
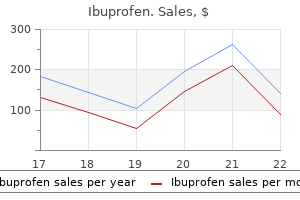
Ibuprofen
Discount ibuprofen online amex
The manufacturing process contains steps for the Risk Summary clearance of viruses pain medication for small dogs buy generic ibuprofen 600 mg online. The estimated background risk of major birth defects and miscarriage Available as 45 mg of ustekinumab in 0. The syringe is ftted with a passive needle Data guard and a needle cover that contains dry natural rubber (a derivative of latex). Each 1 mL preflled syringe delivers 90 mg ustekinumab, L-histidine and L-histidine Animal Data monohydrochloride monohydrate (1 mg), Polysorbate 80 (0. However, if ustekinumab is transferred into human milk the effects of local baseline and up to two weeks post-treatment in subjects with psoriasis. There was no apparent accumulation in serum ustekinumab between older and younger patients, the number of patients aged 65 and over is concentration over time when given subcutaneously every 12 weeks. Steady state ustekinumab No effects on fertility were observed in female mice that were administered an concentration was achieved by the start of the second maintenance dose. In a 26-week toxicology study, one out of 10 monkeys subcutaneously administered Distribution 45 mg/kg ustekinumab twice weekly for 26 weeks had a bacterial infection. Subjects with guttate, erythrodermic, or all psoriasis studies following subcutaneous administration. Metabolism In both studies, the endpoints were the proportion of subjects who achieved the metabolic pathway of ustekinumab has not been characterized. The median trough serum two-thirds of all subjects had received prior phototherapy, 69% had received either concentrations of ustekinumab in subjects of higher weight (greater than 100 kg) prior conventional systemic or biologic therapy for the treatment of psoriasis, in the 90 mg group were comparable to those in subjects of lower weight (100 kg with 56% receiving prior conventional systemic therapy and 43% receiving prior or less) in the 45 mg group. However, the clinical relevance of in vitro data has In subjects who weighed 100 kg or less, response rates were similar with both the not been established [see Drug Interactions (7. The relevance of these experimental 7/166 108/168 103/164 14/290 220/297 216/289 fndings in mouse models for malignancy risk in humans is unknown. Of the adolescent subjects, approximately 63% had prior exposure to phototherapy or conventional systemic therapy and approximately 11% had prior exposure to biologics. Subjects were followed for up to 60 weeks following frst administration of study agent. Patients with each subtype of PsA were Baseline 15 12 13 enrolled, including polyarticular arthritis with the absence of rheumatoid nodules Mean Change at Week 24 -3 -5 -6 (39%), spondylitis with peripheral arthritis (28%), asymmetric peripheral arthritis Number of tender jointsb (21%), distal interphalangeal involvement (12%) and arthritis mutilans (0. Over Baseline 25 22 23 70% and 40% of the patients, respectively, had enthesitis and dactylitis at baseline. The primary endpoint was the percentage of patients achieving Mean Change at Week 24 -0. At baseline and throughout the study, approximately 46% of the point during maintenance therapy. At baseline, in clinical remission, compared to 30% of patients in the placebo group. Clinical 50 94 18% 67 121 26% Response (20%) (38%)b (10%, 25%) (32%) (58%)b (17%, 35%) Disease assessment was based on the Mayo score, which ranged from 0 to 12 (100 point), and has four subscores that were each scored from 0 (normal) to 3 (most severe): Week 8 stool frequency, rectal bleeding, fndings on centrally-reviewed endoscopy, and physician global assessment. Moderately to severely active ulcerative colitis was 70 Point 75 109 13% 81 135 26% defned at baseline (Week 0) as Mayo score of 6 to 12, including a Mayo endoscopy Response, (30%) (44%)a (5%, 22%) (39%) (65%)b (17%, 35%) subscore 2. An endoscopy score of 2 was defned by marked erythema, absent Week 6 vascular pattern, friability, erosions; and a score of 3 was defned by spontaneous 70 Point 67 101 13% 66 106 19% bleeding, ulceration. At baseline, patients had a median Mayo score of 9, with 84% Response, (27%) (41%)a (5%, 22%) (32%) (51%)b (10%, 28%) of patients having moderate disease (Mayo score 6-10) and 15% having severe Week 3 disease (Mayo score 11-12). Clinical remission with a defnition of: Mayo stool frequency subscore of 0 or 1, Mayo rectal bleeding the primary endpoint was the proportion of patients in clinical remission at subscore of 0 (no rectal bleeding), and Mayo endoscopy subscore of 0 or 1 Week 44. The secondary endpoints included the proportion of patients maintaining (Mayo endoscopy subscore of 0 defned as normal or inactive disease and Mayo clinical response at Week 44, the proportion of patients with endoscopic subscore of 1 defned as presence of erythema, decreased vascular pattern and improvement at Week 44, the proportion of patients with corticosteroid-free no friability) is provided in Table 14. Once a syringe has been however, these patients were eligible to receive a 90 mg subcutaneous injection of stored at room temperature, it should not be returned to the refrigerator. Of these patients, 55/101 (54%) achieved clinical response the syringe if not used within 30 days at room temperature storage. The relationship develop any signs or symptoms of infection [see Warnings and Precautions (5. Normalization of endoscopic appearance of the mucosa was defned as a Mayo endoscopic subscore of 0. Keep the product in the original carton to protect from light until the time of use. These may be signs of infections such as chest infections, or skin infections or shingles that could have serious complications. The viruses used in some types of live vaccines can spread to people with a weakened immune system, and can cause serious problems. Tell your doctor about all the medicines you take, including prescription and over-the-counter medicines, vitamins, and herbal supplements. Keep a list of them to show your doctor and pharmacist when you get a new medicine. Record the date when the preflled syringe is frst removed from the refrigerator on the carton in the space provided. Once a syringe has been stored at room temperature, it should not be returned to the refrigerator. Medicines are sometimes prescribed for purposes other than those listed in a Medication Guide. Active ingredient: ustekinumab Inactive ingredients: Single-dose prefilled syringe for subcutaneous use contains L-histidine, L-histidine monohydrochloride monohydrate, Polysorbate 80, and sucrose. Single-dose vial for subcutaneous use contains L-histidine, L-histidine hydrochloride monohydrate, Polysorbate 80 and sucrose. Do not longer than a maximum single period of 30 days or if the give an injection in an area of the skin that is tender, prefilled syringe has been stored above 30C (86F), do not bruised, red or hard. Your prefilled syringe should look clear and colorless to light yellow with few white particles. This will let the empty syringe move up until the entire needle is covered by the needle guard. If your dose is 90 mg, you will receive either one 90 mg prefilled syringe or two 45 mg prefilled syringes. If you receive two 45 mg prefilled syringes for a 90 mg dose, you will need to give yourself a second injection right after the first. If the expiration date an injection in an area of the skin that is tender, bruised, red has passed, call your doctor or pharmacist, or call or hard. Let should look clear and colorless to light yellow with few white your skin dry before injecting. Hold the syringe with Step 4: Prepare the needle the needle pointing up to see if it has any air bubbles inside.
Buy ibuprofen 400mg with amex
At autopsy pain treatment pancreatitis 600 mg ibuprofen amex, no intrinsic cerebral pathologic lesion was found to explain the abnormal eye the eyes usually rove randomly with mild met movements. We have observed transient down abolic coma and come to rest in the forward ward as well as transient upward deviation of the position as coma deepens. Conju stimulation often provides valuable informa gate downward gaze, or occasionally upward tion about the depth of coma in patients with gaze, can occur in metabolic as well as in struc metabolic disease. The ocular response to pas tural disease and by itself is not helpful in the sive head movement is less reliable than the 39 caloric test, as absence of oculocephalic re differential diagnosis. If caloric stim A 63-year-old woman with severe hepatic cir ulation evokes nystagmus, cerebral regulation rhosis and a portacaval shunt was found in coma. The pupillary diameters were 4 mm on ously deviate downward following lateral devia 39 the right and 3 mm on the left, and both reacted to tion, one should suspect drug-induced coma. Her eyes were deviated conjugately down Finally, if caloric stimulation repeatedly pro ward and slightly to the right. Oculocephalic re duces dysconjugate eye movements, structural sponses were conjugate in all directions. Her mus brainstem disease should be suspected (but see cles were accid, but her stretch reexes were brisk Chapter 2). There was no history of previous illness, but her parents stated that she had severe emotional problems. She appeared to be A 60-year-old man was found in the street, stu asleep when left alone, with quiet shallow respi porous, with an odor of wine on his breath. After but appeared to resist passive elevation of her assessing radiographically for cervical spine in eyelids. The urine toxicology screens were positive for barbi liver was palpably enlarged. He responded to turates, and she awoke the next morning and ad noxious stimuli only by groaning. There was no mitted ingesting a mixture of sedative drugs to response to visual threat. However, tonic movement elicited full conjugate ocular move deviation of the eyes in response to cold caloric ments. The corneal reexes were decreased but irrigation signied that normal cerebral control of present bilaterally. He did not move her unresponsiveness was the result of organic, but spontaneously, but grimaced and demonstrated probably toxic or metabolic, and not structural extensor responses to noxious stimuli. Toxicology screening discov muscles were symmetrically rigid and stretch re ered at least one cause, but drug overdosages are exes were hyperactive. The plantar responses often mixed, and not all of the components may be were extensor. Patients with metabolic brain disease generally the following morning he responded appropri present two types of motor abnormalities: (1) ately to noxious stimulation. Hyperventilation had nonspecic disorders of strength, tone, and re decreased, and the extensor posturing had dis exes, as well as focal or generalized seizures, appeared. Diffuse rigidity, increased deep tendon and(2)certaincharacteristicadventitiousmove reexes, and bilateral extensor plantar responses ments that are almost diagnostic of metabolic remained. The general autopsy disclosed severe hepatic cir Diffuse motor abnormalities are frequent in rhosis. Paratonia and snout, suck, or grasp reexes may Comment: In this patient, the signs of liver dis be seen in dementia, as well as in patients in ease suggested the diagnosis of hepatic coma. With increasing brainstem depres rst, however, anisocoria and decerebrate rigidity Multifocal, Diffuse, and Metabolic Brain Diseases Causing Delirium, Stupor, or Coma 195 hinted at a supratentorial mass lesion such as carotid distribution infarction initially. However, hypogly cemia also can cause unconsciousness as well as Focal weakness is surprisingly common with focal signs in conscious patients. Others have re have either focal or generalized seizures that 40,41 ported similar ndings. He received 35 units of protamine zinc insulin each morning in addition to 5 units of regular in Motor Abnormalities Characteristic sulin when he believed he needed it. One week of Metabolic Coma before admission he lost consciousness transiently upon arising, and when he awoke, he had a left Tremor, asterixis, and multifocal myoclonus are hemiparesis, which disappeared within seconds. His entire left side was the tremor of metabolic encephalopathy is numb and paralyzed. His pulse was 80 per min coarse and irregular and has a rate of 8 to 10 ute, respirations 12, and blood pressure 130/80 per second. The general physical examination was rest and, when present, are most evident in the unremarkable. There was supranuclear left ors may spread to the face, tongue, and lower facial paralysis and left accid hemiplegia with extremities, and frequently interfere with pur weakness of the tongue and the trapezius muscles. It is not seen in patients with uni was given 25 g of glucose intravenously and re lateral hemispheric or focal brainstem lesions. Today, Asterixis was originally described as a sudden ngerstick glucose testing would have occurred palmar apping movement of the outstretched 44 much earlier, often before reaching the hospital, hands at the wrists. Incipi abolic tremors it sometimes becomes difcult ent asterixis comprises a slight irregular tremor to distinguish between intense asterixis and of the ngers, beginning after a latent period of myoclonus, and there is some evidence that the 2 to 30 seconds that is difcult to distinguish two types of movements represent the same from the tremor of metabolic encephalopathy. Asterixis is generally seen in awake an irregular oscillation of the ngers, usually in but lethargic patients and generally disappears the anterior-posterior direction but with a ro with the advent of stupor or coma, although tary component at the wrist. The second con occasionally one can evoke the arrhythmic con sists of random movements of the ngers at the traction in such subjects by passively dorsi metacarpal-phalangeal joints. Asterixis can also be elicited tern becomes more and more marked as the pa in stuporous patients by passively exing and 46 tient holds his or her wrist dorsiexed until abducting the hips. Flapping abduction nally the ngers lead the hand into a sudden adduction movements occurring either syn downward jerk followed by a slower return to chronously or asynchronously suggest meta the original dorsiexed position. Electromyograms recorded dur feet is often an easier posture for obtunded ing asterixis show a brief absence of muscular patients to maintain). Ventila nonrhythmic, nonpatterned gross twitching in tory patterns, with the exception of psychogenic volving parts of muscles or groups of muscles hyperventilation, are normal. However, it tion, with nystagmus having a quick phase away may be seen in some waking patients with neu from the side of ice water irrigation; there is rodegenerative disorders. In some patients with psychogenic coma, orders (Creutzfeldt-Jakob disease and related the eyes deviate toward the ground when the 49 disorders). Most conscious bolic brain disease have diffusely abnormal patients with metabolic brain disease are con motor signs including tremor, myoclonus, and, fused and many are disoriented, especially for especially, bilateral asterixis. The patient with cannot concentrate well and cannot easily re gross structural disease, on the other hand, tain new information. Early during the illness, generally has abnormal focal motor signs and the outstretched dorsiexed hands show irreg if asterixis is present, it is unilateral. Co awake patients with psychogenic illness, if they matose patients with metabolic brain disease will cooperate, are not disoriented and can re usually suffer from partial dysfunction affect tain new information. If they seem disoriented, ing many levels of the neuraxis simultaneously, they are disoriented to self. However, although the overall me tabolism of the brain is relatively constant, dif Earlier chapters of this book have described the ferent areas of the brain metabolize at differ 55 physiologic relationships among the brainstem, ent rates, depending on how active an area is. The produce rapidly evolving neurologic abnor brain suffers a special vulnerability in that it malities.
Ibuprofen 400mg with mastercard
Results of a prospective randomized trial toma in adults: clinical characteristics and treatment fibromyalgia treatment guidelines american pain society purchase ibuprofen online now. TrkC expression high-dose thiotepa and etoposide with autologous bone predicts good clinical outcome in primitive neuroectoder marrow rescue in children and young adults with recurrent mal brain tumors. Sur logic detection of leptomeningeal disease in pediatric pa vival results in adult patients treated for medulloblastoma. Survival, patterns of medulloblastoma in childhood: treatment results and a pro failure, and prognostic factors. Ra dren with newly diagnosed diffuse intrinsic brainstem tu diotherapy of primary brain stem tumors. Postoper netic resonance imaging and positron emission tomogra ative neoadjuvant chemotherapy before radiotherapy as phy-guided stereotactic biopsy in brainstem mass lesions: compared to immediate radiotherapy followed by mainte diagnostic yield in a series of 30 patients. A Pediatric dren with recurrent brain tumors with ifosfamide (ifos), Oncology Group study. Patterns of failure in tumors of the central ner praisal of a rare embryonal tumor. Treatment zole, and irradiation for brain stem gliomas: a pilot study of children with medulloblastomas with reduced-dose cran of the Brain Tumor Research Center and the Childrens Can iospinal radiation therapy and adjuvant chemotherapy: a cer Group. Postoperative radiotherapy of intracranial ependy loblastoma: a preliminary report. The effectiveness of chiasmal and hypothalamic gliomas of infancy and child of chemotherapy for treatment of high grade astrocytomas hood with chemotherapy. Med Pediatr Oncol fractionated craniospinal radiation therapy for primitive 24:277. Jorgensen 1, Yi Chieh Lim 3, Louise Goksoyr 1, Swati Choudhary 1, Tobias Gustavsson 1, Robert Dagil 1, Mads Daugaard 4, Adam F. Theander 1, Olga Ostrup 5, Ulrik Lassen 7, Petra Hamerlik 3, Ali Salanti 1,* and Mette O. Introduction Diuse gliomas are the most common primary malignant brain tumors [1]. As the name implies, a general trait of these tumors is their diuse invasion into the brain parenchyma, which impedes complete surgical resection and most likely explains the poor prognosis and frequent local recurrence [2]. A precise classication of diuse gliomas is needed for the optimal diagnosis, stratication, and treatment of patients [3,4]. Most likely, these migrating cells would also be the ones accessing the blood stream. Tumors of the central nervous system were until recently not considered to be metastatic. Taken together, these studies provide evidence that invasive glioma cells successfully intravasate to the blood circulation and may therefore potentially become an important and easily available source of information on the mutational and phenotypic state of the primary tumor. The use of antibodies towards one or few protein surface markers will render the detection fragile to changes in the expression level of the selected marker. On the other hand, targeting several proteins by using an antibody cocktail increases the risk of false positives and high background levels due to healthy cells expressing one or more of the included markers. Both constructs included a C-terminal 6x His-tag and V5-tag, as well as an N-terminal SpyTag. After a 1-h incubation at room temperature, the biotinylated SpyCatcher was puried using a zeba spin column with a 7 kDa cut o. Transition was conrmed by changes in the expression of mesenchymal protein markers using western blot as well as changes in morphology. The resulting peptides were captured and washed using a C18 resin stage-tipping [30]. D1306, Life Technologies) and mounted using Faramount Aquous Mounting Media (Dako). The slides were imaged using the 10 objective of Cytation 3 Cell Imaging Multi-Mode Reader (BioTek, Europe). Following staining, the cells were resuspended in complete growth media and incubated for 30 min. Cell concentration was measured by manually counting the number of viable cells in a 1:1 mixture with Trypan Blue solution (Sigma-Aldrich). The average of the cell counts was used when calculating the percentage of recovery. The cell suspension was transferred to a 96-well plate and counted under a light microscope (10 objective) to ensure precise cell count before spike-in. After adding the cancer cells to the blood, the samples were immediately processed, as described in Section 2. Patient Samples Up to 9 mL blood samples from glioma patients were collected under ethical approval (journal no. A neodymium cylinder magnet was used to drag cells bound to beads towards the side of the tube, enabling removal of supernatant. Variants outside a selected glioblastoma-related target region containing 95 candidate genes were excluded from the call set. The most relevant mutations (described in somatic mutation databases or being frameshift/stop-gain) were further manually inspected by looking at aligned reads sequences. Cell cultures poorly represent the phenotypic plasticity of cancer cells in vivo, where the tumor cells continuously respond to signals from the microenvironment. It should be noted that, although glial cells originate from ectodermal tissue, these cells binding. It should be noted that, although glial cells originate from ectodermal tissue, these cells exhibit a more mesenchymal appearance, such as the expression of vimentin [28]. Thus, the transition exhibit a more mesenchymal appearance, such as the expression of vimentin [28]. Thus, the transition is measured as an increased expression of mesenchymal markers, rather than a down-regulation of is measured as an increased expression of mesenchymal markers, rather than a down-regulation of epithelial markers [36]. This was accompanied by a clear change in morphology as cells more mesenchymal state (Figure 1B). This was accompanied by a clear change in morphology as cells tended to become more elongated, which confirms the occurrence of a transition [36,37] (Figure 1C). This was further tested by flow cytometry analysis showing specific binding to2A). This strategy allowed allowed us to directly assess the recovery of spiked cells independent of downstream staining andus to directly assess the recovery of spiked cells independent of downstream staining and detection detection biases.

| Comparative prices of Ibuprofen | ||
| # | Retailer | Average price |
| 1 | A&P | 915 |
| 2 | Wegman's Food Markets | 576 |
| 3 | Big Lots | 597 |
| 4 | Defense Commissary Agy. | 396 |
| 5 | CVS Caremark | 486 |
| 6 | Williams-Sonoma | 125 |
Cheap ibuprofen 600 mg with mastercard
Viral shedding from nasopharyngeal secretions is most abundant during the frst 2 to 3 days of infection and usually ceases by 7 to 10 days pain medication for dogs arthritis buy discount ibuprofen 600mg on line. Serologic diagnosis of rhinovirus infection is impractical because of the large number of antigenic types. Use of such medications also is discouraged for children younger than 6 years of age because of lack of effcacy and concerns regarding safety. Antimicrobial agents are not indicated for people with a common cold caused by a rhinovirus or other virus, because antimicrobial agents do not prevent secondary bacterial infection and their use may promote the emergence of resistant bacteria and complicate treatment for a bacterial infection (see Antimicrobial Stewardship: Appropriate and Judicious Use of Antimicrobial Agents, p 802). Rickettsial Diseases Rickettsial diseases comprise infections caused by bacteria of the genera Rickettsia (endemic and epidemic typhus and spotted fever group rickettsioses), Orientia species (scrub typhus), Ehrlichia species (ehrlichiosis), and Anaplasma species (anaplasmosis). Risk factors for severe disease include glucose-6-phosphate dehydrogenase defciency, male sex, and use of sulfonamides. Immunity against reinfection by the same agent after natural infection usually is of long duration, except in the case of scrub typhus. Among the 4 groups of rickettsial diseases, some cross-immunity usually is conferred by infections within groups but not between groups. Reinfection of humans with Ehrlichia species and Anaplasma species has not been described. Rickettsiae are small, coccobacillary gram-negative bacteria that are obligate intracellular pathogens and cannot be grown in cell-free media. They grow in different cellular compartments: Orientia and Rickettsia organisms in the cytoplasm and Ehrlichia and Anaplasma organisms in different nonacidi fed modifed phagosomes. Humans are incidental hosts, except for epidemic (louseborne) typhus, for which humans are the principal reservoir and the human body louse is the vector. Rickettsia life cycles typically involve arthropod and mammalian reservoirs, and transmission occurs as a result of environmental or occupational exposure. Geographic and seasonal occurrence of rickettsial disease is related to arthropod vector life cycles, activity, and distribution. The indirect immunofuorescent antibody assay is recommended in most circum stances because of its relative sensitivity and specifcity; however, it cannot determine the causative agent to the species level. The Weil-Felix test will not detect infections caused by Ehrlichia species and Anaplasma species. Although older tetracycline-class antimicrobial agents generally are not given to children younger than 8 years of age because of the risk of dental staining, doxycycline has not been demonstrated clearly to have the same effect on developing dentition (see Tetracyclines, p 801). Antimicrobial treatment is most effective when children are treated during the frst week of illness. If the disease remains untreated during the second week, therapy is less effective in preventing complications. Because confrmatory laboratory tests primarily are retrospective, treatment decisions should be made on the basis of clinical fndings and epidemiologic data and should not be delayed until test results are known. Several rickettsial diseases, including Rocky Mountain spotted fever and ehrlichio sis, are nationally notifable diseases and should be reported to state and local health departments. The causative agents of some of these infections share the same group antigen as Rickettsia rickettsii. Each of these infections has some clinical and pathologic features similar to those of Rocky Mountain spotted fever. These diseases are of importance among people traveling to or returning from areas where these agents are endemic and among people living in these areas. The rash develops 1 to 4 days after onset of fever and 3 to 10 days after appearance of an eschar at the site of the bite of a house mouse mite. Without specifc antimicrobial therapy, systemic disease lasts approximately 7 to 10 days; manifestations include fever, headache, malaise, and myalgia. Less frequent manifesta tions include anorexia, vomiting, conjunctivitis, nuchal rigidity, and photophobia. The disease is mild compared with Rocky Mountain spotted fever, and no rickettsialpox associated deaths have been described; however, disease occasionally is severe enough to warrant hospitalization. The disease can occur wherever the hosts, pathogens, and humans coexist but most often erupts in large urban settings. In the United States, rickettsialpox has been described predominantly in northeastern metropolitan centers, especially in New York City. It also has been con frmed in many other countries, including Croatia, Ukraine, Turkey, Russia, South Korea, and Mexico. The disease is not communicable but occurs occasionally among families or people cohabiting a house mouse mite-infested dwelling. Direct fuorescent antibody or immunohis tochemical testing of formalin-fxed, paraffn-embedded eschars or papulovesicle biopsy specimens can detect rickettsiae in the samples and are useful diagnostic techniques. Doxycycline will shorten the course of disease; symptoms resolve typically within 12 to 48 hours after initiation of therapy. Fluoroquinolones and chloramphenicol are alternative drugs, although fuoroquinolones are not approved for this use in children younger than 18 years of age (see Fluoroquinolones, p 800). Rodent-control measures are important in limiting or eliminating spread of rickettsialpox; however, they should be conducted only in conjunction with acaricide application to ensure vector control. Fever, myalgia, severe headache, nausea, vomiting, and anorexia are typical presenting symptoms. The rash usually begins within the frst 6 days of symptoms as erythematous macules or maculopapules. Rash usually appears frst on the wrists and ankles, often spreading within hours proximally to the trunk and involves the palms and soles. Although early development of a rash is a useful diagnostic sign, rash can be atypical or absent in up to 20% of cases. A petechial rash typically is a late fnding and indi cates progression to severe disease. If not treated, illness can last as long as 3 weeks and can be severe, with prominent central nervous system, cardiac, pulmonary, gastrointestinal tract, and renal involvement; disseminated intravascular coagulation; and shock leading to death. Delay in appropriate antimicrobial treatment is associated with severe disease and poor outcomes. Patients treated early in the course of symptoms may have a mild ill ness, with fever resolving in the frst 48 hours of treatment. The primary targets of infection in mammalian hosts are endothelial cells lining the small blood vessels of all major tissues and organs. Other wild animals and dogs have been found with antibodies to Rickettsia rickettsii, but their role as natural reservoirs is not clear. In ticks, the organism is transmitted transstadially from one life stage to the next and transovarially to the eggs and resulting new generation. People with occupational or recreational exposure to the tick vector (eg, pet owners, animal handlers, and people who spend more time outdoors) are at increased risk of acquiring the organism. Laboratory-acquired infection occasionally has resulted from accidental inoculation and aerosol contamination. Mortality is highest in males, people older than 50 years of age, children 5 to 9 years of age, and people with no recognized tick bite or attachment. Delay in disease recognition and initiation of antirickett sial therapy after the ffth day of symptoms increase the risk of death. Factors contribut ing to delayed diagnosis include absence of rash, initial presentation before the fourth day of illness, and onset of illness during months of low incidence. Most cases are reported in the south Atlantic, southeastern, and south central states, although most states in the contiguous United States record cases each year. The principal recognized vectors of R rickettsii are Dermacentor variabilis (the American dog tick) in the eastern and central United States and Dermacentor andersoni (the Rocky Mountain wood tick) in the western United States. Another common tick throughout the world that feeds on dogs, Rhipicephalus sanguineus (the brown dog tick) has been confrmed as a vector of R rickettsii in Arizona and Mexico and may play a role in other regions. The acute sample should be taken early in the course of illness, preferably in the frst week of symptoms, and the convalescent sample should be taken 2 to 3 weeks later. Both IgG and IgM antibodies begin to increase around day 7 to 10 after onset of symp toms; therefore, an elevated acute titer may represent past exposure rather than acute infection. Currently, commercially available enzyme immunoassays are not quantitative, cannot be used to evaluate changes in IgG titer, and should not be used for monitoring titer changes. Sensitivity of skin biopsy testing decreases greatly after the frst 24 hours of appropriate treatment. Treatment is most effective if started in the frst few days of symptoms, and treatment started after the ffth day of symptoms is less likely to prevent death or other adverse outcomes.
Buy generic ibuprofen online
Some manifest preferentially Occasionally pain treatment devices purchase ibuprofen with a visa, they occur in the setting of in children (desmoplastic infantile astro inherited cancer syndromes, including cytoma/ganglioglioma, dysembryoplas Turcot syndrome (in association with tic neuroepithelial tumour), others pref familial polyposis colon cancer) and erentially in adolescents and adults (gan naevoid basal cell carcinoma syndrome Fig 5. Meningiomas these slowly growing, usually benign, neo 36 yr 47 yr 29 yr plasms develop from arachnoidal cells in Low-grade Low-grade Anaplastic the meninges. They preferentially affect astrocytoma, astrocytoma astrocytoma women, particularly those located in the 37 yr glioblastoma mut/ in tumour mut/ in tumour spine. Preferential sites are the cerebral hemi mut/wt in blood 8 months wt/wt in blood spheres. Malignant menin wt = wildtype p53 Choroid plexus = deletion of p53 carcinoma giomas are much less frequent; they may mut/ in tumour infiltrate the brain and often recur locally. Although not very frequent, brain tumours In tumours, the second allele is usually deleted. They manifest as an abdom Tumours of peripheral nerves radiation and chemotherapy, the progno inal mass almost exclusively in children Most of these tumours develop from sis for patients with glioblastomas is very less than 10 years old, with a peak inci myelin-producing Schwann cells and are poor. Many genetic alterations medulla have a better prognosis, and nostic of the inherited neurofibromatosis involved in the development of nervous some lesions regress spontaneously. Magnetic resonance Spinal cord diseases often have devastating consequences, ranging from quadriplegia imaging and paraplegia to severe sensory deficits due to its confinement in a very small area. Introduction to home in on the diagnosis and classify the etiol the term myelopathy describes pathologic ogy appropriately (2-3). This paper reviews have devastating consequences such as quadriple the different etiologies, divided into compressive gia, paraplegia and severe sensory defcits. The history, an adequate neurological ex 1Neuroradiologist, Fundacion Valle de amination and the study of the cerebrospinal fuid Defnition and clinical picture Lili, Cali, Colombia. Patients with myelopathies but no evident to multiple sclerosis, combined subacute degeneration (vitamin lesions, or who present with multiple lesions of chronic appear B12 defciency), tabes dorsalis, and familial spastic paraplegia. If there is evidence of spinal cord Compressive diseases of the spinal cord are divided into compression due to an acute lesion (epidural metastasis or acute and chronic, including degenerative changes, trauma, abscess), defnitive management is required in order to avoid tumor infltration, vascular malformations, infections with damage or to adequately manage all other potential diagnoses. Patients with If the symptoms progress for more than three weeks, transverse clinical fndings of compressive myelopathy that show exten myelitis is improbable, and other conditions must be considered, sive (more than three vertebral segments) fusiform spinal cord such as a spinal tumor, chronic compressive disease, dural hyperintensity in T2 weighted sequences, are often mistakenly arterio-venous fstula, metabolic disorder, sarcoidosis, or a thought to have optic neuritis, or classifed as idiopathic. Increased intensity and thickening of the spinal cord from the bulbo-medullary compressive myelopathy secondary to rheumatoid arthritis. Motor vehicle acci enhancement limited to the point of greatest stenosis, plus a 4 Diagnostic approach to myelopathies. B) Sagittal section with T2 information in C7 showing diminished height and signal intensity with annulus protrusion in C5-C6 and C6-C7; there is also central and left subarticular protrusion of the annulus associated with annulus and ligament tear in C7, giving rise to central spinal hyperintensity due to compressive myelopathy resulting from nucleus pulposus herniation. Some studies have shown that hemorrhage and longer hemato mas are associated with a lower rate of motor recovery (20). They affect mainly men, with no specifc age range (22), and the incidence has been shown to have increased in recent years. T2 weighted image with annulus protrusion in C4 and C5, giving rise to spinal diabetes mellitus, use of intravenous drugs, chronic renal failure, cord hyperintensity due to traumatic compressive myelopathy. Lumbar trauma has also Tumoral compressive myelopathy been described in one third of patients, as a cause for epidural Myelopathy may be the initial manifestation of a malignancy abscess. Human immunodefciency virus has not been shown in up to 20% of cases where the only systemic symptom is to be the cause of the increased incidence (23). Extradural tumors may absent in subacute and chronic stages), increased local tender be classifed as follows: ness, progressive radiculopathy or myelopathy. Mycobacterium tuberculosis is the second most frequent myelopathy associated with subacute dorsal pain that wors pathogen, found in 25% of cases (22). It must be selected as the frst imaging technique because it is more sensitive than other imag Myelopathy of vascular origin ing modalities and allows to rule out other causes. It is provided mainly by the anterior spinal artery that ment, followed by a late phase with well-defned peripheral emerges from the vertebral arteries, the artery of Adamkiewicz enhancement and perilesional edema. The spinal cord may be affected by compressive and fcity of spinal cord diseases (acute ischemia, tumors or multiple non-compressive vascular diseases, of which the most com sclerosis lesion). However, it is not performed frequently be mon are malformations of the dural arteriovenous fstula type cause of limitations such as movement artifacts and the small (29). In cases of vascular malformation, patients present with size of the spinal canal. These enhance with contrast, together with the thickened spinal cord due to myelopathy resulting from an epidural abscess. The age of onset is low thoracic or lumbar regions, and in a lesser proportion, in the under 40 years, when hemorrhage is the main symptom, and sacral and cervical regions. Another cause of myelopathy of vascular origin of the non Eighty per cent present with bladder dysfunction, when the mal compressive type is acute vascular occlusion, which is less formation involves the cone (32). The disease may progress over frequent and may lead to an infarct that mimics myelitis (8). Syringomyelia is a rare neurologic disorder, characterized by the slow development of fuid-flled areas extending along the the diagnosis of myelopathy secondary to spinal cord ischemia spinal cord, and causing symptoms such as pain, weakness and is diffcult because of the lack of diagnostic criteria in the acute stiffness of the back, shoulders and limbs. The sagittal sequence with T2 information shows a high-intensity signal anterior to the spinal cord suggesting a diagnosis of myelopathy due to ischemia. The diagnosis of an infammatory myelopathy requires Transverse myelitis evidence of spinal cord infammation. Other criteria are sequelae, one third have a mild degree of disability, and yet proposed later for the differentiation between infammatory and another third have a serious disability. Middle-aged adults are non-infammatory transverse myelitis, and between idiopathic most frequently affected. It varies transverse myelitis, including the following: 1) spinal bilateral signifcantly in frequency (from 9% to 60% according to some motor, sensory or autonomic dysfunction; 2) bilateral sensory studies) (9). The diagnosis is made by exclusion and it has a course of a few hours and 21 days, from onset to maximum defcit; and progression between four hours and four weeks. It appears as a high-signal image in T2 sequences, with enhancement mainly on the spinal surface that disappears, suggesting its reversible nature. Fusiform spinal edema is found, with areas of intermediate or high signal intensity in T1 sequences. A high-signal center in T2 may be present due to the lower degree of caseifcation or liquefaction. It has been associated with infection or vaccina tion, but this is not considered a criterion in clinical consensus Figure 12. The sagittal sequence with T2 information showed discal and osteophytic changes prognosis; however, recurrent forms make differentiation from of the vertebral bodies associated with bulging of the inferior annulus and thickening and hypersensitivity of the cervical spinal cord from the craniocervical junction down to C7. It is usually due to a rapidly progressing encephalopathy associated with seizures blood-borne infection originating in the lungs, the skin, the or multiple neurologic defcits. It presents with 11% to 28% of patients, generally in the thoracic and cervical severe motor and sphincter dysfunction associated with fever, segments. The image shows alteration in the shape and signal intensity of the vertebral bodies of T10 and T11, of the disc and of the prevertebral soft tissues.
Cheap 400 mg ibuprofen with mastercard
Selection of new equipment must include considerations related to effective cleaning and disinfection (See 1 pain medication for dogs after shots effective ibuprofen 400 mg. A system should be in place to clearly identify equipment which has been cleaned and disinfected. The health care setting should have written policies and procedures for the appropriate cleaning and disinfection of equipment that clearly define the frequency and level of cleaning and assign responsibility for cleaning. Education All aspects of environmental cleaning must be supervised and performed by knowledgeable, trained staff. Regular education and support must be provided by health care organizations and contract agencies to help staff consistently implement safe and effective cleaning, infection prevention and 15-17,158,159,253,254,291-293 control, and occupational health and safety practices. Education on the topics of infection prevention and control and of occupational health and safety should be provided at the initiation of employment as part of the orientation process and as ongoing continuing 8,79,219,220,229,242,294,295 education. Ergonomic considerations and safe management of chemical agents should be emphasized. Shall include: [Legislation] [modified 2018] the correct and consistent use of Routine Practices. Occupational Health and Safety Issues Related to Environmental Services Environmental service workers are exposed to occupational risks including exposure to infectious microorganisms from clients/patients/residents and the health care environment, exposure to the chemical agents used for cleaning, and ergonomic stressors related to the mechanics of cleaning that 147,222,297-303 may involve repeated pushing, pulling, lifting or twisting. Health care facilities shall ensure that these risks are minimized to protect their environmental service workers and allow them to 229 perform their work in an optimal and safe environment. To minimize the risk of infection in both environmental service workers and clients/patients/residents, environmental service workers shall be: 79,219,220,229,304 Provided with infection prevention and control education and training. In addition, environmental service workers should be aware of: Work restrictions including the need to avoid working in client/patient/resident areas when ill 31,243,305 with a known or suspected communicable infection. Non-infectious occupational risks shall also be minimized and environmental service workers shall have access to and training in the use of the personal protective equipment required when preparing, 8,219,220 handling or using chemical cleaning agents. Strategies should also be in place to reduce the risk of 219,220,229,296,304 injury due to ergonomic or other workplace hazards. Contracts with supplying agencies should include the above immunizations for contracted staff. Examples of these policies and procedures include: 31,218,219 A sharps injury prevention program. Staff members carrying on activities in a health care setting who develop a communicable disease may be 243 subject to work restrictions. Exposures occur most commonly via inhalation 145 (respiratory) or direct skin contact. Over time, 151,317,321 without adequate controls, a sensitizer may cause asthma or chronic bronchitis. Respiratory symptoms increase in direct proportion to increased exposure time and higher concentrations of certain 317 chemicals, such as bleach and ammonia. Certain tasks, such as cleaning of toilet bowls, mirrors, sinks, and counter, as well as floor finishing tasks, regularly expose individuals to high concentrations of 145 volatile organic compounds. Irritants in health care settings associated with skin symptoms (irritant contact dermatitis) include water, soaps and detergents, most frequently in those who have underlying atopic dermatitis (allergy, eczema). A smaller number of people will develop allergic contact dermatitis where a particular allergen can cause an inflammatory response, usually hours to days later, which clinically may appear similar to irritant contact dermatitis. It is important that any health care provider who has a significant allergic, asthmatic, or dermatitis history, or who develops symptoms that may be related to work exposures, be assessed by occupational 322 health and safety. Exposure to workplace chemicals may be reduced through the use of engineering controls. Caution should be taken when cleaning and disinfection is performed in small and/or poorly ventilated spaces to reduce the risk of irritation to exposed skin and respiratory tract, and to ensure that exposure limits are not exceeded. Facilities should periodically conduct an occupational hazards assessment with respect to cleaning and disinfection of surfaces and equipment. The assessment should evaluate risks, and ensure that the safest cleaning agents, equipment and processes are selected; that appropriate training and access to personal protective equipment are in place; and that staff are aware of protocols to be 318 followed in the event of accidents, exposures or injuries. The use of automated dispensing systems or ready-to-use products is preferred over manual dilution and mixing, as automated systems reduce direct personal contact with concentrated products and reduce inhalation of volatile organic compounds from concentrated products. Automated systems also ensure that correct dilution ratios are obtained and eliminate the need for decanting. Applications of cleaning chemicals by aerosol or trigger sprays may cause eye injuries or induce or 141,144,222,317,323-331 compound respiratory problems or illness and must not be used. Repetitive movements, awkward work postures, heavy lifting, and application of high forces. Products that are lighter in weight, easily emptied and having proper handle length help reduce the risk of injury. Additionally, a variety of handle lengths should be available to ensure that differently sized cleaning staff have access 222 to appropriate ergonomically designed equipment. For more information about ergonomic design related to environmental cleaning, visit the Public Services Health & Safety Association website. There shall be policies and procedures in place that include a sharps injury prevention program, post-exposure prophylaxis and follow-up, and a respiratory protection program for staff who may be required to enter an airborne infection isolation room accommodating a patient with tuberculosis. There must be appropriate attendance management policies in place that establish a clear expectation that staff members do not come into work when acutely ill with a probable infection or symptoms of an infection. Environmental Cleaning for Specialized Areas In this section, guidance is provided regarding cleaning and upkeep of specific facility areas including the cleaning of clean and soiled utility rooms, the upkeep of environmental cleaning equipment and supply rooms. Each client/patient/resident care area should be equipped with a room dedicated as a soiled utility room that may be used to clean soiled patient/resident 340 equipment that is not sent for central reprocessing. A separate room 80 shall be dedicated to the storage of clean supplies and equipment. A soiled utility room is used for temporary storage of supplies and equipment that will be removed for 80 341 cleaning, reprocessing or destruction, for the disposal of small amounts of liquid human waste, and 81 for rinsing and gross cleaning of medical instruments. Soiled utility rooms should: 80,81 Be physically separate from other areas, including clean supply/storage areas. If a soiled utility room is used only for temporary holding of soiled materials, the work counter and 81 clinical sink is not required; however, facilities for cleaning bedpans must be provided elsewhere. A clean utility/supply room for storing sterile supplies and equipment should: 80,81 Be separate from and have no direct connection with soiled workrooms or soiled holding areas. Toilet cleaning and disinfecting equipment should be discarded when the patient/resident leaves or sooner if required. In multi-bed rooms, a system should be developed for replacement of toilet brushes on a regular basis or as required. When choosing a tool for cleaning toilets, consideration should be given to equipment that will minimize splashing. To facilitate this, facilities shall have a sufficient number of rooms that are dedicated to the storage of cleaning equipment and supplies required for daily cleaning 80,340,341 (housekeeping closets) and are located conveniently throughout the facility. These rooms are 80,341 used for the storage, preparation and disposal of cleaning supplies and equipment, and are distinct from the clean utility/supply rooms described in 6. Facilities may also have centralized housekeeping rooms for storing bulky cleaning equipment and large 80,341 volume of supplies for distribution to local areas. At a minimum, there shall be at least one 80,340 housekeeping closet in all major care areas. In addition, housekeeping closets: Must be dedicated for use as a cleaning supply room where cleaning solution is prepared, and 80,341 dirty cleaning solution is disposed; and must not be used for other purposes. Infection prevention and control must assess construction and maintenance projects during planning, work, and after completion to verify that 31,86 infection prevention and control recommendations are followed throughout the process. Infection prevention and 31 control and occupational health and safety have the authority to halt projects if there is a safety risk. Cleaning is of particular importance both during construction and after completion of the construction project. This should be done as frequently as is necessary to avoid accumulation of dust and dispersion of dust to other areas of the facility, and at least daily. It is important that there is good liaison between the contractor, environmental services, infection prevention and control, and occupational health and safety. The level of cleaning that is expected during construction and at commissioning must be stated in the contract and the responsibility for cleaning 86 both the job site and adjacent areas shall be clearly defined. Where there is transport of construction materials (both clean and used materials) through the health care setting, a clear plan for traffic flow 86 that bypasses care areas as much as possible shall be established and adhered to .
Buy cheap ibuprofen 600mg on line
There is a great deal of accepted pain diagnosis and treatment center tulsa ok cheap 600 mg ibuprofen visa, non-controversial medical science on mycotoxin exposure via the digestive tract including concrete proof of cancer, immune suppres sion; neurological impairment; and harm to intestinal lining & gut microflora and other serious ailments. Toxin producing molds are always present in water damaged homes and are always producing toxins. As a re sult, mold exposure in the indoor environment is pre dominantly through the digestive tract and not respira tory system. Indoor mold even at moderately high concentrations does not typically result in illness or even irrita tion to those not mold sensitive, which is the majority of people. However, breathing even very low concentrations of indoor mold can affect the sensitive (atopic), especially the young, the aged, those suffering from allergies or asthma and those with other illnesses or sensitivities that challenge or compromise their immune systems. Illness promoting indoor mold problems are typically subtle and not visible; otherwise they are quick ly fixed. So, the affected individual sees what appears to be a clean environment with perhaps a whiff of mustiness (odor from growing mold) but feels for some reason worse in the indoor environ ment than out. Mold hidden inside of walls even if extensive, if there is no active water source so the mold is no longer active, does not generally result in illness or irritation because mold exposure (see Mold Ba sics) is limited. Exposure to indoor mold toxins requires that the toxin containing mold spores be air borne so they can be inhaled. Generally speaking, mold trapped inside of walls results in limited ex posure to occupants. Example of white toxic mold hiding in the fiber Invisible unless the air handler is first removed. Fixing (remediating) the problem/ damaged house or office is generally straightforward when the problem is properly diagnosed. Oftentimes repair of the individual is not so simple and will require treatment under Doctor supervision. Bacteria and endotoxins and other factors besides mold may also be involved in causing indoor irrita tion and illness as a result of indoor dampness/ water damage. For an excellent review of the many illness-promoting factors involved in damp or water damaged buildings see: Biocontaminants and Complexity of Damp Indoor Spaces. Main Mycotoxin Exposure Pathways Eating: People are constantly being ex posed to significant levels of mold tox ins via their diet when they eat grains, meat, farmed fish, poultry and many fruits. Generally the level of mycotoxin exposure through the food chain, at least in the U. Breathing: the human respiratory tract can be considered to consist of two regions: (1) Upper airway. The (toxin laden) mold spores that land in the upper airway adhere to the airway mucous lining. Once embedded in the mucous, the spores are rapidly cleared from the airway and are deposited in the digestive tract for later excretion. Mycotoxins absorbed from the digestive tract will enter the blood stream and directly affect the body. But often more important is the indirect affect on the body by damage occurring to gut bacteria/ mi croflora because mycotoxins are strongly bacteriocidal. Therefore gut related problems from mold toxin exposure can be particularly common. The principal route of exposure from breathing mold toxins is via the gut and not the lungs. Subsequently, a common result of elevated mycotoxin exposure is damage to gut microflora. Conclusions Section 1 Most inhaled mold spores are quickly cleared from the upper airway before reaching the lungs. But as we shall see in the next section, continued exposure to elevated levels of mycotoxins can affect a whole lot more than just gut bacteria. There is a great deal of accepted, non-controversial medi cal science on mycotoxin exposure via the digestive tract including concrete proof of cancer, immune suppression; neurological impairment; and harm to intestinal lining and gut microflora and other serious ailments. While there is limited research on mold toxins that enter the lungs, there are literally thousands of scientific articles on illnesses resulting from mold toxins that enter the body through the digestive system (are eaten. One of the best reviews is Mycotoxins: Risks in Plant, Animal, and Human Systems by the U. This is one of the six mold toxins regulated in foods produced in and imported into the E. Trichothecenes inhibit protein synthesis and have many acute effects, including anemia and infant pulmonary hemorrhage. Carcinogenic Mycotoxins Several common molds produce very strong cancer causing agents. Aspergillis flavus, which grows on peanuts and corn (and in homes), produces the potent carcinogen Aflatoxin (causes liver can cer). Fusarium mold which grows on corn produces the carcinogen Fumonisin B1 and causes esophageal cancer. Esophageal cancer from Fumonisin B1 contaminated corn is observed in peo ple living in Italy, Iran, Kenya, Zimbabwe, United States and Brazil. Government but currently five non-cancer causing mold tox ins, the ones most commonly found on corn and grains, are strictly regulated by the E. Many such as Gliotoxin (produced by the common indoor molds Aspergillus fumigatus, A. Gliotoxin is a well studied mold toxin and has long been fingered as the main chemical player contributing to the vir ulence of A. For studies on how the mold toxin Gliotoxin can compromise human im mune system response see the following links (, , , , , , , ). Although not common, molds have been found growing in the brain as well as the lungs. The Thrasher paper has an excel lent, concise review of molds and their secondary metabolites (toxins/immunosuppresives). Neurotoxic Mycotoxins Some commonly occurring mold toxins can cause Neurological problems such as: Hheadaches, short term memory loss, attention deficit problems, anxiety, neurological impairment in children and other problems. It is well established that some mycotoxins (toxins from Stachybotrys and Tricho derma both molds commonly found in water damaged homes) are neurotoxic and exposure to such neurotoxins can result in some degree of neurological impairment. Note that unless the individual is removed from the mycotoxin laden environment, or the environment is fixed, the individual cannot heal. Mycotoxins and the Gastrointestinal Tract Gut Microflora: Many or most mycotoxins of concern (including the well known mold toxin Penicil lin) exhibit strong anti-bacterial affects (bacteriocidal). Chronic exposure to even very low levels of these bacteriocidal toxins (at mold levels in many homes) can damage the good gut bacteria that make up our gut micro flora. Yeast/Candida secretes the powerful immunosuppressive Gliotoxin (the same causative agent pro duced by Aspergillus molds resulting in Invasive Aspergillosis) and Candida also secretes proteins so it can attach itself permanently to the intestinal lining. No carb/ no sugar diets, anti-fungals, probiotics and sometimes fecal transplants (all under Doctor supervision) are solutions to yeast over-growth. Again, unless the sick individual is removed from the mycotoxin laden environment they will not get better no matter how brilliant the doctor! Therefore no carb/ no sugar diets will be naturally low in consumed/ eaten mycotoxins.
Generic ibuprofen 400 mg without a prescription
The microbiome-gut-brain axis in health Food Standards Programme pacific pain treatment center victoria order ibuprofen with paypal, Secretariat of the Codex Ali and disease. Health and nutritional properties colorectal cancer is distinctive and predictive. Microbial therapy in liver disease: antidepressant-like effects and reverse the impact of chronic probiotics probe the microbiome-gut-liver-brain axis. Probiotics in irritable bowel syndrome: the science clear factor-kappaB and induce heat shock proteins in colonic and the evidence. Pharmabiotic manipulation of the selected strains of lactic acid bacteria on a human T leukemia microbiota in gastrointestinal disorders: a clinical perspective. Strain Demonstration of functionality in animal models of disease and in dependent induction of cytokine proles in the gut by orally human clinical trials. The gut microbiota and its essential role in dampening host proinammatory responses role in the development of allergic disease: a wider perspective. Bugs or drugs: are probiotics safe for use in the prevents physiological damages in a chronic low-grade inam critically ill The suppressive effect of probiotics for prevention of chemoradiotherapy-induced diar bidobacteria on Bacteroides vulgatus, a putative pathogenic rhea in people with abdominal and pelvic cancer: a systematic microbe in inammatory bowel disease. Constante M, Fragoso G, Lupien-Meilleur J, Calve A, postinfective gut dysfunction. Am J Physiol Gastrointest Liver Physiol Microbiota is essential for social development in the mouse. Bidobacterium Nissle 1917 ameliorates experimental colitis by modulating in infantis 35624 administration induces Foxp3 T regulatory cells in testinal permeability, the inammatory response and clinical human peripheral blood: potential role for myeloid and plas signs in a faecal transplantation model. Specic probiotic alters brain activity: a pilot study in patients with irritable bowel therapy attenuates antibiotic induced visceral hypersensitivity in syndrome. Limited Lactobacillus paracasei and its bacterial products to counteract prolonged effects of rifaximin treatment on irritable bowel stress-induced gut permeability and sensitivity increase in rats. Probiotic therapy of the Bidobacterium infantis 35624 displays visceral irritable bowel syndrome: why is the evidence still poor and what antinociceptive effects in the rat. A probiotic for ulcerative colitis: the Bidobacterium infantis 35624 on post-inammatory visceral culture wars continue. Eur J Clin Nutr 2018 Mar 26 [E-pub ahead of casei normalizes muscle hypercontractility in a murine model of print]. Metabolic benets of dietary Gastroenteritis therapies in developed countries: systematic prebiotics in human subjects: a systematic review of rando review and meta-analysis. Probiotics and pre improve eradication rate of Helicobacter pylori infection biotics. Infect Control Hosp Epidemiol 2018; terventions for recurrent abdominal pain in childhood. Interventions to reduce commensals in reinforcing intestinal barrier function and allevi acute and late adverse gastrointestinal effects of pelvic radio ating inammation. Probiotics for treating persistent diarrhoea in chil Conicts of interest the author discloses no conicts. These include ushing and other cutaneous of the response to treatment criteria, 67% of the patients in manifestations and neuropsychiatric symptoms (eg, headache and the cohort had either a complete or major regression in 10 poor concentration and memory). Akin is a consultant for Novartis and is on the Medical Advisory Board for the Mastocytosis Society. We believe this is a unique and 20-29 1 (6) underrecognized population of patients who might be encoun 30-39 4 (22) tered in various medical specialty clinics, especially allergy, 40-49 8 (44) immunology, and gastroenterology clinics. This study was designed and initiated 17 Standardization in Mastocytosis Working Conference, Vienna, Italy, 2005. The criteria used were consis Patients were included in the study on the basis of 3 criteria: (1) they had at tent with those proposed for the treatment of systemic mastocytosis in the least 4 of 6 clinical features (abdominal pain, diarrhea, ushing, headache, 17 Vienna Working Conference. Patients were excluded if they had another greater than 50%, a partial regression was improvement by 10% to 50%, primary medical disorder to explain their symptoms, such as pheochromocy and no regression was less than 10% improvement in symptoms. Se Statistics rum total and mature tryptase studies were performed at either the Virginia P values were determined by using the Student t test. A P value of less than Commonwealth University Laboratories (Richmond, Va) or Mayo Clinic Lab-. The most frequent application of mediator-targeting drugs, as proposed in the Standards and age group represented was 40 to 49 years (44% of patients). Plasma total and mature tryptase Poor concentration and memory 12 (67) levels were generally obtained on our patients to exclude systemic Diarrhea 12 (67) mastocytosis. In our cohort 5 (33%) of 15 patients who had a tryp Naso-ocular 7 (39) tase level measured had a positive result while in a baseline state. It Asthma 7 (39) is worth mentioning that none of the 3 patients in our cohort who Anaphylaxis 3 (17) were tested for the D816V c-Kit mutation from a bone marrow as pirate had a positive result on this test. In our cohort 10 (56%) of 18 tested patients had increased urine Importantly, patients were symptomatic for a mean of 4. A high incidence of allergies among the patients in our cohort Seven (44%) of the 16 tested patients in our cohort had increased was noted (6 [33%] patients). The most common ab depicted in Fig 1, 6 (33%) patients had a complete regression in dominal complaint was pain (17 [94%] patients), and 12 (67%) symptoms, 6 (33%) had a major regression, and 6 (33%) had a patients had diarrhea. Patients in our cohort either complained of ushing symptoms versus those who did not. Interestingly, we found that many patients with ushing also described intense 12); there was a more modest response to ushing (6/16). Of the patients in our cohort, 12 (67%) described intoler were followed for an average of 2. The remaining 4 patients had completely abstained from on the biopsy specimens available from the patients who had alcohol. All biopsy Headache was a common symptom and was elicited by history specimens evaluated were histologically normal (see Fig E1, A and in 15 (83%) of our patients. These tryptase tryptase Histamine (ng/24 h); patients were seen by multiple physicians in the ambulatory and (ng/mL); (ng/mL); (nmol/g creatinine); normal, emergency department setting, and many had been referred by Patient normal, normal, normal, 0-386 nmol/g 100-280 other allergists and gastroenterologists. The total number of patients in each response-to-treatment category is shown by using the criteria established for mastocytosis. Over the 4 years of the study, we estimate that 300 patients vation in our cohort because many of our control population were initially seen at our allergy clinic by 1 provider (M.