heparin-induced thrombocy ness of the platelet aggregation test for the diagnosis of topenia: New evidence for the dynamic binding of pu heparin-induced thrombocytopenia. Greinacher A, Amiral J, Dummel V, Vissac A, Kiefel V, planation for the thrombotic complications of heparin Mueller-Eckhardt C. Amiral J, Wolf M, Fischer A, Boyer-Neumann C, Vissac A, let aggregation test, heparin-induced platelet activation Meyer D. A prospective study on the in therapy in heparin-induced thrombocytopenia with he cidence and clinical relevance of heparin-induced anti patic dysfunction. Anti-heparin/platelet patients with heparin-induced thrombocytopenia and factor 4 antibody optical density values and the con normal or impaired renal function: a single-center ex frmatory procedure in the diagnosis of heparin-induced perience with 68 patients. Validation of the high confrmatory step for the paring desirudin and argatroban in patients with sus diagnosis of heparin-induced thrombocytopenia. Argatroban anticoagulation in patients with dosing requirements of bivalirudin in patients with heparin-induced thrombocytopenia. Bivalirudin during cardi agulation in patients with heparin-induced thrombocy opulmonary bypass in patients with previous or acute topenia. Pharmacokinetic thrombocytopenia or antiplatelet factor four/heparin and pharmacodynamic basis for effective argatroban antibodies. Ar ticoagulant therapy with bivalirudin to assist in the gatroban therapy for heparin-induced thrombocytope performance of percutaneous coronary intervention nia in acutely ill patients. Argatroban anticoagulation invasive strategy: a meta-analysis of randomized clini in renal dysfunction: a literature analysis. A report of 1, 478 clinical outcomes of binant hirudin) for parenteral anticoagulation in pa patients treated with danaparoid (Orgaran) from 1982 tients with heparin-induced thrombocytopenia. Recombinant hiru open-label comparison of danaparoid with dextran 70 din (lepirudin) provides safe and effective anticoagula in the treatment of heparin-induced thrombocytope tion in patients with heparin-induced thrombocytope nia with thrombosis: a clinical outcome study. Greinacher A, Alban S, Drummel V, Franz G, Mueller ment of 51 pregnancies with danaparoid because of Eckhardt C. Fa reduced risk of inducing the immunological type of tal danaparoid-sodium induced thrombocytopenia and heparin-associated thrombocytopenia. Relative son of danaparoid and lepirudin in heparin-induced heparin-induced thrombocytopenic potential of low thrombocytopenia. The pathogenesis of venous duced thrombocytopenia: Clinical considerations of al limb gangrene associated with heparin-induced throm ternative anticoagulation with various glycosaminogly bocytopenia. Treatment options in heparin gatroban to oral anticoagulation with phenprocoumon induced thrombocytopenia. Three of Information about the treatment they received these studies had serious methodological draw during the three-month observation period was backs limiting the clinical applicability of their re available for 597 patients. The analysis included tients, thromboembolic complications occurred in total 2469 patients, 74 and treatment ranged in 58 (10. Similar risk reductions were whether combination therapy may be more ef observed at day 77. Superfcial vein thrombosis in patients with varicose veins: role of thrombophilia 1. Vascular disorders preceding diagnosis of cancer: dis embolism and other venous disease in the Tecumseh tinguishing the causal relationship based on Bradford community health study. Superfcial vein throm ogy, diagnosis and treatment of superfcial-vein throm bosis of lower limbs: infuence of factor V Leiden, bosis. J Vasc bophlebitis and anticardiolipin antibodies report of as Surg 1998; 27:677-80. Hereditary protein S defciency: clinical mani nous thromboembolism: a large, prospective epidemio festations. Martinelli I, Cattaneo M, Taioli E, De Stefano V, Chiuso sis and hypercoagulable states: the evidence. Superfcial venous thrombosis: preva thrombosis of the lower limbs: prospective analysis in lence of common genetic risk factors and their role on 100 patients]. J Am Acad Der after presenting to an emergency department outpatient matol 1990;23:1-18. Operative management of greater saphe phlebitis of the legs: a randomized, controlled, follow nous thrombophlebitis involving the saphenofemoral up study. The son of a low-molecular-weight heparin, a nonsteroidal incidence of deep venous thrombosis in patients with anti-infammatory agent, and placebo in the treat superfcial thrombophlebitis of the lower limbs. Superfcial throm and comparison with a non-steroidal anti-infammatory bophlebitis and deep vein thrombosis. Prevalence of deep vein thrombosis ated heparin for the treatment of superfcial thrombo and pulmonary embolism in superfcial thrombophlebi phlebitis of the leg. A prospective, controlled, random this of the lower limbs: prospective study of 60 cases.

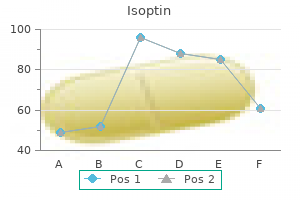
Buy 240 mg isoptin overnight delivery
In pregnant women (factor V Leiden) arrhythmia jokes discount isoptin 40mg on-line, if anticoagulant prophylaxis is not groups, this is a risk factor in determining neural administered during this period. Venous thrombosis of some rare sites include Although in the general population the inci superficial thrombophlebitis and cerebral and mesen dence of thrombophilic defects may be low and the teric veins. Arterial thrombosis including coronary, asymptomatic clinical overview may last for a life cerebrovascular or peripheral circulation is not usual time, higher rates of such mutations in patients with ly associated with hypercoagulable state. However, ve a history of thrombosis show the importance of set nous thrombosis can result from arterial occlusion by ting the correct diagnosis and how the anticoagulant paradoxical embolism through a patent foramen ovale (4, 24) therapy can reduce the risk of recurrent miscarriages. Venous thrombosis is often a chronic condition with recurrence estimated to 5 to 7% annually after the first episode. Goldman-Cecil Medicine, antithrombotic-factor deficient patients (table 2); this 25th Edition, 2016. Inherited antithrombin deficiency causing with heterozygous protein C or protein S deficiency. Inherited antithrombin deficiency: a functioning, their plasmatic levels in patients with in review. Role of antithrombin concentrate in tamin K, and leads to a prothrombotic transient state treatment of hereditary antithrombin deficiency. Folate and homcysteine metabolism states, discrete thrombotic complications seem to be in neural plasticity and neurodegenerative disorders. Reprod markers in spontaneous abortion pathogenesis in parents Biol Endocrinol 2004. Cojocariu Emanuel, Eduard Constantin Radu, Madalina the Longitudinal Investigation of Thromboembolism Iftimie, et al. The 12th Warsaw International currence after deep vein thrombosis and pulmonary em Medical Congres, May 2016. Safety of with common mutation in the methylenetetrahydrofolate reduc holding heparin in pregnant women with a history of venous tase gene: an additional risk factor for neural-tube defects We are not responsible for any adverse medical outcomes as such responsibility lies with the treatng physician. The Hematology or Thrombosis consult services can al ways be consulted for specifc patents with more complex needs. Pharmacy can be consulted as well for help with dosing and monitoring of antcoagulant medicatons. Low Molecular Weight Heparin Enoxaparin (Lovenox) Dalteparin (Fragmin) Tinzaparin (Innohep). Consider lower doses in the elderly, patents with impaired nutriton, liver failure, congestve heart failure, or with a high risk of bleeding. In the absence of any bleeding, the warfarin dose should be adjusted based on the table below. For orthopaedic prophylaxis: 10 mg po qday (14 days for knee replacement/ 35 days for hip replacement). Contraindicated in severe renal failure (CrCl < 30 mL/min), cauton for patents with moderate renal impairment (CrCl 30-50 mL/min). An abnormal thrombin time from dabigatran does not imply that hemostasis is impaired. Indicated in patents with heparin-induced thrombocytopenia who require antcoagulaton. Protamine should be administered over at least 10 minutes to avoid severe hypotension and patents must be monitored for anaphylactoid reactons. Oral vitamin K is the treatment of choice due to its predictable efcacy and to its safety and convenience. Patents should initally be stratfed for stroke risk and bleeding risk to determine appropriate therapy and management. Currently, the oral vitamin K antagonist, warfarin (Coumadin), is the most widely used. An alternatve vitamin K antagonist is nicoumalone (Sintrom), for patents allergic to warfarin. Patents with chronic atrial fbrillaton of unknown duraton, in the absence of an acute embolic event, do not require heparin therapy during the initaton of warfarin therapy. Dabigatran (Pradax), an oral direct thrombin inhibitor, and rivaroxaban (Xarelto), an oral factor Xa inhibitor, are new alternatves to vitamin K antagonists. Both dabigatran and rivaroxaban are as efcacious as warfarin in preventng stroke, with lower risk of intracra nial bleeding. However, they are excreted primarily by the kidney, lack an antdote, and are not readily monitored with standard laboratory tests. Warfarin is recommended for 3 months following open heart surgery, provided the patent reverts to normal sinus rhythm. The duraton of warfarin therapy, regardless of cardioversion outcome, will be decided by the treatng cardiologist. Contnued use of warfarin should be evaluated in Thrombosis Clinic annually, taking into account any new patent-related factors that could alter the risk-beneft balance of long term use of warfarin. Total treatment tme is usually for 3 months but can be extended for up to one year. There is no indicaton to perform thrombophilia screening testng during the acute thrombotc event. It is recommended that thrombophilia testng be performed only by the Thrombosis Clinic. The presence of a thrombophilia will, on occasion although not usually, affect the duration of therapy with warfarin. Patents should complete at least 6 months of antcoagulaton including treatment throughout pregnancy and 6 weeks post-partum. Warfarin is contraindicated during the frst trimester of pregnancy because of the risk of teratogenicity. Primary prophylaxis (with prophylaxis doses of Low Molecular Weight Heparin) is reserved for thrombophilic women during the six weeks post-partum. Antcoagulaton treatment should be contnued indefnitely as long as the malignancy is actve or chemotherapy is ongoing. The role of antcoagulant therapy in women with recurrent fetal loss and other thrombophilias is controversial and such women should be enrolled in currently available clinical trials. In the case of severe renal failure (CrCl 15 30 mL/min), enoxaparin 30 mg sc qday may be used. Other high risk features include the following: 1) Patients who suffer systemic embolism despite adequate anticoagulation with warfarin, 2) Patients with left ventricular dysfunction, 3) Patients with atrial fibrillation, 4) Patients with left atrial enlargement, 5) Patients with caged ball or caged disk valves. Recommended bridging therapy (not needed in low risk patents): Day Day Day Day Day Day 0 Day Day Day 5 4 3 2 1 Surgery +1 +2 +3 D/C warfarin dalteparin 200 units/kg sc qday or enoxaparin 1. Major Orthopedic surgery, other risk factors above risk factors Genitourinary surgery, Neurosurgery, Vascular Surgery, Endoscopy with possibility of biopsy, Abdominal Hysterectomy 27 Note. Patents with severe renal impairment (CrCl <15 mL/min) should receive intravenous unfractonated heparin, as described on page 3, for bridging. The use of combined therapy of warfarin and antplatelet agents (including low dose aspirin) is discouraged due to the higher risk of bleeding in patents on combined therapy. Exceptions include the following: 1) For secondary prophylaxis of ischemic heart disease in patents with coronary artery disease who are under the age of 75. It is not recommended that patents with low ejecton fractons from chronic heart failure be antcoagulated with warfarin unless they have one or more of the following factors: 1. Warfarin therapy is indicated in patents who sufer a cerebrovascular event from a cardioembolic source as evidenced by one of the following risk factors: 1. Other uncommon indicatons for the use of warfarin in the setng of cerebrovascular disease need to be clearly stated by the referring neurologist and can include the following. Central retnal vein occlusion in the setng of a lupus antcoagulant or antcardiolipin antbody 32 11. Argatroban is a second line agent, reserved for patents with severe renal failure (CrCl < 30 mL/min) or for patents who may require acute reversal of antcoagulaton. The goal of this reference is to provide practitioners with an up-to-date, reliable, and easy to use source of information for anticoagulation. The content is based on the latest available evidence-based guidelines and research, whenever possible.
Generic 240mg isoptin free shipping
Santiago 7 itive gastrointestinal neoplasms of differing Ramon Cajal blood pressure 5332 discount isoptin 120 mg otc, a Spanish anatomist, had discov 8 histomorphological and ultrastructural pheno ered this type of primitive nerve cells in the 9 type and biological behavior. This chapter will sum mutations in the exon 11, relevant mutations are 2 marize the current understanding of the pathol suspected on other loci as well. Five-year-survival was 28 and 29% 5 In addition, other mesenchymal tumors unre respectively. These include desmoid 9 tumors, in ammatory broid tumors, myo Little is known about gastrointestinal schwan 4011 broblastic tumors and invasive retroperitoneal nomas. They represent the microscopy often is necessary to con rm diag 7 majority of mesenchymal tumors of the esoph nosis. In 6 Western countries the incidence of mesenchy 7 mal malignomas of stomach and small bowel 8 has been estimated as 1. Transversal computed tomography a and intraop 3 erative macrophotograph b demonstrating an extraluminal 4 pediculate leiomyosarcoma of the stomach in a male patient. Esophageal enema demonstrating leiomyoma, 3 8 cm in diameter, in a 60-year-old female patient. Patients may present can determine tumor site and extent of tumor 8 with recurrent abdominal pain, acute bowel growth. Pylorus preserving partial duodenopancreatectomy 4011 was performed for palliation b. However, some other hand, surgical tumor removal is manda 5 peculiarities of tumor biology may allow a mod tory. The 5 evident tumor remission had lasted for 11 6 Duodenum months at the time of publication. Early demonstrates a broad variability at all gastroin 1 experience with systemic treatment using the testinal locations. Thompson 9 1011 1 2 3 4 5 6 7 8 9 2011 artery, is a branch of the coeliac axis, and its 1 Aims venous drainage, via the splenic vein, is through 2 the portal venous system. Between 14 and 30% 3 To identify the origin of splenic neo of individuals have accessory splenic tissue, 4 plasms. Like lymph nodes, 9 the spleen also has immune functions including 4011 Introduction antibody production, cell-mediated responses 1 and phagocytosis. Presentation clinically in 75% of 1111 Differential Diagnosis patients is with abdominal pain, the remainder 2 through spontaneous rupture, or through 3 Space-occupying lesions in the spleen may be symptoms of hypersplenism such as anaemia, 4 classi ed as cystic, cystic/solid or solid (Table thrombocytopenia or a consumption coagu 5 16. There are two 9 Haemangiomas are the most frequently occur 2011 types depending on the cell of origin. The genital in origin and arise from sinusoidal 4 connective tissue elements give rise to epithelium. Most often, They contain vascular and histiocytic elements 4011 a solitary well-de ned haemorrhagic nodule and most often form multiple nodules within 1 is found, though the spleen may be diffusely the spleen although a focal form is described. Although the overall risk of 8 spontaneous rupture in leukaemic patients 9 is 1%, this is the single commonest cause of 1011 spontaneous splenic rupture, especially in acute 1 leukaemias. The pattern of splenic 4 involvement follows the migratory pathway of 5 the normal benign cellular counterparts. They rarely occur in the this is a low grade B-cell malignancy that 9 spleen and are usually asymptomatic. Micro 3 uation lesions, which are non-enhancing on scopically, only the red pulp is in ltrated in con 4 injection of intravenous contrast. Microscopically, Lymphomas are malignant tumours of the 1 they are composed of vascular and stromal ele lymphoreticular system that are classi ed in 2 ments [7]. Splenomegaly may 4 are noted in lymphoma from reactive enlarge also be observed as a secondary effect without 5 ment to lymphomatous replacement of its malignant in ltration. The commonest 7 later involvement is with scattered foci and form is the low grade type, in which miliary 8 architectural destruction. A spleen over 400 g in in ltration usually occurs, and the second com 9 weight is always histologically in ltrated and monest, the large cell type, in which solitary or 3011 multiple masses are usually found. Expansion 1 by in ltration occurs in the white pulp, partic 2 ularly with low grade lymphoma. Theoretically, 5 this is thought to be because the microenviron 6 ment of the spleen is not favourable to the 7 growth of tumour cells, or because of the lack 8 of afferent lymphatics to the spleen, or the sharp 9 Figure 16. Most often it occurs in the presence of 1 infiltration of the spleen and para-aortic lyphadenopathy. The practice in general from gastric 2011 between benign and malignant lesions in the cancer is to avoid splenectomy unless speci 1 spleen [17]. However, it cannot detect disease 4011 spleen is often ressected in continuity with in normal size nodes (micronodular involve 1 the bowel to achieve a curative margin. The resulting protection 1111 relative to normal spleen on a T2-weighted lasts at least 5 years though the exact duration 2 image, and all demonstrate heterogeneous is unknown. In the presence of coagulopathy due to 5 thrombocytopenia, perioperative platelet trans 6 fusion may be required. In cases where the 7 platelet count is very low (<20 109/l), such 8 Indications for transfusion may only be effective once the vas 9 Splenectomy (Table 16. Occasionally, for lymphoma or cation and the degree of splenomegaly and asso 7 leukaemia, where the spleen involvement is ciated conditions such as portal hypertension. The 3 splenectomy en-bloc to achieve a curative resec paramedian incision may give better access to 4 tion (see above). Symptomatic enlargement the spleen, but it is less useful if the spleen is 5 producing abdominal pain and fullness, and massive or other procedures such as cholecys 6 hypersplenism (anaemia, thrombocytopenia tectomy are contemplated. Initial ligation of 7 or consumptive coagulopathy) may also be indi the splenic artery through the lesser sac may 8 cations for splenectomy [22]. Thereafter the spleen can be safely 1 immobilised by division of the splenorenal lig 2 ament. The chosen 5 the patient should be immunised against pneu approach is the preference of the operating 6 mococcal, Haemophilus and meningococcal surgeon. The operating time for laparoscopic of deep vein thrombosis and speci c anti 6 splenectomy is greater than for open splenec thromboembolic prophylaxis is not indicated in 7 tomy, although the newer technique is in its rel patients undergoing splenectomy [29]. There is a comparable incidence Portal vein thrombosis may occur, particu 9 of the numbers of accessory spleens found larly after splenectomy for massive spleno 1011 during the procedure. Clinically it presents with 9 shock, coma, coagulopathy and adrenal haem 2011 orrhage. It usually occurs within 3 2 is often placed at the time of splenectomy, years after splenectomy, but has been described 3 though there is no evidence that this reduces the up to 30 years later. The available for children between 2 months and 2 2 hazard of overwhelming infection is greatest in: years. It is therefore the responsibil A therapeutic dose should be taken in the event 3011 ity of the individual clinician to take appropri of any illness with shivering, fever or malaise. Doctors attending any asplenic patients with 2 severe infection should give parenteral ben 3 zylpenicillin and arrange hospital admission. Give the differential diagnosis of space 4 ticular importance after laparoscopic splenec occupying lesions of the spleen. A card issued by the Department of Health for patients to carry after splenectomy. Laparoscopic splenec 2011 with peripheral thrombocytopenia: a report of six cases. Strategies 6 metastases from colorectal carcinoma: report of a case to decrease the risk of infection. Ultrasonographic ment of infection in patients with an absent or dysfunc ndings and differentiation of benign and malignant tional spleen. Chasty 1 2 3 4 5 6 7 8 9 2011 Oesophageal lymphomas form less than 1% 1 Aims of oesophageal tumours although the oesopha 2 gus can be involved by gastric lymphoma at the 3 To describe the types of lymphoma of the cardia.
Diseases
- Melhem Fahl syndrome
- Bronchogenic cyst
- Tungiasis
- Chudley Lowry Hoar syndrome
- Leiner disease
- Pituitary dwarfism 1
- Vitamin E deficiency
- Atresia
- Idiopathic infection caused by BCG or atypical mycobacteria
- Sarcosinemia
Buy isoptin 120mg low cost
However blood pressure chart keep track buy isoptin 240 mg, long-term use of these signaling could be responsible for the less ef cient response of hormones may increase the risk for the development of infection, females to corticosteroid therapy [735]. Thus, more personalized in ammatory activity taking place in peripheral tissues such as the treatment strategies taking into account sexual dimorphism may ocular surface. The balance between the production central nervous and peripheral endocrine systems, and translates of cortisone and cortisol is a key point in the control of the events these inputs into signals to the anterior and posterior pituitary leading to activation of innate and adaptive immune responses and (hypophysis) gland. Primary cultures of human corneal epithelial cells, bro modulate the growth, differentiation and function of the lacrimal blasts and allogeneic macrophages (M1) have been shown to be gland [360, 616, 737e740], and to play a direct or indirect. The extent of lacrimal gland alterations following interrup hypothalamic-pituitary axis in general, and speci c pituitary hor tion of the hypothalamic-pituitary axis is often signi cantly greater mones in particular, on ocular surface and adnexal tissues in health in males than in females [91, 743]. The effects of growth tuitary dysfunction on lacrimal tissue appears to be attributed to a hormone are described in Section 3. Impact of interrupting the hypothalamic-pituitary axis guinea pigs [746] is due to hormones from the anterior pituitary. Most information concerning the impact of the hypothalamic Such extracts also promote the proliferation of human meibomian pituitary axis on the ocular surface and adnexa relates primarily gland epithelial cells [747]. For comparison, the administration of poste itary ablation, or interruption of the hypothalamic-pituitary rior pituitary hormones to rabbits had no impact on lacrimal gland connection, as well as in dwarf mice with de cient pituitary func secretion [408]. These conditions cause a functional castration and reportedly Of particular interest, many but not all [745] androgen effects on erase sex-associated differences in the lacrimal gland and induce the lacrimal gland are critically dependent upon an intact cytoplasmic vacuolar metamorphosis, nuclear pyknosis, acinar hypothalamic-pituitary axis. Further, whereas acinar epithelial cells may immune system in vivo is almost completely inhibited by prior contract following anterior pituitary disruption, the density of anterior pituitary ablation or hypophysectomy [529]. Some of the down-regulate the prolactin receptor gene in the lacrimal gland underlying factors may be the signi cant decrease in the androgen may be one mechanism by which androgens suppress in amma receptor protein expression in acinar epithelial cell nuclei [97], as tion in this tissue in Sjogren syndrome [351]. The reason for this linkage However, if the pituitary is transplanted to the kidney capsule, is unknown. Prolactin fragments, in turn, have been reported to androgen therapy increases the acinar complex area in lacrimal inhibit corneal angiogenesis [773]. The mechanism(s) underlying these androgen actions are involved in the control of constitutive proteins by the lacrimal remain to be determined. Thus, the in uence of interrupting the hypothalamic gland weight in orchiectomized rats [417]. Androgentreatment also pituitary axis on androgen target organs appears to be site-speci c. The effects of growth hormone are described lacrimal glands of pituitary-de cient mice [616]. However, prolactin have been positively correlated with central corneal thickness has also been demonstrated to exert no effect on the morphology [782]. Also, exposure to increased prolactin ability to in uence corneal regeneration [790] and the mitotic in levels, induced by metoclopramide treatment, leads to a structural dex of corneal epithelium [791]. Prolactin and its receptor are transcribed and translated in lacrimal gland acinar epithelial cells [750, 752, 753, 755e761]. Treatment with prolactin, prolactin an lacrimal glands in male, but not female, pituitary dwarf mice [616]. It is possible that lacrimal and/or are mediated through the regulation of other hormones. This question is very relevant for patients of this hormone and its receptors are regulated by androgens in with hypothalamic hypogonadism, which was found associated other sites [764e767]. The authors of that case report proposed that this lid levels and tear function [768]. These receptors are thought to be the target for au lacrimal synthesis of prolactin may act to promote autoimmune toantibodies in thyroid-associated ophthalmopathy, and, possibly 310 D. This may contribute to epithelial compromise and tissue growth, differentiation and repair. These actions are crucial the pathogenesis of ocular surface complications reported in for the health and functions of lacrimal gland, meibomian gland diabetes [824]. Insulin has also been found to promote corneal and ocular surface tissues as detailed below. However, the and selenium in the culture media of rat lacrimal gland acinar cells, cross af nity for the receptor is 100e1000 times lower than that induces secretion of secretory component, a protein that binds and of the speci c molecule, depending on cell type [807e809]. The absence of insulin also sues [364, 810e815], and there is evidence of in uences on tissue increases the expression of oxidative markers such as malondial development, and wound healing responses. Insulin resistance is observed in post a slightly lower tear lm breakup time (9. Among them are polycystic ovary syn adnexa drome, pregnancy, anti-androgen therapy and complete androgen 3. Interestingly they estrous cycle change insulin receptor levels or early signaling steps also present with changed levels or impaired action of sex hor in the rat lacrimal gland [73]. These sex-related differences are attrib higher levels of pro-in ammatory cytokines and other markers of uted to sex hormones [524, 848]. Therefore even in type I tion of corneal epithelial cells and broblasts [884e888], differ diabetes, lacrimal gland dysfunction has a signi cant hormonal and entiation of limbal stem cells [889, 890], and the proliferation of metabolic component, plus a possible cross-reactive autoimmune corneal endothelial cells in vitro [891e893]. These ndings are summarized in Table 9 proteins, and are reported to worsen with longer duration of dis [911, 914e930]. In fact, it is often used off-label to promote skin healing the target tissue concentration of insulin [937e939]. Moreover, Sjogren syndrome, a disease ten times differentiation in corneal wound repair in a mouse model of me more frequent in females is commonly associated with thyroid chanical cornea injury [943]. These events taken together indi cate that female sex and/or female sex hormones predispose to 3. Thyroid hormone regulation of the ocular surface and adnexa in ammatory events in the thyroid gland and related target tissues. It has been postulated that the gender composition of the infection [964, 965], quality of life for epilepsy patients [966, 967], patienteclinician dyad could affect communication, shared referrals for cardiac rehabilitation [968], access to and care-seeking decision-making, and other aspects of health care, but the answer is behavior for mental health services [969, 970], quality of life and still not clear. For example, a patient-level meta-analysis by Wyatt long-term outcomes of stroke survivors [971], and care provided et al. Sex and gender in uence the experience and treatment of pain immune diseases are more prevalent in women than in men [33]. This relationship holds true even for conditions children and adolescents [988, 989]. Various explanations for this phenomenon have been given, ranging from experiential and so Trachoma and onchocerciasis, the rst and second leading ciocultural gender differences inpain experience between men and causes of infectious blindness in the world, are classic examples of women to hormonally and genetically driven sex differences in gender-based health issues. Having lower pain thresholds and trachoma is common, women are three times more likely than men tolerances. Women have more physical contact with care providers should take into account the role of gender when people who are infected, putting them at greater risk of exposure. Onchocerciasis in contrast, disproportionately af complain of pain, and their methods for coping with pain fects men compared to women. Many polluted rivers, where the parasitic disease spreads via an insect studies in animal models have demonstrated sex-speci c differ vector [33]. Another group reported by using both sign and symptom data; sex-speci c differences in pain response by dopamine in the bed Use the term sex in most studies of nonhuman animals; nucleus of the stria terminalis in rats [994, 995]. Yet another study Include sex as a variable in basic and clinical research, and take revealed increased heat sensitivity and decreased cold sensitivity donor sex into account in experiments with cultured cells; for female rats, but not males that underwent injections of quis Select animal models for research that mirror human sex dif qualic acid into the thoracic gray matter or sham operations. One studyexamining chronic Elucidate the roles of the sex chromosome complement. Also, the gender of the clinician moderated the pain in ammatory ocular surface disorders; judgments that accounted for the effect of pathology ndings and Use functional neuroimaging. However, further studies are required to clarify the precise nature, extent, and mechanisms of these sex, endocrine David Sullivan: Allergan (F), Novagali/Santen (F), Cempra (F), and gender effects on the eye in health and disease. Therapeutics need to: (C), Dompe (R), Sano Fovea (R), Novartis (R), Laboratoire Thea (R), 316 D. Gender andage-related Aragona: None, Janine Clayton: None, Juan Ding: None, Blanka differences in corneal topography. Ulrike Hampel: Bausch and Lomb GmbH (F), Optima Phamazeuti Exp Eye Res 2009;88:334e8. Prevalence and Essilor (F), Johnson and Johnson Vision Care (F; R), Ocular Dynamics associations of dry eye syndrome in an older population: the Blue Mountains (F), Oculus (F), Ocusense (F), TearScience (F), Visioneering Tech Eye Study.
Order genuine isoptin online
The steps include: maintaining a normal weight blood pressure medication pregnancy cheap isoptin 40mg fast delivery, stopping smoking and being physically active. Comprehensive Stroke Center Cerebral vein and cerebral venous sinus thrombosis 8 What do my family members need to know Your siblings, children and parents need to know they have a slightly higher risk for blood clots, because you had a clot. In that case it might be appropriate to consider testing them for the same clotting disorder. A statement for healthcare professionals from the American Heart Association/ American Stroke Association. Text adapted from Clot Connect: Cerebral vein and cerebral venous sinus thrombosis. It does not replace medical advice from your health care provider because your experience may differ from that of the typical patient. Talk to your health care provider if you have any questions about this document, your condition or your treatment plan. Comprehensive Stroke Center Cerebral vein and cerebral venous sinus thrombosis 9. Restng blood fow (pre-infaton) l Sof garment material provides optmal patent comfort and maximises wear tme. Restng blood fow (pre-infaton) three of the inflated chambers deflate simultaneously. Restng blood fow (pre-infaton) adjustable comfort control when using calf or calf compression to be used at the same thigh garments, for optimum therapy, comfort and system is used time so both lower patient compliance. Augmentaton in blood fow during calf-thigh garment infaton disposable to reduce the risk of cross infection between patients. Velcro fastenings allow full adjustability of fit, congestive heart failure; pulmonary oedema; active infections; local at the femoral vein of a healthy, 40 year old male volunteer test ensuring optimum comfort and therapy. Asian venous thromboembolism l Venous thromboembolism is the term used to describe a blood clot guidelines: prevention of venous thromboembolism. American College of Chest Physicians Evidence-Based Clinical Practice l An embolism occurs when some or all of the blood clot breaks of Guidelines. Inhibition of tissue factor pathway during intermittent pneumatic compression: A possible mechanism for antithrombotic effect. The fibrinolytic effects of intermittent pneumatic compression: mechanism of enhanced combined, and more than twenty fve tmes the number of fibrinolysis. House of Commons Health Committee (2005) the prevention of comparable to those in Western populatons. Every care has been taken to ensure that the information contained in this brochure was correct at the time of going to press. However, Talley reserves the right to modify the specification of any product without prior notice in line with a policy of continual product development. Bridging anticoagulation these risks when scheduling patients for spinal procedures. Consider the benefts and risks before neuraxial intervention in patients anticoagulated or to be anticoagulated [see Warnings and Precautions (5. Reversal of Anticoagulant Effect the most common reason for treatment discontinuation in both studies was for An agent to reverse the anti-factor Xa activity of apixaban is available. Protamine sulfate and vitamin K are not expected to affect the anticoagulant activity of apixaban. Bleeding events were counted during by traumatic or repeated epidural or spinal puncture. If traumatic puncture occurs, delay treatment or within 2 days of stopping study treatment (on-treatment period). If neurological blood cells, bleeding at a critical site: intracranial, intraspinal, intraocular, pericardial, intra compromise is noted, urgent diagnosis and treatment is necessary. Prior to neuraxial articular, intramuscular with compartment syndrome, retroperitoneal or with fatal outcome. Any type of hemorrhagic stroke was adjudicated and counted as an intracranial major bleed. The 95% confdence limits that are shown do not take into account how many comparisons were made, nor do they refect the effect of a particular factor after adjustment for all other factors. Major 22 18 9 14 11 22 Prophylaxis of Deep Vein Thrombosis Following Hip or Knee Replacement Surgery (including (0. Events associated with each endpoint were counted once per subject, but subjects may have Table 4: Adverse Reactions Occurring in 1% of Patients in Either Group contributed events to multiple endpoints. Adverse reactions related to bleeding occurred Blood and lymphatic system disorders: thrombocytopenia (including platelet count in 219 (13. Published data describe that women with a previous history of venous thrombosis are at Gastrointestinal disorders: hematochezia, hemorrhoidal hemorrhage, gastrointestinal high risk for recurrence during pregnancy. Reproductive system and breast disorders: vaginal hemorrhage, metrorrhagia, Labor or delivery menometrorrhagia, genital hemorrhage All patients receiving anticoagulants, including pregnant women, are at risk for Vascular disorders: hemorrhage bleeding. Consider use of a shorter acting Eye disorders: conjunctival hemorrhage, retinal hemorrhage, eye hemorrhage anticoagulant as delivery approaches [see Warnings and Precautions (5. Oral administration of apixaban to rat dams from increase exposure to apixaban and increase the risk of bleeding. Animal Data Maximal plasma concentrations were observed after 30 minutes following a single 7. The concentrations of apixaban in animal milk decrease exposure to apixaban [see Clinical Pharmacology (12. Apixaban has the following 65 years of age and older, and >31% were 75 years of age and older. No clinically signifcant differences in safety or effectiveness were observed when comparing subjects in different age groups. CrCl <15 mL/min; therefore, dosing recommendations are based on pharmacokinetic 12. No dose adjustment is required in patients with mild hepatic impairment (Child-Pugh class A). An agent to reverse the anti-factor Xa activity of Pharmacodynamic Drug Interaction Studies apixaban is available. Pharmacodynamic drug interaction studies with aspirin, clopidogrel, aspirin and clopidogrel, prasugrel, enoxaparin, and naproxen were conducted. No pharmacodynamic interactions were observed with aspirin, clopidogrel, or prasugrel [see Warnings and Precautions (5. However, in patients with moderate hepatic impairment, there is no clear understanding of the impact of this degree of hepatic function impairment on the coagulation cascade and its relationship to effcacy and bleeding. In studies conducted in healthy subjects, apixaban did not meaningfully alter the pharmacokinetics of digoxin, naproxen, atenolol, prasugrel, or acetylsalicylic acid. At doses impairment on the pharmacokinetics of apixaban are summarized in Figure 3. Following oral administration of 10 mg of apixaban as 2 crushed 5 mg tablets suspended in 30 mL of water, exposure was similar to that after oral administration Figure 3: Effect of Specific Populations on the Pharmacokinetics of Apixaban of 2 intact 5 mg tablets. Metabolism Approximately 25% of an orally administered apixaban dose is recovered in urine and feces as metabolites. O-demethylation and hydroxylation at the 3-oxopiperidinyl moiety are the major sites of biotransformation. Unchanged apixaban is the major drug-related component in human plasma; there are no active circulating metabolites. Biliary and direct intestinal excretion contributes to elimination of apixaban in the feces. Apixaban is a substrate of transport proteins: P-gp and breast cancer resistance protein. Figure 2: Effect of Coadministered Drugs on the Pharmacokinetics of Gender: A study in healthy subjects comparing the pharmacokinetics in males and Apixaban females showed no meaningful difference.
Purchase isoptin with amex
Pepsin damage is characterized by focal areas of discontinuity in the adherent mucus layer arteria hepatica propia discount isoptin 40 mg, localized hemorrhagic punctuate ulcers with bleeding into the lumen, and no evidence of reepithelialization or mucoid cap formation (Allen & Flemstrom, 2005). Thus, the unstirred mucus gel layer is also a physical barrier to luminal pepsin accessing the underlying mucosa. Therefore, a dissipation of the mucus gel and phospholipid layer by ulcerogenic substances (such as aspirin and bile salts) leads to both acid back-diffusion and mucosal injury. Moreover, if some oxygen radicals are generated in surface epithelium containing mucus, intracellular mucus could scavenge them, acting as an antioxidant and thus reducing mucosal damage mediated by oxygen free radicals. Even when cells containing mucus are damaged by extracellular oxygen radicals, intracellular mucus may be released into the gastric tissue and prevent additional damage by scavenging them (Seno et al. The efficacy of protective properties of the mucus barrier depends not only on the gel structure but also on the amount or thickness of the layer covering the mucosal surface (Penissi & Piezzi, 1999; Repetto & Llesuy, 2002). The thickness of this layer is the result of a dynamic balance between its secretion and its erosion mechanically by shear forces of the Gastric Ulcer Etiology 5 digestive process and by proteolytic degradation, particularly from luminal pepsin in stomach. Compared with other gastrointestinal secretions, the adherent mucus gel form is physically unique. Studies have shown that adherent mucus gels from stomach, duodenum, and colon are all well-defined viscoelastic gels that do not dissolve on dilution (Allen et al. In functional terms, these recognized properties contribute to the adherent mucus gel layer forming a continuous and effective protection over the mucosa (Allen & Flemstrom, 2005) the mucus bicarbonate barrier is the only preepithelial barrier between epithelium and lumen. When it is overwhelmed or breaks down in different disease conditions, the next series of protective mechanisms come into play, including epithelial repair, and maintenance and distribution of mucosal blood flow (Tulassay & Herszenyi, 2010). This epithelial barrier serves to separate the digestive lumen from the internal compartments of the organism. Its main role is to maintain a selective exchange of different substances (secretions, nutrients, etc. In this context, two crucial elements of the digestive epithelial barrier assure these functions: the epithelial cells and the intercellular junctions (tight junctions). Both structures provide two pathways for transepithelial transport: transcellular and paracellular routes, respectively (Figure 1). Because of the presence of phospholipids on epithelial cells surfaces, these cells are hydrophobic and therefore repel acid and water soluble damaging agents (Lichtenberger et al. The paracellular pathway seems to be the major route of transepithelial macromolecular permeation. This route is a complex array of structures that are mainly controlled by tight junctions between epithelial cells, which appear to be key regulators of gastrointestinal permeability to macromolecules such as endotoxin and other bacterial products. However, this dynamic gateway is able to change its size under various physiological and pathological conditions. For instance, an earlier study (Madara, 1983) showed that increases in guinea pig intestinal transepithelial resistance induced by osmotic loads were accompanied by alterations in absorptive-cell tight junction structure. This alteration in intestinal permeability after meal ingestion enhances the ability of the small intestine to harvest the maximal amount of nutrients, as well as also increase the risk of exposure to luminal proinflammatory compounds. Heat shock proteins generated by gastric epithelial cells are essential for the maintenance of cellular homeostasis during normal cell growth and for survival during various cellular stresses, such as increased temperature, oxidative stress, and cytotoxic agents, preventing protein denaturation and protecting cells against injury. Activation of heat shock protein response is one of the mucosal protective mechanisms of the antacid hydrotalcite. Also, cathelicidin and defensins are cationic peptides that play roles in the innate defensive system at mucosal surfaces preventing bacterial colonization. These elements have been demonstrated in gastric epithelial cells, and they accelerate ulcer healing (Tarnawski et al. They regulate reepithelialization by stimulating cell migration and exert mucosal protective action from a broad range of toxic chemicals and drugs (Laine et al. Maintenance of epithelial integrity requires a precise balance between cell proliferation and cell death. Thus, the epithelium is continually renewed by a well-coordinated and controlled proliferation of progenitor cells that enables replacement of damaged or aged surface epithelial cells. In this context, the gastric epithelium is populated by a variety of functionally-mature cells derived from proliferation of stem cells, such as mucous cells in the stomach, which show rapid turnover rates, and die within only a few days after their formation. Both peptides stimulate epithelial cell proliferation in case of injury as well as also enhance mucus secretion and inhibit acid production in the stomach (Murphy, 1998; Laine et al. However, after superficial injury, restitution of the surface epithelium occurs within minutes by migration of preserved epithelial cells located in the Gastric Ulcer Etiology 7 neck area of gastric glands. Such migration precedes and is independent of proliferation of progenitor cells, which occurs hours after injury (Lacy & Ito, 1984; Blikslager & Roberts, 1997; Laine et al. Particularly prostaglandin E2 and prostacyclin have long been known to have "cytoprotective" effects on the gastrointestinal epithelium and therefore they can be crucial for the maintenance of the gastric integrity. In fact, it is well established that inhibition of their synthesis results in the reduction of gastric mucosal blood flow and gastric mucosal damage (Abdel Salam et al. Thus, although the precise mechanism of cytoprotective action of prostaglandins remained unknown, it appears to result from a complex ability to stimulate mucosal mucus and bicarbonate secretion, to increase mucosal blood flow and sulfhydryl compounds and, particularly in the stomach, to limit back diffusion of acid into the epithelium (Tarnawski et al. Also, growth factors stimulated prostaglandin production in rat endometrial cells through a mechanism that involves an increase in cyclooxygenase activity (Bany & Kennedy, 1995). At the level of the muscularis mucosae, most gastric arteries branch into capillaries, which enter the lamina propria and travel upward in proximity to gastric glandular epithelial cells. At the base of surface epithelial cells, capillaries converge into collecting venules (Laine et al. For instance, restitution, a process whereby denuded areas of the mucosa are covered by rapidly migrating cells from adjacent mucosa, depends to a large extent on adequate blood flow (Lacy & Ito, 1984; Guttu et al. Also, exposure of the gastric mucosa to an irritant or acid back diffusion occurrence leads to a marked increase in mucosal blood flow. This increase allows 8 Peptic Ulcer Disease removal and/or dilution of the back-diffusing acid and/or noxious agents and seems to be essential for mucosal defense because its abolition through mechanical restriction of blood flow leads to hemorrhagic necrosis (Holzer, 2006, Laine et al. It is an important biological signaling molecule that influences circulation by regulating vascular smooth muscle tone and modulating systemic blood pressure. Therefore, it has been shown to exert positive effects on mucosal defense in the gastrointestinal system (Berg et al. Consequently, these agents maintain viability of endothelial cells and prevent platelet and leukocyte adherence to the microvascular endothelial cells, preventing compromise of the microcirculation and thus protecting the gastric mucosa against injury (Laine et al. In addition to local mucosal protection factors, gastric mucosal defense is also regulated, at least in part, by the central nervous system and hormonal factors (Stroff et al. Gastric mucosa and submucosal vessels are innervated by primary afferent sensory neurons and nerves forming a dense plexus at the mucosal base. Afferent neurons constitute an emergency system that is requested when the gastric mucosa is endangered by noxious agents. In this sense, interference with any aspect of the sensory innervations impairs the hyperemic response and therefore diminishes resistance of the gastric mucosa to injury (Tanaka et al. Etiologies multiples of gastric ulcer development Despite its robust and multi-faceted nature, many factors directly related to impairment in mucosal defense can alter the epithelial barrier and encourage the formation of mucosal injury, the most important of which are acid secretion, bacteria and their products, non Gastric Ulcer Etiology 9 steroidal anti-inflammatory drugs, alcohol, reactive oxygen species, as well as different chemical compounds. Their effects on the gastric barrier represent important mechanisms of the pathogenesis of gastric ulcers, chronic gastritis and other gastric diseases, which are frequently generated through an imbalance between mucosal aggressive and defensive factors (Figure 2) (Wallace, 1992; Peskar & Marici, 1998; Tulassay & Herszenyi, 2010). With a prevalence of up to 90% in developing populations, this microorganism is the second most common pathogen for human beings. It is a nonsporulating, gram-negative microaerophilic bacilli, spiral-shaped, having one to six polar-sheathed flagellae emerging from one of its rounded ends and a smooth surface (Dye et al. This pathogen multiplies with great efficiency in the hostile environment within the stomach but survives poorly in the gastric lumen. It is mainly found under the mucous layer and in close proximity, or even attached, to gastric superficial epithelial cells, without substantial invasion of host tissue (Dubois, 1995). The initial response to infection is an interaction of the host epithelial cells with the bacteria, however, the pathogenetic mechanisms of chronic infection with H. This enzyme may explain the extraordinary ability of bacteria to colonize the gastric mucosa and survive in an acid environment (Smoot, 1991).
Buy 40mg isoptin amex
E U S a n d M R C P s e e m t o b e t h e m o s t appropriate tests in patients with intermediate risk to Figure 1: Demonstrated a hyperechoic structure with posterior acoustic shadow in distal common bile duct arteria carotis purchase isoptin pills in toronto. This was consistent with distal common bile duct stone Case 9 Tanassanee Soontornmanokul, M. Technical and clinical success rate were Good cystic fluid was observed (Figure 5). Recently celiac plexus neurolysis with bupivacaine and 98% alcohol was injected to this area. No immediate showed a higher rate of pain improvement than celiac 2 complication after procedure. A 42-year-old male patient presented with Diagnosis: frequent fainting for 8 months from hypoglycemia. Figure 1: Demonstrated a homogeneous hypoechoic mass measuring about 9x7 mm in diameter at the tail of pancreas. Unfortunately, the pathology should not be performed in any lesions reaching to showed well-differentiated gastric adenocarcinoma. Subsequently, laparoscopy higher degree of invasion and surgery was more was performed. Endoscopic ultrasound with biopsy of omental mass for cholangiocarcinoma diagnosis in cirrhosis. Endoscopic ultrasound-guided fine needle aspiration of peritoneal nodules in patients with ascites of unknown cause. The mass endosonographically delineate origin of the lesion and th originated from a 4 layer of intestinal wall and was then suggest the most likely diagnosis. Nowadays, mediastinoscopy It revealed a well-defined border hypoechoic mass to gain tissue preoperatively can be avoided by either measuring about 30x14 mm in diameter (Figure 1). The sensitivity, specificity, and positive and proliferation of poorly cohesive small sized mitotically negative predictive values were 71. The cyst had suggestive for malignant cystic neoplasms including mural nodule and thickening wall as shown in Figure 2. This cyst was then diagnosed as amylase in combination with endosonographic features mucinous cystadenocarcinoma. The mass originated from diagnosis of sub-epithelial lesions with low complication nd 2 2 layer of rectal wall. In this case, the patient already had a mucosal neuroendocrine tumor which was proven from the biopsy which showed neuroendocrine tumor. Diagnosis: Rectal neuroendocrine tumor Figure 1: Demonstrated a rectal sub-epithelial mass with a post-biopsy ulcer on the surface of lesion. Figure 2: Demonstrated a homogeneous hypoechoic mass originating from the 2nd wall layer of rectum. Intrabiliary metastasis from colonic adenocarcinoma without tumor growthmay be accompanied with hepatic liver parenchyma involvement: contrast enhanced parenchymal metastasis or, less commonly, the solitary ultrasonography detection. Peroral video polypoid growth of liver metastasis from colonic cholangioscopy using narrow band imaging for adenocarcinoma with minimal invasion of the liver early bile duct cancer (with video). Because of the rapid advances in the medical sciences, the publisher recommends that there should be independent verification of diagnoses and drug dosages. Spinal Pain, Section 1: Spinal and Radicular Pain Syndromes 11 Note on Arrangements 11 Definitions of Spinal Pain and Related Phenomena 11 Principles 14 Radicular Pain and Radiculopathy 15 D. Local Syndromes of the Upper Limbs and Relatively Generalized 23 Syndromes of the Upper and Lower Limbs F. In the third part, the ments to the wording and helped to establish the new opportunity has been taken now, as before, to present format. Notes on visional compilation for scrutiny and correction by all the terms Sympathetically Maintained Pain and who have the expertise and the will to devote some Sympathetically Independent Pain have also been effort to developing this statement of our existing introduced in a separate section, in connection with knowledge of pain syndromes. Serratore have been unfailingly quire new knowledge; and, the adoption of such tax patient and helpful in the production of the manu onomy with the condition that it can be modified will script and in the associated correspondence over sev encourage its use widely by those who may disagree eral years. Bryan Urakawa un been the experience and chronology of such widely ix accepted classifications as those pertaining to heart each as can be obtained, at least with respect to the disease, hypertension, diabetes, toxemia of preg pain. It would be expecting too much and also would nancy, psychiatric disorders, and a host of others. Accordingly, a classification system the spoken and written transfer of information, par for pain syndromes has been attempted which, with ticularly scientific papers, books, etc. Specialist workers in various fields usually timate truth and universal consistency. The Ad Hoc far as we know, but complete consistency is beyond Committee on Headache of the American Medical the hopes of any medical system of classification. Stroke has cation in medicine has achieved such aims, nor can it brought forth a schedule of its own (Capildeo et al. Classification 1977), the American Rheumatism Association (1973) in medicine is a pragmatic affair, and we may con has produced its own system with criteria for diagno sider briefly how classifications can be devised. Clas sis, hematologists have continuously developed the sifications may be natural if they reflect or presume to numbering of clotting factors, and so forth. Alternatively, they may be field of chronic pain, two requirements spring readily artificial but convenient. The first is that we should be able to identify cation into animate or inanimate objects is a natural all the chronic pain syndromes we encounter. With regard to internal medicine, the same ap is used as the criterion for classification. By contrast, a phylogenetic clas Pain syndromes are distinguished particularly often sification by evolutionary relationships is a very supe on the basis of duration, site, and pattern, some of rior form of classification. Here we have aimed espe infectious diseases or neoplasm; by systems of the cially at describing chronic pain syndromes and at body. Chronic disease and hereditary ataxia; (c) extrapyramidal and pain has been recognized as that pain which persists movement disorders. Overlapping three months is the most convenient point of division occurs repeatedly in such approaches to categoriza between acute and chronic pain, but for research pur tion. Those who and abnormal clinical and laboratory findings as R52 treat cancer pain find that three months is sometimes Pain Not Elsewhere Classified. Pain that persists for a given length of time provision for conditions that are not well described would be a simpler concept. This length of time is and which will overlap with others that are well de determined by common medical experience. Thus, in psychiatry we may diagnose stances, chronic pain is recognized when the process operationally from biochemistry (phenylketonuria), of repair is apparently ended. These include rheuma After quite protracted discussion and correspon toid arthritis, osteoarthritis, spinal stenosis, nerve dence, it was agreed that there were a number of pain entrapment syndromes, and metastatic carcinoma. Such changes can make it even including some of the foregoing, have a fairly difficult to say that normal healing has taken place. First a smaller one, important, even if we must understand it slightly dif in which there is recognition of a general phenome ferently as a persistent pain that is not amenable, as a non that can affect various parts of the body, and sec rule, to treatments based upon specific remedies, or to ond, a very much larger group, in which the the routine methods of pain control such as non syndromes are described by location. As it happens, the coding system the present arrangement has been adopted be has always allowed durations to be entered as less cause it offers a particular advantage. That advantage than one month, one month to six months, and more stems from the fact that the majority of pains of than six months. This is probably the best solution for which patients complain are commonly described first the purpose of comparing data within a diagnostic by the physician in terms of region and only later in category, or even between some diagnoses. Each syndrome then was to be not meet one of the above characteristics are omitted. Each colleague approached was asked to exchange his the myofascial pain syndromes have presented or her descriptions with others who were looking at obvious difficulties. Accordingly, the majority of descrip erly validated information with agreed criteria and tions-but not quite all of them-have been scrutinized repeatable observations.