
Microzide
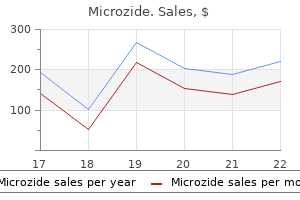
Purchase microzide 12.5mg online
There is no information concerning the impact of the thulium laser on prostate volume or the impact of any laser therapy on the transition zone volume blood pressure 60 over 0 25mg microzide for sale. The literature does not contain information concerning the impact of the various laser therapies on the detrusor pressures at maximum flow. Randomized controlled studies of the holmium laser compared to open prostatectomy found a total withdrawal rate of 38. The concerns for mortality rates associated with laser therapies are referred to the section addressing mortality for all surgical therapies. Intraoperative, immediate, postoperative, and short-term complications involve a broad spectrum of events and reporting rates may be based on subjective thresholds. The ability to directly compare laser therapies with respect to the operative time is constrained by the fact that each laser modality seems to select from patient populations with different baseline characteristics and seldom selects the same comparison therapy as a control. This is in contrast to a cohort comparison study that reported operative times were similar despite greater tissue resection with holmium enucleation. However, other studies reported enucleation times of 86 minutes in a large series, which was 255 improved from 112 minutes in their initial series of 118 cases. The longest mean operative time was reported in a series by Kuo et al (2003) (133. A single-cohort study reported that the average weight of prostate tissue resected 294 was 11 g and the procedure required an average operative time of 47 minutes. The sole study for the thulium laser is a single-cohort study reporting an operative time of 52 minutes in men with a mean pretreatment prostate volume of 32 mL. The published data in the interval from the 2003 analysis of the literature does not provide sufficient information to assess a change in risk. This rate is higher than expected from other transurethral technologies available today and the reason for the difference is not clear. Minimally invasive and surgical procedures induce irritative voiding symptoms immediately after and for some time subsequent to the procedure. Periprocedure and postprocedure adverse events associated with voiding symptoms include frequency, urgency, and urge incontinence and are categorized as postprocedure irritative adverse events. Such events are reported more often following heat-based therapies than following tissue-ablative surgical procedures. Because they impact QoL, irritative events are important and warrant documentation. Unfortunately, all patients will have some symptoms during the healing process immediately following the procedure. Because there is no standard for reporting this outcome, some studies reported these early symptoms while others did not. Further, because it is not possible to stratify these complaints according to severity, it is not possible to compare the degree of bother of these symptoms across therapies. Further, new technologies are resulting in earlier removal of catheters with much shorter hospital stays. The earlier attempts to remove the catheter are likely to increase the reported rates of repeat catheterization compared to historical rates associated with other technologies and longer hospital stays. Randomized controlled studies also showed a shorter length of 263, 294 stay for patients treated with holmium resection of the prostate. This wide range is believed to be a reflection of the change in technology over the review period as the laser energy increased in increments from 40W to 100W over time. In addition, various protocols in select institutions facilitated early discharge from the hospital. The average hospital stay reported in the study 253 utilizing the thulium laser was 3. The category urinary incontinence represents a heterogeneous group of adverse events, including total and partial urinary incontinence, temporary or persistent incontinence, and stress or urge incontinence. Secondary procedures, defined as interventions rendered by the treating physician for the same underlying condition as the first intervention, are challenging to classify. Examples of such procedures include initiation of medical therapy following a minimally invasive or surgical treatment, minimally invasive treatment following surgical intervention, or surgical intervention following a minimally invasive treatment. First, the threshold for initiating a secondary procedure varies by patient, physician, and the patient-physician interaction. In the absence of clearly defined thresholds for the success or failure of an initial intervention, secondary procedures are initiated on the basis of subjective perceptions on the part of either patients or treating physicians, which may not be reproducible or comparable between investigators, trials, or interventions. Moreover, the duration of trials and follow-up periods both affect rates at which secondary procedures are performed. Thus, although patients receiving longterm follow-up are at greater risk for treatment failure than those followed for short periods, it is virtually impossible to construct Kaplan-Meier curves or perform survival analyses for secondary procedure rates. As a result, the estimates for secondary procedure rates should be viewed with caution. Reoperation rates following various laser therapies are inconsistently reported, often due to the limited length of follow-up or the small numbers of patients in these studies. Inclusion and exclusion criteria were generally similar across studies, excluding subjects with prior pelvic surgery, prostate cancer, and neurologic disorders. The mean age of study participants was similar across studies, ranging between approximately 65 and 70 years. There was significant variation in Qmax at baseline, ranging from two to 20 mL per second in individual treatment groups. There was also much variation in preoperative prostate gland size: one study examined small glands (mean prostate volume of treatment 305 groups ranged from 24 to 34 mL), while another examined larger glands (mean of treatment groups, 308 54 mL and 63 mL). In studies where post-void residual was compared between treatments, no significant differences were found, with improvements noted with both 302, 304, 306, 308-311 treatments. Safety Outcomes Withdrawals and Treatment Failure Withdrawal rates were only reported in three of the 10 trials, with high rates of attrition when follow-up was two years or more. Mortality rates were low, largely due to cardiovascular disease, and never attributed to the surgical intervention. Longer-term Adverse Events Urethral stricture and bladder neck stenosis were uncommon and occurred with both treatments. Total sample size ranged between 40 and 240 subjects and follow-up intervals 319 323 varied between three weeks and 21 months. Cohort Studies with a Comparison Group 325, 326 We identified two cohort studies with comparison groups. Methods for recruiting subjects or identifying the study cohort were not generally reported. Sample size varied greatly (ranging from 21 to 1,014 327, 335, 336, 339, 342-344 participants), and seven studies had a sample size greater than 200 participants. Three studies examined the Gyrus Plasmakinetic 328, 334, 335 327 (bipolar) system and another a coagulating intermittent cutting device. Postvoid residual decreased significantly in all studies and Qmax increased in all studies in the 334, 342 range of 6 to 10 mL per second. Predictors of Efficacy and Effectiveness Outcomes Several studies examined the relationship between various demographic and clinical 337, 340, 343-345 characteristics and efficacy or effectiveness outcomes. Machino and colleagues (2002) categorized 62 patients into those with equivocal obstruction and those with obstructive symptoms, as 337 defined by the Abrams-Griffins nomograph. Preoperative obstruction grade (Schafer) correlated with improvements in obstruction grade, symptom 345 index, and QoL. Only one of the randomized and the two nonrandomized studies showed a reduction in blood loss or transfusion requirements. Other studies found no significant differences between the treatment group and placebo for blood loss during surgery, excessive or severe bleeding, 362 or clot retention. Yanoshak S, Roehrborn C, Girman C et al: Use of a prostate model to assist in training for digital rectal examination. Roehrborn C, Sech S, Montoya J et al: Interexaminer reliability and validity of a threedimensional model to assess prostate volume by digital rectal examination. Crawford E, Wilson S, McConnell J et al: Baseline factors as predictors of clinical progression of benign prostatic hyperplasia in men treated with placebo. Djavan B, Fong Y, Harik M et al: Longitudinal study of men with mild symptoms of bladder outlet obstruction treated with watchful waiting for four years. Temml C, Brossner C, Schatzl G et al: the natural history of lower urinary tract symptoms over five years.
Diseases
- Spinal cord injury
- Spondylarthritis
- Athetosis
- Brachydactyly scoliosis carpal fusion
- Dermal dysplasia
- Nystagmus, central
- Raine syndrome
Discount microzide 12.5 mg with amex
Researchers have demonstrated that induction of labor for any reason increases the risk for a number of complications for women and infants ulterior motive meaning buy microzide with visa. Induced labor results in more postpartum hemorrhage than spontaneous labor, which increases the risk for blood transfusion, hysterectomy, placenta implantation abnormalities in future pregnancies, a longer hospital stay, and more hospital re-admissions. Induction of labor is also associated with a signifcantly 11 higher risk of cesarean birth. For infants, a number of negative health efects are associated with induction, including increased fetal stress and respiratory illness. Research on the risk-to-beneft ratio of elective augmentation of labor is limited. However, many of the risks associated with elective induction may extend to augmentation. In a recent systematic review, the authors found that women with slow progress in the frst stage of spontaneous labor who underwent augmentation with exogenous oxytocin, compared with women who did not receive oxytocin, had similar rates of cesarean. Such results call into question a primary rationale for labor augmentation, which is the reduction of cesarean surgery. In addition to the serious health problems associated with non-medically indicated induction of labor, hospitals, insurers, providers and women must consider a number of fnancial implications associated with the practice. Further, women who deliver vaginally have shorter hospital stays, fewer hospital readmissions, faster recoveries and fewer infections than those who have cesareans. Prescription opioids are among the most efective medications for the treatment of pain. However, regular or long-term use of opioids can create physical dependence and in some cases, addiction. Women who are prescribed, or continue to use, opioids during pregnancy may not understand the risks to themselves or their babies. Women using opioids during pregnancy were shown to have higher rates of depression, anxiety and chronic medical conditions as well as increased risks for preterm labor, poor fetal growth and stillbirth. Women who used opioids during pregnancy were four times as likely to have a prolonged hospital stay compared to nonusers and incurred signifcantly more per-hospitalization cost. In utero exposure to these substances can cause a newborn to experience withdrawal symptoms after birth. Instead, help the mother to place her newborn in skin-to-skin contact immediately after birth and encourage her to keep her newborn in her room during hospitalization after the birth. Keeping mothers and newborns together promotes maternal-infant attachment, early and sustained breastfeeding and physiologic stability. Early 13 initiation of skin-to-skin care and breastfeeding promotes optimal outcomes and can signifcantly reduce morbidity for healthy term and preterm or vulnerable newborns. Breastfeeding is the ideal form of infant nutrition and should be the societal norm. Given the numerous health benefts for infant and mother and the health care cost savings associated with breastfeeding, breastfeeding has become a global public health initiative that can improve the overall health of nations. The most important step in treating delirium is identifying, removing and treating the underlying cause(s) of delirium. Delirium is often a direct physiological consequence of another medical condition, substance intoxication or withdrawal, exposure to a toxin, or is due to multiple etiologies. Because numerous medications or medication classes are associated with the development of delirium. In terms of delirium prevention, it is recommended health systems should implement multicomponent, nonpharmacologic interventions that are delivered consistently throughout hospitalization by the interdisciplinary team. Delirium is common in older adults, especially in the hospital setting, yet delirium is frequently unrecognized and not documented by nursing or 15 medical staf. Delirium is associated with very poor clinical outcomes, including prolonged length of stay, high costs and lower quality of life for older adults when not detected early. Delirium is treatable and often reversible and dementia is not, so mislabeling older adults with dementia may miss a life threatening underlying condition causing the delirium such as an infection, medication side efect or subdural hematoma. Children have an increased risk of cancer with exposure to higher cumulative 16 radiation doses. Febrile seizures are the most commonly occurring seizures in the frst 60 months of life. Classic spine surgical treatment involves bilateral dissection of paraspinal muscles to expose the involved levels. Treatment of these spasms should include both pharmacologic and non-pharmacologic interventions. Age-related changes in adults 18 can afect both metabolism and drug elimination in the body, resulting in a prolonged half-life for medications. Among the benzodiazepines, diazepam is particularly problematic due to its long half-life and many active metabolites. Benzodiazepines can lead to over-sedation, potential for respiratory depression, increased risk of delirium, and extended in-hospital recovery time. Benzodiazepines have consistently been associated with falls in the aging population and should be avoided. Efective non-pharmacological interventions for use include heat, cold, repositioning, and massage. Medical and surgical treatment decisions are based on relieving intracranial pressure. Inaccurate pressure readings can lead to unnecessary surgeries such as cranial vault expansion, shunt revisions and placement of lumbar-peritoneal shunts as well as unnecessary medical treatments. It is 20 associated with an increased risk of aspiration, pneumonia, prolonged hospital stay, disability, and death. Swallow screening is critical in the rapid identifcation of risk of aspiration in patients presenting with acute stroke symptoms. Because formal swallowing evaluation is not warranted in all patients with acute stroke, the purpose of a swallowing screen is to identify those who do not need a formal evaluation and who can safely take food and medication by mouth. Thromboembolic disease is a signifcant cause of complications and mortality in hospitalized patients and a growing public health issue. However, when pulse oximetry and physiologic monitoring are used inappropriately, signifcant cost burdens can afect the entire healthcare system. In addition, the high number of alarm alerts and level of noise created by these alarms leads to alarm fatigue. When high levels of false alarms occur in the work environment, clinically signifcant alarms may be masked by being silenced or unrecognized when clinicians become desensitized. Continuous bedside monitoring should not be used in place of hourly safety checks. Clinical instability is defned by physiologic criteria such as age-specifc tachycardia or hypotension, tachypnea, low urine output, altered mental status, or any signifcant clinical deterioration that warrants increased level of care and investigation. Therefore, the routine use of repeat laboratories studies in children with isolated solid organ injury who have physiologically normal vital signs for their age is not necessary. Despite the high human and dollar costs associated with these symptoms, their treatment continues to challenge practitioners and remains a top research priority in long-term care settings. Removing hair at the surgical site has long been believed to be associated with an increased rate of surgical site infections because of razor-induced microtrauma. Postoperative wound infections increase the costs and the length of hospital stay. For example, during emergent craniotomies or any time a surgeon deems hair removal necessary for the surgical procedure. When hair removal is necessary, hair at the surgical site should be removed by clipping or depilatory methods. In a landmark nonexperimental study of 23,649 surgical wounds, Cruse (1973) found a 2. In addition, most patients dread the thought of having the hair on their head removed, and hair shaving can negatively afect their body image. How this List Was Created the American Academy of Nursing has convened a workgroup of member fellows who are leaders of professional nursing organizations representing a broad range of clinical expertise, practice settings and patient populations. An extensive literature search and review of practice guidelines is conducted for each new proposed recommendation for the list. The supporting evidence is then reviewed by the respective nursing organization(s) with the most relevant expertise to each recommendation. The Academy workgroup fellows narrow the recommendations through consensus, based on established criteria. How nurses decide to ambulate hospitalized older adults: development of a conceptual model. Impact of a nurse-driven mobility protocol on functional decline in hospitalized older adults.

12.5mg microzide
Rehabilitation outcomes following traumatic spinal cord injury in a tertiary spinal cord injury centre: a comparison with an international standard arrhythmia upon waking buy microzide paypal. Beneficial effect of intranasal desmopressin for men with benign prostatic hyperplasia and nocturia: preliminary results. Incidence and severity of vesicoureteral reflux in children related to age, gender, race and diagnosis. Safety and efficacy of transurethral resection of the prostate under sedoanalgesia. Evaluation of nuclear matrix protein-22 as a clinical diagnostic marker for bladder cancer. Correlation between serum prostate specific antigen and prostate volume in Taiwanese men with biopsy proven benign prostatic hyperplasia. Clinical study of benign prostatic disease, current concepts and future prospects: randomized controlled trials versus real life practice. Lower urinary tract symptoms suggestive of benign prostatic obstruction-Triumph: design and implementation. Randomized controlled trials for benign prostatic obstruction: problems and pitfalls. Differential diagnosis of prostate cancer and benign prostate hyperplasia using twodimensional electrophoresis. Two-dimensional electrophoresis of prostatespecific antigen in sera of men with prostate cancer or benign prostate hyperplasia. Sleep apnea symptoms, nocturia, and diabetes in African-American community dwelling older adults. Comparison of once and twice daily dosage forms of Pygeum africanum extract in patients with benign prostatic hyperplasia: a randomized, double-blind study, with longterm open label extension. The role of the androgen receptor in the development of prostatic hyperplasia and prostate cancer. Successful voiding after trial without catheter is not synonymous with recovery of bladder function after colorectal surgery. Prenatal diagnosis of cystic bladder distension secondary to obstructive uropathy. Comparison of ofloxacin and norfloxacin concentration in prostatic tissues in patients undergoing transurethral resection of the prostate. The correlation between clinical outcome and residual prostatic weight ratio after transurethral resection of the prostate for benign prostatic hyperplasia. Hemolysis in transurethral resection of the prostate using distilled water as the irrigant. Lower urinary tract symptoms and uroflow in a community-based sample of Taiwanese men. Hepsin and maspin are inversely expressed in laser capture microdissectioned prostate cancer. Clinical investigation on the correlation between lower urinary tract infection and cystitis glandularis. Is surveillance necessary for inverted papilloma in the urinary bladder and urethrafi. Diagnosing symptomatic urinary tract infections in infants by catheter urine culture. Pediatric transperitoneal laparoscopic partial nephrectomy: comparison with an age-matched group undergoing open surgery. Endoscopic puncture of ureterocele as a minimally invasive and effective long-term procedure in children. The impact of polymorphism on prostate specific antigen gene on the risk, tumor volume and pathological stage of prostate cancer. Human kallikrein-2 gene polymorphism is associated with the occurrence of prostate cancer. Pilot study of transperineal injection of dehydrated ethanol in the treatment of prostatic obstruction. Results of holmium laser resection of the prostate for benign prostatic hyperplasia. Nephroureterectomy for transitional cell carcinoma the value of pre-operative histology. Peripheral hypoechoic lesions of the prostate: evaluation with color and power Doppler ultrasound. Is the higher prevalence of benign prostatic hyperplasia related to lower urinary tract symptoms in Korean men due to a high transition zone indexfi. Expression of senescence-associated beta-galactosidase in enlarged prostates from men with benign prostatic hyperplasia. Prostate carcinoma risk subsequent to diagnosis of benign prostatic hyperplasia: a population-based cohort study in Sweden. Superficial transitional cell carcinoma of the ureteral orifice: higher risk of developing subsequent upper urinary tract tumors. A comparison of sonourethrography and retrograde urethrography in evaluation of anterior urethral strictures. Expression of vascular endothelial growth factor in primary superficial bladder cancer. Initiation of nonselective alpha1-antagonist therapy and occurrence of hypotension-related adverse events among men with benign prostatic hyperplasia: a retrospective cohort study. Prostate tissue and leukocyte levels of n-3 polyunsaturated fatty acids in men with benign prostate hyperplasia or prostate cancer. Microsatellite alterations in urinary sediments from patients with cystitis and bladder cancer. Risk assessment of renal cortical scarring with urinary tract infection by clinical features and ultrasonography. Double-blind randomized comparison of single-dose ciprofloxacin versus intravenous cefazolin in patients undergoing outpatient endourologic surgery. Combination of ballistic lithotripsy and transurethral prostatectomy in bladder stones with benign prostatic hyperplasia: report of 120 cases. Toxicological effects of in utero and lactational exposure of rats to a mixture of environmental contaminants detected in Canadian Arctic human populations. Change in International Prostate Symptom Score after transurethral prostatectomy in Taiwanese men with benign prostate hyperplasia: use of these changes to predict the outcome. Botulinum toxin type A improves benign prostatic hyperplasia symptoms in patients with small prostates. Sustained beneficial effects of intraprostatic botulinum toxin type A on lower urinary tract symptoms and quality of life in men with benign prostatic hyperplasia. Intraprostatic injection of botulinum toxin type-A relieves bladder outlet obstruction in human and induces prostate apoptosis in dogs. Dual effects of ouabain on the regulation of proliferation and apoptosis in human prostatic smooth muscle cells. Long-term follow-up study to evaluate the efficacy and safety of the doxazosin gastrointestinal therapeutic system in patients with benign prostatic hyperplasia with or without concomitant hypertension. Relationship between serum prostate-specific antigen and prostate volume in Korean men with benign prostatic hyperplasia: a multicentre study. Doxazosin for benign prostatic hyperplasia: an open-label, baselinecontrolled study in Korean general practice. Long-term outcome of radiation-based conservation therapy for invasive bladder cancer. Transperineal sonography guided biopsy of the prostate: critical review of 1107 cases. Randomized clinical trial comparing transurethral needle ablation with transurethral resection of the prostate for the treatment of benign prostatic hyperplasia: results at 18 months. Standard versus hydrophilic catheterization in the adjuvant treatment of patients with superficial bladder cancer. Marked suppression of dihydrotestosterone in men with benign prostatic hyperplasia by dutasteride, a dual 5alphareductase inhibitor.
Buy microzide 12.5 mg on line
Cervical or vaginal preparation before a C-section l Gently wash the external genital area with soap and clean water and dry the area before applying the antiseptic arteria zarobki buy generic microzide 12.5 mg line. It is not necessary to prepare the external genital area with antiseptic solution if it appears clean. Infection prevention measures related to surgical technique Good surgical techniques minimize tissue trauma, control bleeding, eliminate dead space, remove dead tissue and foreign bodies, use minimal sutures, and maintain adequate blood supply and oxygenation the following recommendations apply specifically for C-section or require special emphasis: l Make the skin incision with a scalpel rather than with electrocautery. Change a sterile surgical glove (or gloves) immediately when contamination occurs, before touching a sterile area (see Module 3, Chapter 1, Personal Protective Equipment, for how to change gloves). Infection and Prevention Control: Module 10, Chapter 5 99 Preventing Maternal and Newborn Infections in Health Care Settings l Do not explore the peritoneal cavity unless absolutely necessary. If necessary, then perform only after closure of the uterine incision and changing to a pair of new surgical gloves. See the Infection Prevention and Control Interventions after Delivery: Care of the Newborn section below. It should be done only in the presence of dense substances blocking the nose and mouth. Use a separate square for each eye and wipe from the inner corner to the outer corner. In the presence of meconium-stained amniotic fluid: l Do not perform tracheal suctioning and avoid suctioning of the mouth and nose before initiating positive pressure ventilation for infants who do not start breathing on their own. Manage expressing and storage of breast milk carefully to prevent infection (see the Breast milk handling and storage section in this chapter). Infection and Prevention Control: Module 10, Chapter 5 103 Preventing Maternal and Newborn Infections in Health Care Settings l Manage the preparation of formula (See Module 5, Chapter 3, Managing Food and Water Services in Health Care Facilities. Use of chlorhexidine in these situations may help prevent application of harmful traditional substance, such as cow dung, to the cord stump. Immunizations and post-exposure prophylaxis l Provide non-live vaccines to medically stable infants (including premature infants) according to the national immunization schedule for age. Careful hand hygiene between patients is most likely of more benefit than the length of hand scrub upon entry to the nursery. However, because newborns require such small doses, cost-effectiveness may be an inhibiting factor in limited-resource settings (see Module 4, Chapter 1, Injection Safety). There is no known benefit, it takes resources, and hands may become contaminated when putting on and removing them. Although some absorption has been documented, no systemic effects have so far been identified. Once an outbreak is suspected, investigation and measures to halt any further spread should be implemented promptly. During an outbreak, control measures should be monitored along with any new infections to make sure that they have been effective and the problem is resolving. Phenol has been known to cause neonatal hyperbilirubinemia and hexachlorophene has been associated with neurotoxicity. Infections have been associated with contaminated breast milk pumps and refrigerated storage practices. Clean the containers with hot, soapy water after each use, before they are sterilized. Infection and Prevention Control: Module 10, Chapter 5 111 Preventing Maternal and Newborn Infections in Health Care Settings Formula preparation and care Powdered infant formula is not sterile and can be contaminated by the manufacturer, after the formula container is opened, during the preparation, or during storage. Summary Maternal and newborn care is unique and complex, requiring the simultaneous care of two interdependent patients. Typically, early-onset sepsis is considered to be maternally acquired, usually from the maternal genital tract. The choice of dose within that range should be guided by which formulations of penicillin G are readily available to reduce the need for pharmacies to specially prepare doses. For penicillin-allergic patients who do not have a history of those reactions, cefazolin is the preferred agent because pharmacologic data suggest it achieves effective intra-amniotic concentrations. Vancomycin and clindamycin should be reserved for penicillin-allergic women at high risk for anaphylaxis. During nursery outbreaks, cohorting ill and colonized infants is recommended, as are good hand hygiene practices. Because antenatal testing is not available in most low-income countries, use of eye drops is the only preventive measure usually available. Unfortunately, neither tetracycline nor erythromycin eye drops prevents chlamydial pneumonia. When caring for patients with chlamydial conjunctivitis or pneumonia and mothers with genital chlamydia, use Standard Precautions. Most severe manifestations of gonorrhea in newborns are ophthalmia neonatorum (a condition of the eye that may result in blindness) and sepsis. Prevention of gonorrhea during pregnancy includes screening, diagnosis, and treatment of infected pregnant women using appropriate antibiotics (tetracycline should not be used because it is deposited in the teeth of the developing fetus). Because antenatal testing is not available in most low-income countries, use of eye drops (tetracycline or erythromycin) is the only preventive measure usually available. When caring for patients with ophthalmia neonatorum and mothers with gonorrhea infection, use Standard Precautions. Infection and Prevention Control: Module 10, Chapter 5 115 Preventing Maternal and Newborn Infections in Health Care Settings Listeriosis Listeriosis is predominantly a foodborne infection caused by Listeria monocytogenes. Infection during pregnancy can cause fetal loss, preterm labor, and illness or death in newborn infants. Similar to group B streptococcal disease, listeriosis can present as an earlyor late-onset syndrome. An erythematous rash with small pale papules can also occur in early onset with severe newborn infection. Immunocompetent patients with mild infections can be treated with ampicillin alone. Additionally, immunizing mothers with the tetanus vaccine, which is inexpensive and effective, is essential for prevention. Infants become infected during childbirth through use of an unclean instrument to cut the umbilical cord or following childbirth by placement of substances heavily contaminated with tetanus endospores. To be effective, non-immunized pregnant women should receive at least two doses of tetanus toxoid prior to childbirth. If there is sufficient time before childbirth, two doses should be administered at least 4 weeks apart, and the second dose should be given at least 2 weeks before childbirth. When caring for patients with tetanus, use Standard Precautions, as this infection is not transmitted from person to person. It is transmitted through sexual contact with an infected partner and is also transmitted from mother to child during pregnancy. Antenatal testing of pregnant women should be done to identify and treat women who are seropositive for syphilis and to prevent congenital syphilis in their newborns. If the results of serologic tests for syphilis are equivocal or not available, a cord blood or venous sample from the newborn should be tested. Regardless of stage of pregnancy, infected women should be treated with penicillin according to the dosage appropriate for the stage of syphilis as recommended for non-pregnant patients. Standard Precautions apply to all patients (women and their babies) irrespective of their hepatitis B vaccine status or disease status. Care is aimed at maintaining comfort and adequate nutritional balance, including replacement of fluids that are lost from vomiting and diarrhea. Breastfeeding is not contraindicated, but if her nipples are cracked and bleeding, the mother may wish to abstain. However, it is often difficult to determine whether or not an infection is recurrent or primary. Mothers can continue to breastfeed their babies, provided there are no lesions in the breast area and all skin lesions are covered.
Forget Me Not (Forget-Me-Not). Microzide.
- Dosing considerations for Forget-me-not.
- What is Forget-me-not?
- Are there safety concerns?
- How does Forget-me-not work?
- Lung problems and nosebleeds.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96503
Order generic microzide line
Electrolyte reand the azole drugs (clotrimazole and placement is another important adjunct of amphomiconazole) prehypertension american heart association generic 25mg microzide free shipping. New preparations of amphotericin B are now available Most species of fungi are susceptible to it, and although that add different lipids (fats! The addition of the most serious systemic fungal infections: lipid decreases the nephrotoxicity of the drug, making it Systemic Candida i nfections. Rigors still Severe pneumonia and extrapulmonary Blastomycooccur but nephrotoxicity is reduced. Less nephotoxicity is seen, but Adverse Effects once again we do not yet know enough about antifungal efficacy. Remember that most antimetabolite type drugs will do this (methotrexate, sulfa Flucytosine drugs, 5-fluorouracil, etc. This again is comFlucytosine is rarely used alone because of rapid demon with the antimetabolites, such as the chemotheravelopment of resistance. Like ketoconazole it is used for cutaneous Candida inthe Azole Family fections but it is also used as a second-line agent behind amphotericin B for systemic candidiasis and cryptococthe azole family may be classified into 2 groups of meningitis. The de2) A single dose of fluconazole very effectively clears pletion of ergosterol disrupts the permeability of the candida vaginitis. Itraconazole Clotrimazole and miconazole are too toxic for systemic use and for this reason, are primarily used for this triazole is becoming the next amphotericin B but topical fungal infections, including pityriasis versiin an oral formulation without the many amphoterrible color, cutaneous candidiasis, and the dermatophytosis side effects!!! Clotrimazole troches (like Itraconazole is now used as first-line treatment candies) are sucked to treat oral Candida (thrush), and for chromoblastomycosis, histoplasmosis, coccidioidoclotrimazole vaginal suppositories treat Candida mycosis, blastomycosis, and possibly for invasive vaginitis. The main problem with this drug is Ketoconazole, fluconazole, and itraconazole are poor oral absorption. Taking it with acid drinks tolerated orally and have many important uses for syssuch as orange juice or colas enhances absorption temic fungal infections. Ketoconazole Ketoconazole, one of the imidazoles, is the drug of Voriconazole choice for chronic mucocutaneous candidiasis (Candida on every surface). Alzole is currently not used for the treatment of systemic though more clinical experience is needed, data are suffungal infections. The safer, more efficacious, oral itraficient to support its future use in patients with invasive conazole and old faithful, amphotericin B, are the first aspergillosis who have failed to respond to agents of line drugs. Nystatin 3) Inhibition of testosterone synthesis: Ketoconazole inhibits the cytochrome P-450 system, which is Nystatin, like amphotericin B, binds to ergosterol, inimportant in testosterone synthesis. The result is gycreasing the permeability of the cell membrane and causing cell lysis. Griseofulvin Also, since it is not absorbed from the gastrointestinal tract, oral nystatin can be used to treat oral and Fig. You will orcram used to lever the dermatophyte plaques off the der nystatin on the wards as Nystatin, Swish and skin. Griseofulvin deposits in keratin precursor cells in the skin, hair, and nails, where it inhibits the growth Fig. Terbinafine tends to accumulate normal cell turnover, this translates into a slow cure i n nails, and is therefore useful for tinea unguium of skin fungus. It also appears useful in the treatAdverse effects of griseofulvin are uncommon. Terbinafine Recommended Review Articles: Terbinafine is a new oral fungicidal agent that blocks fungal cell wall synthesis. Certain viruses are further enclosed by an external lipid bilayer membrane that surrounds the capsid and may contain glycoproteins. The genetic material contains instructions to make millions of clones of the original virus. Viruses contain all of the genetic information, but not the enzymes, needed to build millions of replicas of the original virus. The nucleic acid strands can be single-stranded, doublestranded, linear, or looped, in separate segments or one continuous strand. The nucleic acid sequences can enFigure 22-1 code a simple message or encode hundreds of enzymes and structural proteins. Imagine that a virus is a specially designed military spaceship with a super-resistant outer shell. Here is the confusing part: the they are not able to begin translation immediately. Take 1 or more polypeptide chains and organize them into a globular protein subunit. Most of these assume a spherical shape except for the rhabdoviruses (rabies virus), which have a bullet-shaped capsid. Viruses acquire this membrane by budding through the host cell nuclear or cytoplasmic membrane and tearing off a piece of the membrane as they leave There may be various glycoproteins embedded in their cell membranes. The appearance of the complete viruses 2) Capsid: and their approximate sizes compared to the bacterium Icosahedral E. Then they copy the viral genetic material enough times so that a copy can be placed in 1) Parvoviridae: this virus is so simple that it only each newly constructed virus. This feature forces the 2) Poxviridae: this virus is at the opposite end of host cell to construct only viral proteins and copies of the spectrum and is extremely complex. Herpes Hepadna Pox 4) Release of virions from the host cell (either by lyThree are naked: A woman must be naked for the sis or budding). This internalization occurs by show helical capsid symmetry, and replicate in the endocytosis or by fusion of the virion envelope with the cytoplasm: host cell membrane. Toga Orthomyxo Corona Paramyxo Uncoating Retro Rhabdo the nucleic acid is released from the capsid into the Picorna Bunya nucleus or cytoplasm. Thus, viral transcription is divided into immediate early, early, and late transcription. The paramyxoviridae include parainfluenza virus, mumps, measles, and respiratory syncytial virus. The ability to produce epidemics and susceptibility to antibody immunity d vaccination all depend on the viral ultrastructure. You will see at the end of this section that the paramyxoviridae have a similar structure with a few small changes (making it oh so easy to learn! Surrounding the nucleocapsid lies an outer membrane studded with long glycoprotein spikes. Anchoring the bases of each of these spikes on the inside of the viral lipid bilayer are membrane proteins (M-proteins). Major mutational changes usually result in altered codon reading There are 3 types of influenza virus: A, B, and C. Type A infects humans, other Q: We all think that this is a pesky but mild self-limmammals (swine, etc. So why have there been about epidemiology arise: devastating pandemics of influenza throughout history, as in 1918fi We are taking the boat mentioned above and H5N1) was transmitted from infected poultry to humans airlifting it to a mountain in the Himalayas. So the entire human population would be susceptible, leadEven the normal yearly flu can cause complicaing to devastating pandemics. The viral was caused by a virus with an H2 hemagglutinin, the infection also lowers the host defenses against pandemic of 1900 was caused by a new virus with H3 many bacteria. The chart below is only inpatients (especially the elderly) closely until complete cluded to demonstrate the many pandemics and their resolution of their illness. Study the figure of the child with the crown (the ReySpanish for king) and the lightning bolts 1989: H2N2 around his head and liver. Virus isolation: Culture of the virus allows for genetic and antigenic analysis "Notice also that some strains caused a second pan2. Detection of viral proteins: New one hour tests help demic as a new unexposed population grows to adulthood. Serological diagnosis: 4-fold increase in specific antigenic drift and antigenic shift. Respiratory syncytial virus and parainfluenza virus both cause lower respiratory infections (pneumonia) in children and upper respiratory tract infections (bad colds) in adults.
Purchase 25 mg microzide free shipping
While some interventions are relatively inexpensive at the individual level (such as foot screening) arrhythmia cheap microzide, they can be costly at a societal level, considering the millions of people with diabetes. Other interventions are costly at the individual level (such as custom-made footwear), but reduce ulcer recurrence risk to a level that they are expected to be cost-saving at a societal level. Future research is needed to explore the potential of a more personalised medicine approach in diabetic foot ulcer prevention, so to deliver the right treatment, to the right person, at the right time. Future research should assess the effectiveness of various educational interventions, as well as the frequency of education provided. This includes but is not limited to motivational behavioural interventions, e-health applications and (online) social support systems by peers or health professionals. These interventions may include, among others, assistive technology, educational interventions or shoe technical solutions. High quality data on the benefit of interventions to prevent a first foot ulcer are scarce. As the event rate (foot ulceration) is relatively low in a population without a previous ulcer, large groups of patients need to be targeted and it is unclear if the benefits will outweigh harm and costs. Studies are urgently needed to better define the categories of patients that will benefit from preventative interventions and what specific types of interventions should be included. The exact role of these surgical procedures compared to conservative approaches in the prevention of ulceration is still unclear, and requires appropriately designed controlled studies. Reducing the risk of ulceration also reduces the risk of infection, hospitalization, and lower-extremity amputation in these patient. While not drawing most attention of clinicians and researchers, foot ulcer prevention is the best way to prevent severe morbidity and mortality in people with diabetes. We think that following the recommendations for preventative treatment in this guideline will help health care professionals and teams provide better care for diabetic patients who are at risk of ulceration. We encourage our colleagues, both those working in primary care and in diabetic foot clinics, to consider developing forms of surveillance. We also encourage our research colleagues to consider our key controversies and considerations and conduct properly-designed studies (17) in areas of prevention in which we find gaps in the evidence base, so to better inform the diabetic foot community on effective treatment for preventing a foot ulcer in a persons with diabetes. Adequately trained healthcare professional: a person who according to national or regional standards has the knowledge, expertise, and skills to perform a specified task in screening, examining, or managing a person with diabetes who is at risk of foot ulceration. This may also incorporate other features, such as a metatarsal pad or metatarsal bar. Even greater depth is sometimes provided in footwear that is referred to as double depth or super extra-depth. Foot-related exercises: Any physical exercise specifically targeting the foot or lower-extremity with the aim of changing foot function. These exercises can include stretching and strengthening of the foot and ankle musculature and functional exercises such as balance and gait training. Foot self-care: Foot care interventions the patient can do at home, consisting of but not limited to: foot inspection, washing of feet, careful drying between the toes, nail cutting, using emollients to lubricate skin, not using chemical agents or plasters to remove callus, footwear inspection, avoidance of walking barefoot or on socks only or in thin-soled slippers, avoidance of wearing tight socks, avoiding exposure to excessive cold and heat. Foot self-management: Advanced assistive interventions the patient can use at home, consisting of but not limited to: home monitoring systems, lifestyle interventions, telemedicine, technological applications, peer support programs. Footwear modification: Modification to existing footwear with an intended therapeutic effect. In-shoe (semi-)rigid orthosis: Term used for device put inside the shoe to achieve pressure reduction or alteration in the function of the foot. Also known as pedorthic footwear Off-the-shelf footwear: Readily available footwear that has not been modified and has no intended therapeutic functions. Pre-fabricated medical grade footwear: Pre-fabricated footwear that meets the specific needs of a person, on the basis of footwear that provides extra depth, multiple width fittings and features designed to accommodate a broader range of foot types. Other features may include modified soles, fastenings and smooth internal linings. The last shape defines the footwear shape including the outsole shape, heel pitch and toe spring. For off-the-shelf or pre-fabricated footwear generically generated lasts in different sizes are used. Socks: Garment for the foot and lower part of the leg, typically knitted from wool, cotton, or nylon. Stockings: Garment that fits closely over the foot and lower leg, typically elastic. Structured education: Any educational modality that is provided in a structured way. This can take many forms, such as one-to-one verbal education, motivational interviewing, educational group sessions, video education, booklets, software, quizzes, and pictorial education via animated drawing or descriptive images. Toe orthosis: an in-shoe orthosis to achieve some alteration in the function of the toe. Weight-bearing activity: Activity during which the foot is loaded by supporting the body weight of the person, and expressed as quantitatively as possible. Diabetes-related lower-extremity complications are a leading cause of the global burden of disability. Prevention of foot ulcers in the at-risk patient with diabetes: a systematic review. Prevention of foot ulcers in the at-risk patient with diabetes: a systematic review (update). Prevention of modifiable risk factors for foot ulceration in people with diabetes: a systematic review. The Ipswich Touch Test: a simple and novel method to identify inpatients with diabetes at risk of foot ulceration. The Ipswich Touch Test: a simple and novel method to screen patients with diabetes at home for increased risk of foot ulceration. The influence of external precipitating factors and peripheral neuropathy on the development and outcome of diabetic foot ulcers. Causal pathways for incident lowerextremity ulcers in patients with diabetes from two settings. Perceptions and experiences of diabetic foot ulceration and foot care in people with diabetes: A qualitative meta-synthesis. Impact of chronic kidney disease on survival after amputation in individuals with diabetes. The association of chronic kidney disease and dialysis treatment with foot ulceration and major amputation. Temporal association between the incidence of foot ulceration and the start of dialysis in diabetes mellitus. Biomechanical characteristics of peripheral diabetic neuropathy: A systematic review and meta-analysis of findings from the gait cycle, muscle activity and dynamic barefoot plantar pressure. Independent factors associated with wearing different types of outdoor footwear in a representative inpatient population: a cross-sectional study. Adherence to wearing prescription custom-made footwear in patients with diabetes at high risk for plantar foot ulceration. Reduction in foot ulcer incidence: relation to compliance with a prophylactic foot care program. Amputation prevention initiative in South India: positive impact of foot care education. Patients With Diabetic Foot Disease Fear Major Lower-Extremity Amputation More Than Death. Preventing diabetic foot ulcer recurrence in high-risk patients: use of temperature monitoring as a self-assessment tool. Skin temperature monitoring reduces the risk for diabetic foot ulceration in high-risk patients. A pilot study testing the feasibility of skin temperature monitoring to reduce recurrent foot ulcers in patients with diabetes-a randomized controlled trial. Diagnostic values for skin temperature assessment to detect diabetes-related foot complications. Custom-made orthesis and shoes in a structured follow-up program reduces the incidence of neuropathic ulcers in high-risk diabetic foot patients. Effectiveness and safety of using Podikon digital silicone padding in the primary prevention of neuropathic lesions in the forefoot of diabetic patients. Offloading effect of therapeutic footwear in patients with diabetic neuropathy at high risk for plantar foot ulceration.
Purchase microzide from india
Officials report that direct supervision facilities in San Francisco County have one-eighth the number of incident reports in comparison to linear facilities pulse pressure ati order microzide 12.5mg on line. Research conducted over a four month period in 2005 documented a significant decrease in the number of inmate-to-inmate and inmate-to-staff aggressive incidents in the direct supervision jails. These results were especially impressive because the direct supervision pod housed new arrivals, many of whom were detoxifying from substances, and who were adjusting to the new jail environment. Three of the five jails in Orange County were designed as direct supervision facilities. The same architect was employed to design each new facility, and subsequent designs were modified and enhanced based upon the experience of staff. Staff and administrators review all grievances and Administrators reported a dramatic shift in the attitudes disciplinary reports, a practices that administrators believe communicates of correctional officers from fair and equitable treatment to inmates that they will be treated fairly and regarding inmates as equitably. Additionally, joint rounds by security, inmate affairs, medical and problems to treating them mental health staff are conducted for special management inmates, and with respect. During interviews, management in a podular indirect supervision facility over a two-year period administrators reported that beginning in 2001. Correctional officers were trained and supported in those who stayed found direct adjusting to supervision inside the pods and in taking an active role in inmate supervision to make a supervision. Administrators reported a dramatic shift in the attitudes of dramatic effect, with increased communication and decreased correctional officers from regarding inmates as problems to treating them job-related stress. Not every staff person could make the adjustment to direct 41 supervision, and those who could not make the transition were either Mecosta County Jail staff made reassigned or discharged. During interviews, administrators reported that a commitment to jail those who stayed found direct supervision to make a dramatic effect, with cleanliness since a wellincreased communication and decreased job-related stress. Agency administrators made a significant commitment of training and resource development in Inmate Behavior Management principles developed by the National Institute of Corrections. Policies, procedures and rules were revised and there was a renewed emphasis on management not control. Like many of the other facilities visited during this study, Mecosta County Jail staff made a commitment to jail cleanliness since a well-maintained physical plant communicates that officials are in control and value orderliness. Detention Center was constructed as a podular, indirect supervision jail, but it operates with direct supervision principles. But officials and staff report that the use of direct supervision principles facilitates more efficient, effective and humane operations. Staff are expected to be in the housing pods at all times, and administrators are frequently there also to provide oversight and support. Staff are expected to prevent negative behavior before it occurs, and they are evaluated on their ability to supervise inmates effectively. Become familiar with group and individual inmate behavior patterns and identify changes that could signal a problem. It is neither a custodial strategy nor a treatment program, but rather a system of custody in which security and treatment staff work collaboratively to establish a safe, correctional environment, and to provide the necessary programs and services to inmates to promote sound adjustment and effective reintegration (Johnson, 1996). Unit management is the operational structure that encourages the personal interaction between staff and inmates. Unit management provides a flexible approach to classification and the management of diverse groups of offenders with different need. The objective is to ensure that inmate behavior does not deteriorate because officers are not holding inmates accountable and are not consistently addressing inmate concerns. The Arapahoe County Jail is a podular, indirect architecture facility, but administrators use smaller, more manageable pods as part of its supervision strategy. Each of the six pods is designed to hold a maximum of 32 inmates in each dayroom, and certain pods are self-contained environments. Pod 6, for example, holds a lockdown disciplinary unit and is comprised of one dayroom surrounded by a single pod. Four staff are assigned to each of these pods, including three deputies and one civilian Detention Operation Technician. Pods 2 and 5 hold minimum security inmates (work release, jail industries and jail trustees), and Pod 5 also holds a stand-alone facility for juvenile offenders, with its own staff and intake entrance. The purpose of this arrangement is creating small units designed for maximum supervision and manageability. Shelby County Jail officials implemented unit management as part of its direct supervision management philosophy. In this way, the jail was broken down into more manageable units and authority was delegated to a multi-disciplinary team in charge of each housing unit. Unit managers were given both the responsibility to independently manage their unit and the authority and support necessary to do so. The direct supervision philosophy was central to the process and there was an emphasis on staff having strong communication skills and recognizing early signs of trouble. Specialized units were created such as a gang intelligence unit and a disturbance response team. Because gangs can be a destabilizing factor in jails, there was a particular emphasis placed on conducting interviews and intelligence to identify and monitor gang members and their activities. The disturbance response team was responsible for regularly checking in with staff, conducting random searches and inmate escorts. Though some of the institutions were older architecture, the facilities by design and practice were created to be small, self-contained environments. Units were designed with staff and programming to match the particular level that a resident had achieved based on their time and success within the program. In this manner, each of the juvenile correctional institutions created a humanistic and individualized therapeutic environment designed to maximize the likelihood that residents would be successful upon release. In summary, direct supervision architecture and direct supervision inmate management philosophy were key ingredients in most of the facilities that were the subject of this study. Nearly every correctional agency was fundamentally transformed when they implemented direct supervision principles. Table 5 outlines a comparison of direct supervision management among selected jail study sites. Description of direct supervision management San Francisco Orange County Corrections Mecosta Shelby Patrick J. Programs and services to (a) productively occupy the time of inmates, (b) meet the needs of prisoners and juveniles, and (c) improve the life outcomes of those who are incarcerated the correctional professionals interviewed for this study discussed the need for high quality institutional programs and services to meet the needs of offenders and to assist in their successful transition to the community. Programs and services play a vital role in enhancing facility safety by gainfully occupying residents during incarceration. Idleness and boredom eventually result in serious behavior problems and destabilize the correctional environment. Well-implemented programs and supervised work opportunities contribute to institutional safety while also preparing individuals for success upon release. Description of programs and services across facilities San Francisco Orange County Corrections Mecosta Shelby Patrick J. Additionally, administrators prioritized a jail environment that is quiet, clean and sanitary, with sufficient light and air flow. That is, any type of disorder, including any signs of disrepair in the physical environment such as dirt, scuff marks, or peeling paint, sends a message about carelessness and disrespect. In the Mecosta County jail, then, there is a priority on ensuring unit cleanliness so inmates spend time productively keeping their rooms and the entire facility clean. Detention Center administrators focus on its health care program as one effort to keep the facility safe. Close working relationships have been established between the healthcare providers and security staff in the facility. Nurses act as patient advocates, so if an inmate does not show up when prescribed medications are distributed, nurses talk to the inmate to determine the reason and to help manage medication refusals. Additionally, all new detainees are provided an orientation on how to access medical services how to report sexual abuse. Officials promote an agency-wide emphasis on safety and reporting by emphasizing that all staff and inmates have a role in creating and ensuring safety in the facility. Woodfield has implemented a formal de-escalation program for use with residents which structures the method used to intervene with youth who are experiencing problems. Toward this goal, Woodfield solicits family support, visits and providing inmate other contact.
Cheap microzide line
Her pregnancy has been complicated by infectious etiology for her symptoms a bicuspid aorta with moderate aortic stenosis blood pressure kid buy cheapest microzide. A 32-year-old woman comes to your clinic for preconception She has had no symptoms of heart failure or arrhythmia during counseling. What is the best management plan to minimize currently taking phenytoin and carbamazepine. Start ampicillin for endocarditis prophylaxis crease the risks for the upcoming pregnancyfi Stop all seizure medications plan for an assisted vaginal delivery with forceps or vacuum b. Optimize her seizure regimen to include only one medication once the fetus is 12 station c. Keep the same dose of both medications and start taking diac stress 4 mg of folic acid d. To maintain cardiac output give lasix to decrease afterload and start taking valproic acid for monotherapy 32. A 35-year-old G4P0030 presents to the offce for her initial pretational age who has had limited prenatal care. She is 8 weeks pregnant, dated by her last normal complaints of abdominal pain, cold sweats, anxiety, and insomnia. Her obstetric history is signifcant for an elecUpon review of her history, she tells you that she usually has two tive termination of pregnancy as a teenager and two losses at to three vodka drinks every day. Low fetal birth weight sized, normal-appearing placenta with membranes intact and a. Her fundus is noted to be Her pregnancy is complicated by tobacco use and she is currently above the umbilicus and boggy despite fundal massage. A 27-year-old Caucasian G1P01001 is seen in the hospital on postpartum day number 2, after a spontaneous vaginal delivery of a 34. She presents with 6 months of pelvic discomfort, increasing abdomiis tolerating a regular diet, breast-feeding without diffculty, voidnal girth, and early satiety. Physical examination reveals a large ing spontaneously without discomfort, and having minimal lochia. Her pregnancy was complicated solely by In your discussion with the patient you predict that this most likely her rubella nonimmune status. She asks about the priby a superfcial vaginal laceration that was repaired in standard mary method of treatment for ovarian carcinoma. Surgery followed by radiation therapy regular heart rate and rhythm, clear lungs, a soft abdomen with a. Chemoradiation alone frm, though mildly tender, uterus, and nontender symmetric lower 35. A 20-year-old African American G2P2 is seen in the hospital on extremities signifcant for 21 pitting edema. Which of the followpostpartum day number 1, after a spontaneous vaginal delivery ing is the most likely cause of her postpartum feverfi Urinary tract infection a second degree perineal laceration that was repaired in standard c. This morning she appears very tired and although do2 days gestation arrives on labor and delivery and precipitously ing well from a physical standpoint, is noted to be bottle-feeding delivers a viable male infant followed by a large gush of fuid. She subsequently delivered a normal-sized, normalfollowing describes one of the benefts of bottle-feeding over appearing placenta with a centrally inserted three-vessel cord breast-feedingfi She decreases her risk of vertical transmission of Hepatitis C Her pregnancy was complicated by A1 gestational diabetes, by bottle-feeding which was suboptimally controlled. She will be unable to breast-feed because of her history of cant for a 2 3 3 cm intramural fbroid noted in the anterior wall breast augmentation during routine pregnancy ultrasound. Breast-feeding is contraindicated in women receiving Depoof asthma or hypertension. Bottle-feeding ensures a more adequate supply of milk to her Review of her previous pregnancy ultrasounds is signifcant for a baby during the frst few days of life low-lying placenta without previa. Breast-feeding may not provide enough Vitamin D for some conducted postpartum she is noted to have continued brisk infants compared with that supplemented in formula bleeding from her vagina. A 34-year-old Caucasian G3P2002 presents to labor and delivery tor for her postpartum hemorrhagefi A 22-year-old G2P1001 at 39 weeks 2 days presents with history smooth and light-bluish in color with the appearance of a bubble of contractions every 3 minutes for the past 2 hours. Her prior under the epithelial surface and a blood vessel running over the pregnancy was induced at 41 weeks and 3 days. A 68-year-old woman presents with vulvar pruritus since the repeat her cervical examination in 2 hours to assess if she is in previous year that has been increasing over the last few months. Two hours later you evaluate the patient and see that she She has tried antifungal medications, which seem to help, but the is painfully contracting and requesting epidural placement. You admit the patient to labor and delivery for use any douching products and is not taking any antibiotics. On expectant management and she receives an epidural for pain physical examination, you note thin white epithelium of the labia control. Which of the following fndings will cause you to recomminora with red oval-shaped erosions, varying in size from 0. A healthy 28-year-old G1 P0 comes to you for established prenaassessment of vulvar pruritus. This pregnancy was desired but has been treated with oral and topical antifungal creams. An early ultrasound for dating shows that the embryo She has adhered to vulvar skin care guidance. This diagnosis is new to vulvar biopsy that described squamous cell hyperplasia withher and she is concerned about the implications for her pregout evidence of a fungal infection. Antepartum bleeding epithelium of the inner labia majora and labia minora, with c. Recurrent frst trimester miscarriage several small red erosions suggestive of excoriation. Prolonged course of antifungals tempt at conception in the next month or two but she wants. There are no signs of adenomyosis and the and that she has had similar pain for several days, approximately endometrial stripe and ovaries are all normal. She has no vomiting or of mild dysmenorrhea but no history of menorrhagia, menodiarrhea with the pain, but she is constipated frequently, having metrorrhagia, postcoital spotting, or intermenstrual bleeding. What treatment jeans are getting tighter around the waist, although she remains options would you recommend to her for management of her active, playing soccer daily. Uterine artery embolization refuses a pelvic examination, but agrees to a visualization of the. A 48-year-old G3 P3 patient comes to see you for a complaint history reveals a history of infection with chlamydia 2 years ago. She has always had regular menstrual periods until denies any abnormal pap smears. She is also experiencing increased pain with her menis afebrile with stable vital signs. This was a desired pregnancy and she and her partner had a few episodes of intermenstrual bleeding. What counseling ultrasound reveals a normal myometrium with an endometrial should you give her regarding her future riskfi Her history of chlamydia makes it unlikely that she will dometrium without evidence of glandular crowding or cytologic ever conceive normally and she should consider in vitro atypia. She should receive a single dose of methotrexate to ensure that all of the pregnancy tissue has been evacuated 47. A new female patient presents to your offce on referral from her primary care physician. A 32-year-old G3P1021 woman returns to your clinic for a followpausal for more than 10 years, and has occasional right lower up visit. She has been using a combination oral 4-cm complex ovarian mass with cystic and solid components, contraceptive in a continuous fashion to manage her cyclic pelvic two internal nodules, septations, and increased Doppler fow.
Buy microzide master card
However blood pressure yogurt order microzide 12.5mg without prescription, psychiatric disorder may be less common than for individuals who do not have Down syndrome but who have a similar level of intellectual functioning (Cooper and Collacott 1994). Consider a mental health referral if symptoms of a possible psychiatric disorder appear to be developing. Endocrine Perform thyroid screening tests for hypothyroidism every two years until adolescence, and thereafter yearly. Immune-mediated hyperthyroidism also occurs more frequently (Pueschel et al 1998). There is an increased risk of other autoimmune disorders such as insulin-dependent diabetes mellitus (1. At 10 years refer to an optometrist to screen for refractive errors, keratoconus and cataracts. Personal hygiene and social skills Reinforce the importance of good self-care skills (grooming, dressing, and money handling skills). Discuss the development of age-appropriate social skills and the development of a sense of responsibility. Also discuss socialisation and family status and relationships, including financial arrangements and guardianship. Review the past history of health problems, questioning specifically about the possibility of obstructive airway disease and sleep apnoea. Nutrition and growth Continue to monitor for obesity, and provide advice about diet and exercise. Remember the ongoing requirement for endocarditis prophylaxis with dental care and certain other invasive procedures (Appendix 3). Continue to monitor for signs of sleep apnoea, especially if obesity is becoming a problem. Neurodevelopmental assessment A general physical and neurological examination should be performed, giving special consideration to the early diagnosis of atlanto-axial instability. An individual with significant communication deficits may be a candidate for an augmentative communication device. A gynaecological examination should only be performed if the young woman is sexually active. Anticipatory guidance Vision and hearing Review concerns about vision and strabismus at each visit. Presbyacusis, manifested by high-frequency hearing loss, may be evident by the second decade. Personal hygiene and social skills Reinforce the importance of good self-care skills (grooming and dressing). Discuss the development of age-appropriate social skills and the development of a sense of responsibility, for example money-handling skills. Discuss the appropriateness of school placement, with emphasis on adequate vocational training within the school curriculum. The family with an adolescent with Down syndrome may experience the usual conflicts as the adolescent tries to establish their own identity, find some private space and pursue their 24 the Clinical Assessment and Management of Children, Young People and Adults with Down Syndrome own interests. Teenagers with Down syndrome are subject to the same tempers, desires and emotions as anyone else, although they are often more frustrated in their experience. They are less able to resolve or manage the conceptual reasoning required at this age. Written information and videos are available from the local Down Syndrome Association (see Appendix 2 for resources. Discuss abuse prevention and talk about the recurrence risk to the patient and her family if she were to become pregnant. Currently, adult needs assessment services for individuals as adults begin at 16 years and the disability support services allowances and subsidies change. Sexual maturation and development in young people with Down syndrome Primary gonadal deficiency is common, progressive from birth to adolescence, and definitely present in adults. Females the average age of menarche of 13 years six months does not differ from a control group of girls without Down syndrome (Arnell et al 1996). Menses are usually normal and regular, and gonadotropin levels are similar to control groups. Most girls with Down syndrome can manage their own menstruation, either independently or with varying degrees of assistance (Epps et al 1990). Hormonal and surgical treatments should be required no more frequently than in the rest of the population. However, abnormal follicular development has been shown to be common among women with Down syndrome. Males In males primary and secondary sexual characteristics, genital size and hormonal levels are no different from a normative control group. Some men have difficulty attaining a full erection and ejaculation is not always possible. Although there have been several case reports in which a male has reproduced (a genetically normal child), males with Down syndrome are usually infertile (Zuhlke et al 1994). Contraception If contraception is required, the usual range of options is available to people with Down syndrome. Barrier methods, however, require a particularly careful process of education, and hormonal methods may need to be supervised. Reliable contraception may be the Clinical Assessment and Management of Children, 25 Young People and Adults with Down Syndrome important, but no more so than education on protective behaviours and appropriate sexual expression. Promoting healthy behaviour Promote education on smoking, and the use of drugs and alcohol. Transfer to adult care Facilitate transfer to adult specialist medical care, if this is appropriate or desired. At what age the transfer occurs should be based on the best interests of the young person. A referral letter from the paediatrician to appropriate adult specialists would help outline ongoing medical needs. Combined clinics are often helpful during the transition stage to help build trust and confidence in the new clinician. There may be concern that at one of the most vulnerable times in the life of the young person, he or she loses a known long-term support person. This issue needs managing carefully and with the interests and needs of the young the primary consideration. Discuss group homes, workshop settings, and other communitysupported employment. These discussions should also cover familial relationships, financial planning, and guardianship. General Most adults with Down syndrome enjoy good health, but their quality of life can be dramatically affected by chronic treatable conditions. Adults with Down syndrome may experience high levels of pain with comparatively little complaint and may localise pain poorly. In some cases, a change in behaviour may indicate an underlying medical condition causing chronic discomfort or pain. Behavioural disturbance may also indicate anxiety, sexual abuse, reaction to change, or the side effects of medication. People with Down syndrome will often comprehend more than is evident by their speech. Generally, adults with Down syndrome enjoy being addressed directly in an ageappropriate manner. The only legal authorities are the enduring power of attorney or the welfare guardian. The code sets out the options of what to do when neither of these are available (Bray 1999). Cardiorespiratory Untreated congenital cardiac anomalies will need ongoing monitoring. Mitral valve prolapse with or without tricuspid valve prolapse and aortic regurgitation may occur after 18 years of age, and predispose to infective endocarditis and cerebral emboli. Low blood pressure may lead to light-headedness and fainting, especially on rising in the morning.