
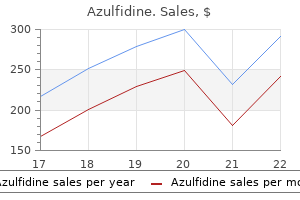
Azulfidine
Buy azulfidine with visa
Palliative care focuses on the management of symptoms and improving quality of life pain treatment center rochester general hospital discount 500mg azulfidine amex, regardless of prognosis. Therefore, palliation may be viewed as an option in those patients who wish to forego life-extending options such as transplantation. Palliative and end-of-life care in cystic fibrosis: what we know and what we need to know. On physical examination, he has a lordotic posture, and there is no scoliosis, sacral hair, or skin abnormalities. His patellar deep tendon reflexes are normal; on plantar stroking, his toes go downward. This suggests a disorder of the spinal cord (a myelopathy) with involvement of exiting nerve roots. Vitamin B12 deficiency causes a myelopathy that affects the posterior columns of the spinal cord. Other causes of myelopathy include mass lesions like hematomas or spinal cord tumors, spinal cord syrinx, trauma, genetic disorders such as hereditary spastic paraparesis, and infections including meningitis, myelitis, and abscesses. Becker muscular dystrophy and spinal muscular atrophy are disorders of the muscle and motor neuron, respectively; they are not typically associated with back pain. There were no reported complications in the operating room and there was minimal bleeding. Physical examination reveals a tired-appearing child in severe respiratory distress. Pulmonary edema, similar to edema in any tissue bed, occurs because of Starling forces favoring filtration out of capillary bed. Pulmonary edema is commonly caused by increased capillary permeability in sepsis and pneumonia, by increased intraluminal hydrostatic pressure in heart failure, and by decreased intraluminal oncotic pressure in hypoproteinemia. Clinical signs of pulmonary edema include rapid, shallow breathing, hypoxia, retractions, and crackles. Another possibility is that positive end-expiratory pressure is required to overcome an upper airway obstruction, and its sudden removal after a corrective therapy favors fluid transudation. Treatment of postobstructive pulmonary edema includes oxygen, diuretics, and in more severe cases, application of positive end-expiratory pressure either noninvasively or with intubation and mechanical ventilation. Congestive heart failure can be a cause of pulmonary edema, but it is less likely for the child in this vignette because there is no hepatomegaly or signs of decreased cardiac output. Surgical bleeding can be a cause of respiratory failure postoperatively after a tonsillectomy and adenoidectomy, but the surgical sites are clean and intact. Upper airway obstruction as a cause of respiratory failure presents with stridor and deep retractions, as opposed to hypoxia, tachypnea, and crackles. Thyroid peroxidase and anti thyroglobulin antibodies are often detectable in Hashimoto thyroiditis, and would likely be positive in this patient. Hashimoto thyroiditis is the most common cause of acquired hypothyroidism and results in autoimmune destruction of the thyroid gland. In addition to those described previously, other common signs and symptoms of hypothyroidism include menstrual irregularities in females, poor linear growth, and weight gain that is usually mild. Thyroid function can be normal in Hashimoto thyroiditis, but the individual remains at risk for hypothyroidism in the future. Other causes of thyroid enlargement include multinodular goiter, iodine deficiency, other thyroiditis, and rarely, thyroid cancer. Thyroid uptake and scan would be diagnostic of Gravesdisease, but not hypothyroidism. A urinary iodine level would be informative only in the setting of iodine deficiency, but would not diagnose hypothyroidism. Physical examination reveals numerous vesicles with red halos on the buccal mucosa. This condition presents most often in children younger than 5 years of age, though it may occur at any age with the first bout of herpes simplex virus. As the lesions progress, many patients develop poor oral intake, drooling, and foul-smelling breath; some may be quite ill-appearing and are at risk for dehydration. Antiviral therapy with oral acyclovir may be considered for those with more serious signs or symptoms, and systemic therapy should be used in immunodeficient patients. Healthcare providers must be comfortable differentiating primary herpetic gingivostomatitis from the other common infectious or benign causes of oral lesions in children. Acute necrotizing gingivitis (trench mouth or Vincent stomatitis) is a painful ulcerative condition that primarily affects adolescents and young adults with poor oral hygiene, immunosuppression, or malnutrition. These usually occur as 1 to 3 shallow ulcers 3 to 6 mm in diameter, with well-defined borders and a small surrounding rim of erythema, and covered with a grayish white membrane. The exanthem consists of gray-white vesicles surrounded by erythema primarily on the palms and soles, and may also involve the buttocks and distal extremities. The enanthem presents as 1 to 3-mm vesicles on an erythematous base involving the buccal mucosa, palate, tongue, uvula, and anterior tonsillar pillars. Herpangina is an enanthem also caused by enteroviral infection, most often seen in children ages 3 to 10 years. Tiny vesicles and erythematous ulcers occur on the posterior pharynx, involving the soft palate, uvula, and tonsillar pillars, and resolve spontaneously within 1 week. Up to 60% of cases of congenital and early-onset hearing loss are caused by genetic factors. Approximately 30% of genetic hearing loss is syndromic; thus, a thorough physical examination is essential in evaluating a child with hearing loss. If the result of this testing is negative, it is appropriate to perform a hereditary hearing loss next-generation sequencing panel that can test for many known nonsyndromic gene mutations in a single blood test. Meningitis is another leading cause of acquired permanent hearing loss, whereas otitis media can result in reversible hearing loss. The isolated finding of a single transverse palmar crease can be seen in normal individuals, but in pediatrics, trisomy 21 must be considered, especially if other associated dysmorphology is present. American College of Medical Genetics and Genomics guideline for the clinical evaluation and etiologic diagnosis of hearing loss. Hearing assessment in infants and children: recommendations beyond neonatal screening. In a study of approximately 2,800 young women with breast disease, more than 98% were of benign etiology. Overall, fibrocystic changes are significantly more common in adolescent girls, but biopsies are rarely performed. The diagnosis is typically made by the combination of physical examination and the appearance of clearly defined, homogeneous, hypoechoic densities on ultrasonography. Most fibroadenomas are less than 3 cm in diameter; giant fibroadenomas are more than 5 cm. Treatment should include coverage for likely skin pathogens (eg, staphylococci, streptococci). Breast cancer is uncommon among adolescents; therefore, both breast carcinoma and phyllodes tumor are unlikely in this scenario. Adolescents with fibrocystic changes in the breast often complain of breast tenderness, with peak symptoms near the time of menstruation. For the girl in this vignette, who does not require specialized academic instruction, the best recommendation would be a regular class for the majority of the day, with services for speech therapy and physical therapy or adaptive physical education for part of the day. Early intervention programs are multidisciplinary, community-based, and family-centered. A service coordinator assists the family with setting up the services and connecting with resources. If the child qualifies for special education services, an Individualized Education Program is developed, outlining the services and accommodations that will be provided to the child to meet his educational needs. This means that the child should be educated in typical educational settings with students without disabilities as much as possible. General education teachers may feel inadequately prepared to provide optimal instruction to students with disabilities. In addition, children with disabilities may need some time in a less inclusive environment to work on nonacademic functional skills. Pediatricians can optimize their identification of children with possible delays by using standardized developmental screening instruments at the American Academy of Pediatrics recommended time points of 9 months, 18 months, and 24 or 30 months of age. His physical examination is significant for marked bruising and swelling over his right eyelid and periorbital area.
Order azulfidine cheap online
Furthermore pain treatment with laser purchase azulfidine 500mg overnight delivery, the number of chemical compounds for which the biological activity is well understood by scientists is a fraction of the sheer number of unidentifed chemical components that have potential health effects (Carpinella and Rai 2009). In particular, when researchers plan on studying traditional medicines, it is important that the advan tages revealed through study are returned to the particular group from which the knowledge is taken (King, Carlson, and Moran 1996). Much emphasis was placed on properly describing the herbal intervention, including name of the herbal medicine, its characteristics, dosage used, and informa tion regarding qualitative testing (Gagnier, Boon et al. N-of-1 trials are prospectively planned multiple crossover trials in an individual participant (Guyatt et al. An N-of-1 approach can help overcome issues of heterogeneity, in effect allowing clinicians to determine whether a product is achieving a benefcial effect in a specifc individual. Given that some herbal medicines have therapeutic abilities equivalent to (and sometimes supe rior to) those of conventional medicine, patients have a wider range of treatment options, which allows for greater patient autonomy. For instance, both cisapride and probiotics have been favorably evaluated for their role in gastrointestinal motility (Muller-Lissner 1987; Nurko et al. However, there are adverse events associated with cisapride (as discussed in Section 21. Saw palmetto is yet another example, as it relieves prostatic symptoms of the urinary tract that are comparable to the effects of fnasteride, a prescription medication used for the same indication (Wilt et al. Numerous weight-loss products have been adulterated with prescrip tion medications like sibutramine, cetilistat, furosemide, or chemicals like phenolphthalein, all of which are only available with a prescription or are illegal to add to health products in an undeclared fashion (U. In a study of 26 herbal medicines taken from a pharmacy in Hong Kong and tested for adulterants, 15 were adulterated with phosphodiesterase V inhibitors, including sildenafl (Poon et al. A recent case in which an herbal medicine tested positively for the presence of microorganisms has confrmed the seriousness of bacterial contami nation. The herbal medicine was also implicated in two cases of liver damage (Stickel et al. In contrast, evidence has yet to show any signifcant safety issues when probiotics are taken by people in good health, even for extended periods (Charrois, Sandu, and Vohra 2006). Herbal therapy may be the preferred choice if it is less harmful than its conventional counterpart. The degree to which a clinician might feel comfortable to support the use of herbal medicine as primary treatment often depends on the seriousness of the situation (Adams et al. For mild or self-limiting illnesses, a clinician might be more willing to tolerate herbal medicine as primary treatment, if it is believed to be safe and it is consistently preferred by patients, even in the absence of compelling effcacy data. A corollary is that the patient must be informed if the herb is not well studied, because the beneft of treating a minor illness may not be worth the potential harm of an unstudied therapy (Adams et al. Risk must be evaluated in a relative fashion, in light of the known safety profle of the herbal medicine and its conventional counterpart, so that the patient can make an informed choice. In cases of moderately severe illness, a clinician might be willing to promote the use of herbals as primary treatment. In contrast, if a patient had a serious or life-threatening illness, the use of herbal medicines as primary treatment would be limited to conditions for which there were no known effective conventional therapies or for which herbal medicines had compelling effcacy data. In each instance, evidence and patient preference should guide decision making in conjunction with clinical judgment. If evidence suggests that the herbal medicine may be effective and with out harm, then it is reasonable for the clinicians to discuss this therapeutic approach with patients (Cohen and Eisenberg 2002). Under these circumstances, when herbal medicine is an adjunct, a clinician may feel comfortable with a lower standard for proof of effcacy than the herbal medicine being used as primary treatment. Examples of adjunct therapy include the follow ing: using butterbur for migraine prophylaxis (Lipton et al. The authors described the effect as a result of the combined anticoagulatory effects of the two prod ucts. In a pharmacokinetic interaction, the absorption, distribution, metabolism, or excretion of one product is affected by another (Baxter and Stockley 2005). Many herbs have been little documented about their pharmacological properties and even less about their potential interac tions with pharmaceutical medications. One challenge that exists is determining which theoretical interactions will be important clinically (Brulotte and Vohra 2008). While research is actively underway to expand the knowledge base regarding herbal medicine safety and effcacy, clinicians are obligated to work with the best available evi dence at the time. Respect for patient autonomy demands that health care pro fessionals be well informed about herbal products in order to provide information (Sugarman and Burk 1998). Interactions supported by clinical evidence (reported in human case reports or clinical trials). Routine inquiry will help promote clinician aware ness of patientsuse of herbal medicines, and a proactive approach is required for nonmalfeasance. Ultimately, research should provide information on effcacy and safety that can be translated into the clinical setting and become useful to patients. No clinician is expected to know all of the possible interactions, but there should be some effort to at least know of common interactions based on frequently used products in their patient population. Fortunately, some universities have already adopted this approach, those belonging to the Consortium of Academic Health Centers for Integrative Medicine. The major focus of the Consortium is to promote integrative medicine-related principles in educational settings; this may be achieved by supporting the forma tion of integrative medicine curricula, research, and potential therapeutic modalities (Consortium of Academic Health Centers for Integrative Medicine 2009a). There are 46 institutions that belong to the Consortium, including Yale University, Johns Hopkins University, and Harvard Medical School (Consortium of Academic Health Centers for Integrative Medicine 2009b). Clinicians will become more aware of therapies that are effective and will be able to offer alternatives to patients, which will help improve patient autonomy and benefcence. Also, health care professionals will be more informed as to what therapies may cause harm for patients, and thus, they can guide patients to avoid these deleterious practices. Patients have a right to choice in treatment, but this right assumes that their clinicians can pro vide them with enough information about their therapeutic options (conventional, complementary, and alternative) for them to do so. To promote full disclosure, clinicians should cultivate respectful rela tionships in which patients know that their preferences, values, and beliefs will be considered when making treatment decisions. With continued research and careful attention to patient-centered care, issues sur rounding the ethical use of herbal medicines will be dealt with in such a way as to promote benef cence, nonmalfeasance, and patient autonomy. Ethical considerations of complementary and alternative medical therapies in conventional medical settings. Management of stimulant medications in children with attention defcit/hyperactivity disorder. Complementary and alternative medicine use among adults and children: United States, 2007. Potential physician malpractice liability associated with comple mentary and integrative medical therapies. American Academy of Pediatrics: Counseling families who choose complementary and alternative medicine for their child with chronic illness or disability. Prescription, over-the-counter, and herbal medicine use in a rural, obstetric population. Task force on complementary and alternative medicine: Provisional section on complementary, holistic, and integrative medicine. Knowledge and attitudes of lay public, pharmacists, and physicians toward the use of herbal products in north Jordan.
Buy discount azulfidine 500 mg on-line
Levetiracetam inhibits burst firing without affecting normal neuronal excitability treatment guidelines for pain management generic 500 mg azulfidine with amex, suggesting that levetiracetam may selectively prevent hypersynchronization of epileptiform burst firing and propagation of seizure activity. When discontinuing therapy, wean the dose gradually to minimize the potential of increased seizure frequency. Capsules cannot be crushed, suspended in water, or dissolved by placing in water before use. Monitor patient closely when switching brand of drug due to some differences in bioavailability. Title Levothyroxine Dose Initial oral dose: 10 to 14 mcg/kg/dose orally every 24 hours. Adverse Effects Prolonged over-treatment can produce premature craniosynostosis and acceleration of bone age. Monitoring After 2 weeks of treatment, serum levothyroxine (T4) concentration should be in the high normal range (10 to 16 mcg/dL) and should be maintained in this range for the first year of life. Assess for signs of hypothyroidism: Lethargy, poor feeding, constipation, intermittent cyanosis, and prolonged neonatal jaundice. Assess for signs of thyrotoxicosis: hyperreactivity, altered sleep pattern, tachycardia, tachypnea, fever, exophthalmos, and goiter. Special Considerations/Preparation 477 Micormedex NeoFax Essentials 2014 Oral suspension is not commercially available. Also available in capsules that contain a viscous liquid ranging from 13 to 150 mcg per capsule. To prepare a 15-mcg/mL levothyroxine oral suspension: Crush levothyroxine 100-mcg tablets in glycerol and add sterile water up to desired volume. Stability tests demonstrated a 12% decline in levothyroxine concentration in the prepared suspension over 11 days. An oral liquid formulation of levothyroxine sodium 25 mcg/mL in 40% glycerol compounded from crushed tablets and distilled water with no preservatives added was stable for 8 days when stored in amber bottles at 4 degrees C. Injectable form is available as lyophilized powder in vials containing 100 or 500 mcg. Product Information: levothyroxine sodium intravenous injection, levothyroxine sodium intravenous injection. Contraindications/Precautions Contraindicated in complete heart block and wide complex tachycardia attributable to accessory conduction pathways [3] [4]. Transformed in the liver to metabolites with antiarrhythmic activity; approximately 30% is excreted unchanged in neonates. Cardiac toxicity is associated with excessive doses and includes bradycardia, hypotension, heart block, and cardiovascular collapse. Special Considerations/Preparation 480 Micormedex NeoFax Essentials 2014 Use only preservative-free lidocaine without epinephrine. Title Lidocaine Antiarrhythmic Dose 481 Micormedex NeoFax Essentials 2014 Initial bolus dose: 0. Later signs include seizures, loss of consciousness, respiratory depression, and apnea. Alteplase, aminophylline, amiodarone, ampicillin, caffeine citrate, calcium chloride, calcium gluconate, cefazolin, cefoxitin, chloramphenicol, cimetidine, dexamethasone, digoxin, dobutamine, dopamine, enalaprilat, erythromycin lactobionate, famotidine, fentanyl, flumazenil, furosemide, glycopyrrolate, heparin, hydrocortisone succinate, insulin, linezolid, methicillin, metoclopramide, micafungin, morphine, nafcillin, nicardipine, nitroglycerin, penicillin G, pentobarbital, potassium chloride, procainamide, ranitidine, sodium bicarbonate, and sodium nitroprusside. The clinically effective dose of 6 mg/kg/hr will lead to accumulation of both lidocaine and metabolites within several hours. Alteplase, aminophylline, amiodarone, ampicillin, caffeine citrate, calcium chloride, calcium gluconate, cefazolin, cefoxitin, chloramphenicol, cimetidine, dexamethasone, digoxin, dobutamine, dopamine, enalaprilat, erythromycin lactobionate, famotidine, fentanyl, flumazenil, furosemide, glycopyrrolate, heparin, hydrocortisone succinate, insulin, linezolid, metoclopramide, micafungin, morphine, nafcillin, nicardipine, nitroglycerin, penicillin G, pentobarbital, potassium chloride, procainamide, ranitidine, sodium bicarbonate, and sodium nitroprusside. Caution: Preterm newborns and term newborns undergoing hypothermia treatment are at risk for drug accumulation due to slower drug clearance. Uses Treatment of severe recurrent or prolonged seizures that do not respond to first-line therapies. Pharmacology the mode of action for lidocaine as an anticonvulsant drug is unknown. Free drug fraction in both term and premature neonates is approximately twice that found in older children because of significantly reduced protein binding by alpha 1-acid glycoprotein. Measuring blood concentrations is not clinically useful except when accumulation is suspected. Special Considerations/Preparation Use only preservative-free lidocaine without epinephrine. References Shany E, Benzaqen O, Watemberg N: Comparison of continuous drip of midazolam or lidocaine in the treatment of intractable neonatal seizures. Compatibilities updated 7/2009 Dose & Administration and References updated 1/2009 Added 3/2006 1. Before administering oral suspension, gently mix by inverting bottle 3 to 5 times. Uses Limited to treatment of infections, including endocarditis and ventriculitis, caused by gram positive organisms (eg, methicillin-resistant Staph. Do not use as empiric treatment or in any patient with infections caused by gram-negative organisms. Contraindications/Precautions Contraindicated in patients with carcinoid syndrome, uncontrolled hypertension, pheochromocytoma, thyrotoxicosis, and/or patients receiving concurrent serotonergic agents, sympathomimetic agents, vasopressive agents, or dopaminergic agents unless monitored closely [1]. Myelosuppression (including anemia, leukopenia, pancytopenia, and thrombocytopenia) has been reported. Symptomatic hypoglycemia has been reported in patients with diabetes receiving insulin. Peripheral and optic neuropathy have been reported in pediatric patients, mainly in patients treated for longer than 28 days. Lactic acidosis has been reported in a case series of 3 children aged 6 months, 6 months, and 16 years receiving linezolid for 53, 31 and 7 days of treatment, respectively. Two patients developed multiple system organ failure and metabolic acidosis, and the third patient developed pressor-refractory shock and metabolic acidosis. Patients in an open-label, randomized trial comparing linezolid with vancomycin, oxacillin, or dicloxacillin in the treatment of seriously ill patients with intravascular catheter-related bloodstream infections had a higher chance of death than did patients treated with any comparator antibiotic, and the chance of death was related to the type of organism causing the infection. Patients with Gram positive infections had no difference in mortality according to their antibiotic treatment. In contrast, mortality was higher in patients treated with linezolid who were infected with Gram negative organisms alone, with both Gram positive and Gram negative organisms, or who had no infection when they entered the study. Pharmacology 489 Micormedex NeoFax Essentials 2014 Linezolid is an oxazolidinone agent that has a unique mechanism of inhibition of bacterial protein synthesis. Serum half-life in most neonates is 2 to 3 hours, with the exception of preterm neonates less than one week of age, who have a serum half-life of 5 to 6 hours [1] [16] [17]. Adverse Effects Elevated transaminases and diarrhea occur in approximately 5% of treated patients; thrombocytopenia and anemia occur in 2% to 5% [2] [8]. Acyclovir, amikacin, aminophylline, ampicillin, aztreonam, calcium gluconate, caspofungin, cefazolin, cefoxitin, ceftazidime, ceftriaxone, cefuroxime, cimetidine, clindamycin, dexamethasone, digoxin, dobutamine, dopamine, enalaprilat, esmolol, famotidine, fentanyl, fluconazole, furosemide, ganciclovir, gentamicin, heparin, hydrocortisone succinate, imipenem/cilastatin, lidocaine, lorazepam, magnesium sulfate, meropenem, methylprednisolone, metoclopramide, metronidazole, mezlocillin, midazolam, morphine, naloxone, netilmicin, nicardipine, nitroglycerin, pentobarbital, phenobarbital, piperacillin, piperacillin-tazobactam, potassium chloride, propranolol, ranitidine, remifentanil, sodium bicarbonate, theophylline, ticarcillin, tobramycin, vancomycin, vecuronium, and zidovudine. Terminal Injection Site Incompatibility Amphotericin B, erythromycin lactobionate, phenytoin, and trimethoprim/sulfamethoxazole. Supplied as ready-to use infusion bags (2 mg/mL); no further dilution is necessary [1]. Uses 492 Micormedex NeoFax Essentials 2014 Limited to treatment of infections, including endocarditis and ventriculitis, caused by gram positive organisms (eg, methicillin-resistant Staph. All 3 children had liver dysfunction and complicated medical courses while receiving linezolid therapy. The role of linezolid in the development of lactic acidosis in these patients is unknown [6]. Safety and efficacy of linezolid therapy for greater than 28 days has not been evaluated in controlled clinical trials [1]. Pharmacology Linezolid is an oxazolidinone agent that has a unique mechanism of inhibition of bacterial protein synthesis. The majority of patients had 493 Micormedex NeoFax Essentials 2014 received linezolid previously [14] [15] [9]. Monitor lactate concentrations in patients receiving extended courses of linezolid therapy or in patients with pre-existing hepatic or renal dysfunction [6].
Buy discount azulfidine 500 mg on line
A third problem in assessment of executive functions is the failure of laboratory testing to re ect problems in cog nition or behavior as they are manifested in everyday Executive Functions: the Need life pain sacroiliac joint treatment azulfidine 500mg for sale. Executive functions are dynamic, and unlike eval for Subcategories uation of more speci c functions such as motor skills, problem-solving behavior that includes planning or decision making is more difficult to fully capture in Executive functioning is a multifactorial rather than a controlled environment [63, 84, 103]. Given the diversity of the frontal patient errors when performing everyday activities are systems underpinning the executive functions, no one less likely to be manifested in the laboratory than they test can be sensitive to all aspects of dysfunction are in the natural setting [104]. In general, subdivisions that capture both the cog errors of action in performing basic everyday activities nitive and the behavioral/emotional aspects of exec such as making coffee, toast, packing a lunch, etc. The utive functions are emphasized because they provide necessary items for a particular task are placed on a the necessary framework for a systematic evalua table in a standardized fashion in front of the patient, tion strategy [80, 97]. Assessment of executive func who is then instructed to complete it, and performance tioning must therefore include measures of the cog is observed and errors are recorded. Competing stimuli can also be and biases in judgment in problem solving, ability to introduced to increase complexity. Morris Accurate assessment of executive functioning that from the acute confusion, delirium, and/or posttrau encompasses all frontal systems will best be accom matic amnesia can be a slow, nonlinear process. When evalu motivation, and using tasks that assess errors of action ating the executive functions multiple procedures will in a more natural environment. Supplementation with be required, including self-reports, naturalistic obser more experimental procedures such as ToM tasks may vation or tasks measuring everyday action errors, tasks also be indicated. Use of multiple measures that re ect the different frontal circuits will be neces sary. Consequently, the neuropsychological evaluation should be dynamic in terms of being ex Summary ible and accommodating to the emergent cognitive and behavioral changes marking the phases of recovery. Briefer testing of causing long-term disability in a signi cant number postconfusional state and posttraumatic amnesia via of patients. The economic costs alone are stagger use of short instruments, behavioral observations, and ing. Additional measures to evaluate concomitant delir Neuroimaging, particularly newer functional imag ium and agitation should be employed. Characteristics employed standardized tests associated with general and rehabilitation outcomes among patients with blast and cerebral and/or dorsolateral prefrontal functioning, other injuries sustained during the global war on terror. Transient vestibu been underevaluated, despite the vulnerability of lar dysfunction after primary blast injury. National Institutes of Health Consensus Conference on as multifactorial and consisting of subdivisions and Rehabilitation of Persons with Traumatic Brain Injury. Rehabilitation of persons with traumatic brain injury employing tests/procedures that measure those func 1998; Available on-line at consensus. Brain injury without head injury: tests, informant and self-rating inventories, naturalistic some physics of automobile collisions with particular ref erence to brain injuries occurring without physical head observations, and thorough interview of patients and trauma. Diffusion tensor any patient, and neuropsychological evaluation(s) must imaging detects clinically important axonal damage after re ect this. The assessment battery in general should mild traumatic brain injury: a pilot study. The human frontal for Disease Control and Prevention: National Center for lobes: functions and disorders. Handbook of clinical neurol up: facts for physicians about mild traumatic ogy: head injury. Prognostic matic brain injury: American congress of rehabilitation role of proton magnetic resonance spectroscopy in medicine. Issues in neuropsychological Cobalt-55 positron emission tomography in traumatic assessment. The Galveston neuropsychological and positron emission tomography orientation and amnesia test: a practical scale to assess assessment. Measurement activation during working memory one month after of posttraumatic amnesia: how reliable is it Neuropsychologic assessment mentation of traumatic brain injury subsequent to mild of frontal lobe dysfunction. The Halstead-Reitan neu sociopathic behavior caused by frontal damage fail to ropsychological test battery: theory and clinical interpre respond autonomically to social stimuli. The California injuries, violence, and aggression: a report of the Vietnam verbal learning test. The Hopkins verbal learning test: development tions in prefrontal glucose metabolism in murderers. Reliability Contributions to neuropsychological assessment: a clin and validity of the apathy evaluation scale. Use of the cognitive test for delirium in patients Wisconsin card sorting test: a positron emission tomogra with traumatic brain injury. Dimensions of disordered dysfunction of the dorsolateral prefrontal cortex in attention in traumatic brain injury: further validation of schizophrenia, I: regional cerebral blood ow evidence. Amsterdam: Elsevier Science; dysfunction following traumatic brain injury: compari 1994. Cognitive bias, action test: a standardized assessment for everyday action functional cortical geometry, and the frontal lobes: lat impairment. Belasco Introduction and History drowsiness, and general distress were associated with masses [1]. The tumors were global (such as affecting multiple areas neurocognitive effects of brain tumors themselves are of the meninges or bihemispheric disease [1]). This variable and require close examination of the neu awareness of neurobehavioral abnormalities associated rocognitive underpinnings of composite test scores. Finally, basic biomedical background on tumors in children surgical resection of tumors begins in this era, with and adults, the questions of tumor site and metastatic bene cial effects on behavior, though the problems spread as well as treatment effects on brain and cog of postsurgical infection were yet to be worked out. Information will also be presented on the have needed a great deterioration to be noticed, as techniques for diagnosing and treating tumors and on patients were described as developing imbecility issues to be considered in doing research in neuro and dementia [1]. Finally, this chapter will discuss how dis ing the behavioral effects earlier in the course of the orders and syndromes that result from brain tumors tumor development, allowed by modern diagnostic and and their treatments differ from more classical or treatment techniques, is a contemporary issue. Brain tumors and cancers that metastasize to the References to the behavioral effects of brain masses brain allow cancerous cells to pervade normal tissue are found in the early common era. Furthermore, brain tumors are not fully Documented descriptions of the behavioral effects visualized on brain scans (see. A model is emerging that grouping generally fall between that of E-A and Af is constructed by radiation injury to epithelial, glial, A. Race does not seem to in uence survival rates in and neuronal cells; their effects on brain tissue; and patients with malignant gliomas, in part because of the resulting in ammatory processes in the brain. Biological Processes of Brain Neoplasms Although only about 20% of all brain and nervous sys tem tumors are diagnosed under the age of 20 years, the Genesis of Brain Tumors brain tumors are the second most common malignancy of childhood and account for 20% of all childhood cancers [2]. The and oncogenes are not just pathological; they also act improved prognosis for cancer and longer life span as fundamental regulators of cell growth and differ of cancer patients is leading to a higher incidence entiation during normal development [5]. There are of brain metastases, which are the most common regulators that cause programmed cell death or apop brain tumors in adults, but not in children [7, 8]. Gliomatosis cerebri is a rare as well as peripheral nerve sheath tumors (neuro neoplasm characterized by individual neoplastic bromas). Although in hand, is associated with meningiomas and schwan theory not malignant, it behaves malignantly and nomas of the cranial nerves and spinal cord, and presently remains a fatal disease. Impairments can present as neurocognitive de cits vary widely [11] and affect higher cognitive dysfunction, such as executive reasoning, visuoconstructive skill, visual and tac dysfunction and memory impairment, as psychi tual memory, logical abstraction, coordination, and atric features, and as sensorimotor impairments, mental exibility. No improvement cers of the lung, especially small cell lung can in cognition was observed as children matured cer, breast cancer, melanoma, renal cancer, and into adults, even though the number, size, and 36 C. Some studies have examined the effects extent and nature of memory impairment in this of ionizing radiation treatments encompassing disease. Individual patterns can be expected to be the brain for non-neoplastic disease, such as related to the location of tumors and spongiform treatment for tinea capitis, a skin disorder, and dysplasia within the brain. A review of ment related to tumor versus spongiform dysplasia 52 studies of radiotherapy for primary brain is not known.
Order azulfidine 500 mg fast delivery
Less his tologic similarity to normal choroid plexus is found in the rarer choroid plexus carcinomas low back pain treatment guidelines azulfidine 500mg fast delivery. Total surgical resection without additional therapy results in long-term disease control for children with choroid plexus papillomas and for some patients with carcinomas (Packer et al. The utility of adjuvant radiotherapy or chemotherapy for incompletely resected lesions, including carcino mas, has not been proved in a prospective clinical trial. Recently, however, Wolff and colleagues (1999) reported a retrospective analysis of 48 patients with choroid plexus carcinoma and total tumor resection, of whom one-half received postsurgical irradiation. They found a 5 year survival of 68% for the irradi ated group compared with 16% for the nonirradiated group. View of occiput of child with occipital dermal sinus and subcutaneous dermoid tumor, which extended through the calvarium and ended in a fourth ventricular dermoid tumor. Dimples such as these the posterior fossa occupy the vermis and encroach are usually covered with hair and are frequently un on the fourth ventricle. Multivariate analysis of prognostic factors in adult patients with medulloblastoma. Medulloblastoma in lar tumors, especially those with pilocytic cerebellar adults: survival and prognostic factors. Adult medul loblastomas, are curable with modern techniques of loblastoma: prognostic factors and patterns of relapse. Proc Annu Meet Am Soc Clin Oncol the neurosurgeon to safely excise fourth ventricular 16:A1419. Pediatric choroid better defined and, for medulloblastoma, is being ex plexus neoplasms. Brain stem gliomas citrovorum factor rescue in the management of brain of children. Survival and neurologic outcome of infants with Dupuis-Girod S, Hartmann O, Berhamou E, et al. Intrinsic brain-stem tumors of review of 47 patients treated between 1952 and 1981. Results of a prospective randomized trial toma in adults: clinical characteristics and treatment. TrkC expression high-dose thiotepa and etoposide with autologous bone predicts good clinical outcome in primitive neuroectoder marrow rescue in children and young adults with recurrent mal brain tumors. Sur logic detection of leptomeningeal disease in pediatric pa vival results in adult patients treated for medulloblastoma. Survival, patterns of medulloblastoma in childhood: treatment results and a pro failure, and prognostic factors. Ra dren with newly diagnosed diffuse intrinsic brainstem tu diotherapy of primary brain stem tumors. Postoper netic resonance imaging and positron emission tomogra ative neoadjuvant chemotherapy before radiotherapy as phy-guided stereotactic biopsy in brainstem mass lesions: compared to immediate radiotherapy followed by mainte diagnostic yield in a series of 30 patients. A Pediatric dren with recurrent brain tumors with ifosfamide (ifos), Oncology Group study. Patterns of failure in tumors of the central ner praisal of a rare embryonal tumor. Treatment zole, and irradiation for brain stem gliomas: a pilot study of children with medulloblastomas with reduced-dose cran of the Brain Tumor Research Center and the Childrens Can iospinal radiation therapy and adjuvant chemotherapy: a cer Group. Postoperative radiotherapy of intracranial ependy loblastoma: a preliminary report. The effectiveness of chiasmal and hypothalamic gliomas of infancy and child of chemotherapy for treatment of high grade astrocytomas hood with chemotherapy. Med Pediatr Oncol fractionated craniospinal radiation therapy for primitive 24:277. The characterization of such his newly recognized neoplasms, and has deleted some entities, tological similarities has been primarily dependent on light variants and patterns that no longer have diagnostic and/or microscopic features in hematoxylin and eosin-stained biological relevance. Other notable changes include the addi sections, immunohistochemical expression of lineage tion of brain invasion as a criterion for atypical meningioma associated proteins and ultrastructural characterization. It will, however, also create potentially larger genetic basis of tumorigenesis in the common and some rarer groups of tumors that do not ft into these more narrowly brain tumor entities, raising the possibility that such an under defned entities. In 2014, a high interobserver discordance [11, 47], with some centers meeting held in Haarlem, the Netherlands, under the auspices diagnosing these lesions frequently and others diagnosing of the International Society of Neuropathology, established them only rarely. As a result, the most controversial issues at a three-day consensus con both the more common astrocytoma and oligodendroglioma ference by a Working Group of 35 neuropathologists, neuro subtypes become more homogeneously defned. A synopsis of tumor grades for dendrogliomas and oligoastrocytomas leads to the question selected entities is given in Table 3. At this point in time, this is not possible: one must still make a diagnosis of diffuse General principles and challenges glioma (rather than some other tumor type) to understand the nosological and clinical signifcance of specifc genetic the use of integrated [28] phenotypic and genotypic changes. Another reason why objectivity that has been missing from some aspects of the phenotype remains essential is that, as mentioned above, 1 3 Acta Neuropathol Table 1 the 2016 World Health Organization Classifcation of Tumors of the Central Nervous System. The present review, however, has used American English spellings there are individual tumors that do not meet the more nar require genotyping may create challenges with respect to rowly defned phenotype and genotype criteria. These have instances, patient age) and what constitutes prognostically been added into the classifcation in those places where favorable 1p/19q codeletion (combined whole-arm losses, such diagnoses are possible. To avoid numerous sequential hyphens, wildtype nation of novel, genetically defned entity has been used without a hyphen and en-dashes have been Addition of newly recognized entities, variants and patterns used in certain designations. This is followed by characteristic Deletion of former entities, variants and terms associated fndings. Finally, for some tumors, there is a commentary that 1 3 Acta Neuropathol Newly recognized entities, variants and patterns phenotype and genotype; from a prognostic point of view, it groups tumors that share similar prognostic markers; and A number of newly recognized entities, variants and pat from the patient management point of view, it guides the use terns have been added. Variants are subtypes of accepted of therapies (conventional or targeted) for biologically and entities that are suffciently well characterized pathologi genetically similar entities. These newly recognized entities, blastomas, as well as the related diffuse gliomas of child variants and patterns are listed in Table 2 and discussed hood (see below). This approach leaves those astrocytomas briefy in their respective sections below. In other the nosological shift to a classifcation based on both phe words, diffuse astrocytoma and oligodendrogliomas are notype and genotype expresses itself in a number of ways in now nosologically more similar than are diffuse astrocy the classifcation of the diffuse gliomas. Most nota toma and pilocytic astrocytoma; the family trees have been bly, while in the past all astrocytic tumors had been grouped redrawn.
Tagara (Valerian). Azulfidine.
- Is Valerian effective?
- What other names is Valerian known by?
- Depression, anxiety, restlessness, convulsions, mild tremors, epilepsy, attention-deficit hyperactivity disorder (ADHD), chronic fatigue syndrome (CFS), muscle and joint pain, headache, stomach upset, menstrual pains, menopausal symptoms including hot flashes and anxiety, and other conditions.
- Dosing considerations for Valerian.
- How does Valerian work?
- Are there any interactions with medications?
- What is Valerian?
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96840
Order cheap azulfidine on line
Several have reported biochemical changes in the brain pain treatment dvt discount azulfidine master card, including alterations in the dopaminergic, noradrenergic, serotonergic, or gabaergic systems; increased monoamine oxidase; and decreased iron levels (Anderson et al. While results from these studies are varied, taken together, they indicate that excess manganese exposure during early postnatal development can lead to alterations in brain chemistry and behavioral development. Formulas were exclusively fed to infants starting on the day of birth and extending through 4 months of age, at which time monkeys were transitioned to standard laboratory diet. The battery included measures of motor, cognitive, and social skills, as well as tests related to the dopamine system (reward delay, fixed interval dopamine drug response). Infants that did not generate sufficient data in each test to permit evaluation were excluded from data analyses. No significant differences between groups were observed for body weights and levels of dopamine and serotonin metabolites in cerebrospinal fluid. Monkeys fed soy supplemented with manganese were consistently more active during 12 weekly 7-minute observation periods, compared with control and soy monkeys. Assessment of gross motor maturation during these observation periods did not detect clear differences between the groups. Both soy and soy plus manganese groups showed some changes in activity/sleep patterns. Compared with controls at 4 months, the 4-month monkeys fed soy plus manganese showed 50% less activity (p<0. At 8 months (but not at 4 months), both soy and soy plus manganese monkeys showed significantly (p<0. Social interactions were assessed during 16 sessions in which each monkey was paired with another monkey in the study. Significant group differences were not consistently observed in more highly structured tests to assess cognitive functions including learning, memory, and attention than controls (p<0. For example, a response latency decrease was observed in a reward delay response task in the soy group by 50% compared to control, but no significant difference (although a 20% reduction) was observed in the soy plus manganese group. The authors noted that more formal tests of cognitive functions would be most appropriately administered at more mature ages. The authors dosed the pups with 150 mg manganese/kg/day by gavage in water for 41 days. In 43-day-old rats, the increases in brain manganese levels were less than those observed in younger rats. Manganese treatment decreased the concentration of homovanillic acid (metabolite of dopamine) in the striatum and the hypothalamus, but not in other brain regions. In a similar study, neonatal rats given bolus doses of manganese chloride in water of 0. In the first study, male rat pups were administered 0, 1, 10, or 20 mg manganese/kg/day (as manganese chloride) via gavage in 5% sucrose solution for 24 days postnatal. Hypothalamic norepinephrine was unaffected by any manganese dose, and no significant changes in neurochemistry were noted in the corpus striatum. The authors suggested that the observed effects were probably due to decreased activity of tyrosine hydroxylase and increased levels of monoamine oxidase. The authors performed neurochemical analyses of hypothalamus and corpus striatum as before and observed that serotonin was increased in the hypothalamus at the highest dose, but was not elevated significantly in the striatum. Acetylcholinesterase levels were significantly decreased in the striatum at the highest dose, but were unchanged in the hypothalamus. The authors believed that the decrease in acetylcholinesterase to be of minor functional significance given that other mechanisms can also regulate acetylcholine metabolism. There was a significant decrease in body weight gain in pups at the highest manganese exposure dose. However, in adult rats, the amplitude of the acoustic startle reflex was significantly decreased compared to the control at the lowest dose tested. The only behavioral end point affected during the neonatal period was a significant (p<0. The results indicate that neonatal exposure of rats to excess manganese caused subtle behavioral effects (altered balance in the neonatal period and diminished locomotor response to cocaine in adulthood) and neurochemical effects in adulthood (decreased dopamine binding sites in the striatum). The two highest dose groups of rats took approximately twice as long (2 seconds) as control and 0. The control group required approximately 40 seconds; the high-dose group required 75 seconds (an 88% increase in the high-dose group over the control). In the passive avoidance task, there was a positive linear trend, with the highest dose group showing a 3-fold increase in the number of footshocks received over the control. A negative linear relationship was also observed in striatal dopamine concentrations, with the high-dose group having approximately half the dopamine concentration of the control. No dose-related trends over time points were observed in manganese content of tissues. Again, Sprague-Dawley rat pups received dietary supplementation in the form of 0, 0. No statistically significant results for any individual treatment group for any behavioral task or striatal dopamine levels. A statistically significant positive trend was observed for passive avoidance (approximately 50% more footshocks in highest dose group, compared with control). Dose groups were balanced across sex within each of 26 litters, each culled to 10 pups with an approximate 2:1 male to female ratio. All treated males had increased stereotypical behavior in the radial arm maze (p<0. Additionally, there were significant decreases in dopamine D1 and D2 receptors and dopamine transporter in multiple brain regions from males from the 50 mg/kg/day group. In a follow-up study, Kern and Smith (2011) evaluated the effects of preweaning manganese exposure on the adult dopaminergic system, behavior, and astrocytic activation. Sprague-Dawley rat pups were exposed to 0, 25, or 50 mg manganese/kg/day using the experimental design described above. At 50 mg/kg/day, additional regions in the adult brain had significantly increased atrocytic activation (prefrontal cortex, nucleus accumbens). In the open field, there were no measureable differences in activity in adults (compared to increased activity in weanlings reported in the previous study). However, a residual effect could be observed under the influence of D-amphetamine. In order to determine if developing animals are more susceptible to the neurochemical and neurobehavioral effects of manganese exposure, Moreno et al. Littermates from timed-pregnant C57Bl/6 mice were paired in control and manganese-exposed groups, receiving 0, 4. Brain levels of manganese, iron, and copper were also measured in three animals per group. In all treated animals, brain regions with the highest levels of manganese were striatum, substantia nigra, and cortex. In the open field, juvenile-only exposed males, but not females, spent significantly (p<0. These results indicate that developing mice are more sensitive to neurobehavioral and neurochemical effects of manganese exposure than adult animals, and that previous juvenile exposure increases susceptibility to these effects from manganese exposure in adults. However, it should be noted that these measures actually decreased with respect to the control in the low dose manganese group. Overall, data do not appear to support an effect of manganese exposure on measured biochemical variables indicative of oxidative stress.
Purchase 500 mg azulfidine amex
Elevated manganese and cognitive performance in school-aged children and their mothers pain treatment center seattle buy discount azulfidine 500 mg on line. Manganese neurotoxicity, a continuum of dysfunction: Results from a community based study. Manganese alters mitochodrial integrity in the hearts of swine marginally deficient in magnesium. Control of tissue manganese: Initial absence and sudden emergence of excretion in the neonatal mouse. Trace element reference values in tissues from inhabitants of the European community. Ingestion of Mn and Pb by rats during and after pregnancy alters iron metabolism and behavior in offspring. Striatal manganese accumulation induces changes in dopamine metabolism in the cirrhotic rat. Biomarkers of manganese exposure in a population living close to a mine and mineral processing plant in Mexico. Exposure of laboratory animals to atmospheric manganese from automotive emissions. Manganese intoxication decreases the expression of manganoproteins in the rat basal ganglia: An immunohistochemical study. Uptake, distribution and behavioral effects of inhalation exposure to manganese (MnO2) in the adult mouse. Transfection of a manganese-containing superoxide dismutase gene into hamster tracheal epithelial cells ameliorates asbestos-mediated cytotoxicity. Nervous system effects of occupational manganese exposure on South African manganese mineworkers. The nervous system effects of occupational exposure on workers in a South African manganese smelter. Behavioral effects of chronic manganese administration in rats: Locomotor activity studies. Manganese intoxication during total parenteral nutrition: report of two cases and review of the literature. Persistent effects of manganese on effortful responding and their relationship to manganese accumulation in the primate globus pallidus. Visualizing manganese in the primate basal ganglia with magnetic resonance imaging. Epidemiological studies on disturbance of respiratory system caused by manganese air pollution: (Report 1) Effects on respiratory system of junior high school students. Bright basal ganglia in T1-weighted magnetic resonance images are frequent in patients with portal vein thrombosis without liver cirrhosis and not suggestive of hepatic encephalopathy. Manganese tissue dosimetry in rats and monkeys: Accounting for dietary and inhaled Mn with physiologically based pharmacokinetic modeling. Manganese distribution in the brain and neurobehavioral changes following inhalation exposure of rats to three chemical forms of manganese. Assessment of bioaccumulation, neuropathology, and neurobehavior following subchronic (90 days) inhalation in Sprague-Dawley rats exposed to manganese phosphate. Department of Health and Human Services, Public Health Service, National Toxicology Program. Manganese intoxication in the rhesus monkey: A clinical, imaging, pathologic, and biochemical study. Determination of methylcyclopentadienyl manganese tricarbonyl in gasoline by capillary gas chromatography with alternating current plasma emission detection. Conditions for detecting the mutagenicity of divalent metals in Salmonella typhimurium. Perinatal manganese exposure: Behavioral, neurochemical, and histopathological effects in the rat. Zinc, copper, and manganese intake and balance for adults consuming self-selected diets. Behavior of Fe, Mn, Cu and Cd in the Duwamish River estuary downstream of a sewage treatment plant. Changes in activity of the manganese superoxide dismutase enzyme in tissues of the rat with changes in dietary manganese. Mineral content of foods and total diets: the selected minerals in foods survey, 1982 to 1984. Manganese acts centrally to stimulate luteinizing hormone secretion: A potential influence on female pubertal development. Trace elements in the human central nervous system studied with neutron activation analysis. Effects of oral administration of manganese on the kidneys and urinary bladder of Sprague-Dawley rats. Histopathological changes in the testis of the Sprague Dawley rat following orally administered manganese. Effect of manganese on luteinizing hormone releasing hormone secretion in adult male rats. In: Chemical attenuation rates, coefficients, and constants in leachate migration. Manganese administration induces the increased production of dopamine sulfate and depletion of dopamine in Sprague-Dawley rats. Mutagenic effects of some water-soluble metal compounds in a somatic eye-color test system in Drosophila melanogaster. Chronic manganese oxide administration to pre-weanling rats: Manganese accumulation and distribution. Chronic ingestion of Mn3O4 by young rats: Tissue accumulation, distribution, and depletion. Chronic ingestion of Mn3O4 by rats: Tissue accumulation and distribution of manganese in two generations. Age-dependent changes in gastrointestinal transport and retention of particulate manganese oxide in the rat. Postnatal manganese exposure attenuates cocaine induced locomotor activity and reduces dopamine transporters in adult male rats. Intellectual function in Mexican children living in a mining area and environmentally exposed to manganese. Morphological changes of rat astrocytes induced by liver damage but not by manganese chloride exposure. Motor alterations associated with exposure to manganese in the environment in Mexico. Epidemiological survey among workers exposed to manganese: Effects on lung, central nervous system, and some biological indices. Relationship between external and internal parameters of exposure to manganese in workers from a manganese oxide and salt producing plant. Influence of the route of administration and the chemical form (MnCl2, MnO2) on the absorption and cerebral distribution of manganese in rats. Preclinical toxic effects of manganese in workers from a manganese salts and oxides producing plant. Assessment of the permissible exposure level to manganese in workers exposed to manganese dioxide dust. Prospective study on the reversibility of neurobehavioral effects in workers exposed to manganese dioxide. Manganese deposition in basal ganglia structures results from both portal-systemic shunting and liver dysfunction. Chronic manganism: Neurologic and laboratory studies during treatment with levodopa. Homeostatic and toxic mechanisms regulating manganese uptake, retention, and elimination. Reference values for the trace elements copper, manganese, selenium, and zinc in the serum/plasma of children, adolescents, and adults.

Cheap azulfidine 500 mg amex
Special Considerations/Preparation Oral solution is available in concentrations of 4 mg/mL and 8 mg/mL (contains 0 pain treatment center suny upstate order azulfidine uk. Initial doses of 2 mg/kg/day orally in 3 divided doses have been used while some authors recommend starting at 0. Contraindications/Precautions Contraindicated in patients with cardiogenic shock, sinus bradycardia greater than first degree block, reactive airway disease, or diminished myocardial contractility. Potential molecular mechanisms of action for propranolol in the treatment of infantile hemangioma include vasoconstriction (reduction of blood flow to the hemangioma), inhibition of angiogenesis (decreased expression of vascular endothelial growth factor and inhibition of tubulogenesis of endothelial cells), and induction of apoptosis in endothelial cells. Adverse Effects Adverse effects are related to beta-receptor blockade: Bradycardia, bronchospasm, and hypoglycemia are most frequently reported. A withdrawal syndrome (nervousness, tachycardia, sweating, hypertension) has been associated with sudden cessation of the drug. Asymptomatic and symptomatic hypoglycemia, requiring hospitalization, have been reported in infants receiving propranolol for the treatment of infantile hemangioma. Monitor vital signs and measure blood glucose during initiation of treatment and after dosage changes. Special Considerations/Preparation 699 Micormedex NeoFax Essentials 2014 Oral solution is available in concentrations of 4 mg/mL and 8 mg/mL (contains 0. Terminal Injection Site Compatibility Alteplase, dobutamine, heparin, hydrocortisone succinate, linezolid, milrinone, morphine, potassium chloride, and propofol. Infusion rate of a 10 mg/mL solution (undiluted) should not exceed 5 mg/min [1] [2]. Cases of life-threatening pulmonary hypertension and severe hemorrhagic pulmonary edema have been reported in infants after protamine administration [4]. Combines ionically with heparin to form a stable complex devoid of anticoagulant activity. Monitoring 701 Micormedex NeoFax Essentials 2014 Monitor vital signs, clotting functions, and blood pressure continuously. Title Protamine Dose Intravenous Time since last heparin dose in minutes and protamine dose: Less than 30 min: 1 mg per 100 units heparin received [1]. Maximum dose: 50 mg 702 Micormedex NeoFax Essentials 2014 Administration Administer intravenously. Black Box Warning Hypotension, cardiovascular collapse, pulmonary edema, pulmonary vasoconstriction, and pulmonary hypertension may occur [2] [3]. Hypotension, bradycardia, dyspnea, and transitory flushing have been reported in adults [2]. Monitoring Monitor vital signs, clotting functions, and blood pressure continuously. Special Considerations/Preparation Available as a 10-mg/mL concentration (preservative-free) in 5 and 25-mL vials. Dose regimen should be adjusted to maintain a target peak protein C activity of 100%. After resolution of acute episode, maintain trough protein C activity level above 25% for duration of treatment. Uses Treatment of patients with severe congenital protein C deficiency for the prevention and treatment of venous thrombosis and purpura fulminans. Also indicated as a 704 Micormedex NeoFax Essentials 2014 replacement therapy [1] [2] [3] [4]. Pharmacology Protein C, a precursor of a vitamin K-dependent anticoagulant glycoprotein, is activated by the thrombin/thrombomodulin-complex on the endothelial cell surface resulting in subsequent potent anticoagulant effects. Adverse Effects Patients receiving protein C and initiating oral anticoagulant therapy are at increased risk for warfarin-induced skin necrosis. Most serious and common adverse events reported were hypersensitivity or allergic reactions and lightheadedness. During acute thrombotic events, measure protein C activity immediately before the next dose until the patient is stabilized; dose regimen should be adjusted to maintain a target peak protein C activity of 100% (1 international unit/mL). Special Considerations/Preparation Available in single-dose vials that contain nominally 500 (blue color bar) or 1000 (green color bar) international units human protein C. For patients beginning warfarin therapy (vitamin K antagonist therapy), continue protein C until stable anticoagulation is achieved. Pharmacology 706 Micormedex NeoFax Essentials 2014 Protein C, a precursor of a vitamin K-dependent anticoagulant glycoprotein, is activated by the thrombin/thrombomodulin-complex on the endothelial cell surface resulting in subsequent potent anticoagulant effects. Limited data also suggests a faster clearance and larger volume of distribution in young children which may lead to significantly reduced Cmax and therefore, reduced systemic exposure compared to older subjects [1] [3]. Patients with renal impairment may experience sodium overload (contains greater than 200 mg of sodium in maximum daily dose) [1]. Closely monitor patients with renal impairment for sodium overload (contains greater than 200 mg of sodium in maximum daily dose) [1] [3]. Vials should be brought to room temperature and reconstituted with 5 mL and 10 mL of sterile water for injection, respectively, to provide a concentration of 100 international units/mL. When reconstituted, contains the following excipients: human albumin 8 mg/mL, trisodium citrate dihydrate 4. Pyridoxine and antiepileptics are then withdrawn, followed by a reoccurrence of clinical seizures that are, again, successfully treated with pyridoxine monotherapy [4] [5] [1] [2] [3]. Pharmacology Pyridoxine is a coenzyme in amino acid and carbohydrate metabolism required for the conversion of tryptophan to both niacin and neurotransmitter serotonin and conversion of dopa to dopamine. A pyridoxine level than less 20 nanomoles/L is indicative of deficiency [7] Special Considerations/Preparation Injectable form available in concentration of 100 mg/mL (1 mL in 2-mL vial). They typically present in the neonatal period or early infancy; however, seizures can occur for the first time at up to 3 years of age. In addition to seizures, presentation may include hypothermia, jitteriness, encephalopathy, abdominal distension, and vomiting. Cardiorespiratory monitoring is recommended and ventilator support may be necessary with initial administration of pyridoxine. Serum half-life of quinupristin in adults ranges from 1 to 3 hours, and of dalfopristin ranges from 5 to 9 hours. Adverse Effects Myalgias and arthralgias occur frequently in adults with hepatic or renal failure. Special Considerations/Preparation Synercid is supplied as a lyophilized powder in single-dose, 10-mL vials containing 500 mg or 600 mg. Concentrations less than 1 712 Micormedex NeoFax Essentials 2014 mg/mL may be used if venous irritation occurs following peripheral administration. Terminal Injection Site Compatibility Aztreonam, fluconazole, metoclopramide, and potassium chloride. Uses Limited to treatment of infections caused by gram positive organisms resistant to other antibiotics, eg, methicillin-resistant Staph. Synercid is a parenteral antimicrobial agent which consists of two streptogramin antibiotics (quinupristin and dalfopristin in a 30:70 ratio) that inhibit bacterial protein synthesis by binding to separate sites on the bacterial ribosome. Reconstitute 500-mg and 600-mg vials by adding 5 mL or 6 mL of Sterile Water for Injection or D5W, respectively, resulting in a concentration of 100 mg/mL. Concentrations less than 1 mg/mL may be used if venous irritation occurs following peripheral administration. Diluted solution is stable for 5 hours at room temperature, or 54 hours if stored under refrigeration. Contraindications/Precautions the use of H2-blockers in preterm infants has been associated with facilitating Candida species colonization [1], and an increased risk for late-onset bacterial and fungal sepsis [2] [1]. Elimination half-life in neonates is 3 to 7 hours, and is prolonged in preterm infants and patients with renal or hepatic insufficiency. Adverse Effects Ranitidine is generally well tolerated by infants, children and adults, and has a low incidence of adverse effects, including rash, headache, fatigue, irritability, dizziness, nausea, constipation, and diarrhea, that are usually mild. Elevations in hepatic enzymes, leukopenia, and bradycardia have been reported in adults [6] [7]. Special Considerations/Preparation 715 Micormedex NeoFax Essentials 2014 Available as a 1 mg/mL preservative-free solution for injection in 50 mL single-dose plastic containers, and a 25 mg/mL injectable solution in 2 and 6-mL vials. Acyclovir, acetazolamide, amikacin, aminophylline, ampicillin, atropine, aztreonam, cefazolin, cefepime, cefoxitin, ceftazidime, chloramphenicol, clindamycin, dexamethasone, digoxin, dobutamine, dopamine, enalaprilat, epinephrine, erythromycin lactobionate, fentanyl, fluconazole, flumazenil, furosemide, gentamicin, glycopyrrolate, heparin, insulin, isoproterenol, lidocaine, linezolid, lorazepam, meropenem, metoclopramide, midazolam, milrinone, morphine, nicardipine, nitroprusside, pancuronium bromide, penicillin G, piperacillin, piperacillin/tazobactam, potassium chloride, propofol, protamine, remifentanil, tobramycin, vancomycin, vecuronium, vitamin K1, and zidovudine. Saiman L, Ludington E, Pfaller M et al: Risk factors for candidemia in Neonatal Intensive Care Unit patients. Pulsifer-Anderson E: National Institues of Health recommends the routine use of H2 blockers in preterm infants be carefully evaluated.