
Zanaflex
Cheap zanaflex 2 mg online
Understand the natural history of cardiac abnormalities in the infant of a diabetic mother 5 spasms below rib cage buy zanaflex 2mg on line. Differentiate and manage the various causes of systemic hypertension in newborn infants 7. Recognize the fetal cardiac abnormalities in and plan follow-up for fetuses of mothers with connective tissue diseases, including systemic lupus erythematous E. Plan the evaluation and management of a newborn infant with transient myocardial ischemia 4. Plan the medical management of a newborn infant with persistent pulmonary hypertension, recognizing the systemic and pulmonary effects of vasoactive drugs 5. Understand the risk factors for development of persistent pulmonary hypertension in a newborn infant 6. Recognize the clinical features of an infant with persistent pulmonary hypertension and interpret diagnostic studies 7. Know the cardiovascular manifestations of maternal and fetal thyroid disease in a newborn infant F. Know how to recognize and manage hypoventilation in a child who is mechanically ventilated 5. Be familiar with airway support and mechanical ventilation strategies specific to patients with systolic and diastolic dysfunction B. Understand the principles of supply-demand balance (eg, concept of oxygen supply, oxygen reserve, extraction, oxygen consumption, perfusion requirements, relations between supply and demand) 2. Understand compensatory cardiovascular adaptive mechanisms (eg, autoregulation, local response, systemic responses) 4. Know the principles of monitoring and therapy for patients with low cardiac output, eg, principles and limitations of near-infrared spectrometry C. Understand the physiologic principles and management for the post-arrest patient D. Know the acute postoperative management for antiplatelet and anticoagulation therapy for artificial valves, systemic to pulmonary artery shunts, conduits and pulmonary patients at risk of pulmonary or systemic thromboembolism 2. Recognize and manage residual cardiac lesions after surgery may adversely affect a patients postoperative course 8. Know the indications for and limitations of various available diagnostic tools in evaluating a postoperative patient 9. Understand factors that influence systemic and pulmonary blood flow in a postoperative patient with an aortopulmonary shunt 10. Understand the role and limitations of mechanical cardiovascular support in the postoperative patient 14. Understand the mechanisms involved in the genesis of cardiac arrhythmias (eg, re-entry, automaticity, conduction block) 4. Understand the indications for acute and chronic medical management of tachy- and bradyarrhythmias 2. Know the mechanical methods (eg, vagal maneuvers; esophageal, external, intracardiac pacing; cardioversion) available for treatment of arrhythmias 3. Know the techniques for use of vagal maneuvers (including indications, contraindications, risks, and limitations) (eg, Valsalva, ice to face, carotid sinus massage) 2. Understand the factors associated with temporary pacing (eg, indications, contraindications, risks, and limitations) 2. Understand the basic technical aspects of the different modalities available for temporary pacing d. Understand the factors associated with cardioversion/defibrillation (eg, indications, contraindications, risks, and limitations) 2. Understand the factors associated with permanent pacing (eg, indications, contraindications, risks, and limitations) 3. Understand the factors associated with an implantable cardioverter-defibrillator (eg, indications, contraindications, risks, and limitations) 4. Understand the basic technical aspects for insertion of a permanent pacemaker or an implantable cardioverter-defibrillator 5. Understand the factors associated with biventricular resynchronization pacing (eg, indications, contraindications, risks, and limitations) B. Plan the evaluation and management of a patient with frequent atrial or ventricular ectopy C. Recognize and medically manage sinus tachycardia in patients of varying ages (eg, fetus, infant, child, adolescent, young adult) 2. Differentiate ectopic atrial tachycardia by surface electrocardiographic criteria 3. Recognize intracardiac electrophysiologic characteristics of ectopic atrial tachycardia b. Recognize and medically manage ectopic atrial tachycardia in patients of varying ages (eg, fetus, infant, child, adolescent, young adult) 2. Understand the factors associated with electrophysiologic study (eg, indications, contraindications, risks, and limitations) and catheter- or surgical- based ablation therapy for ectopic atrial tachycardia 3. Differentiate multifocal atrial tachycardia by surface electrocardiographic criteria 3. Recognize intracardiac electrophysiologic characteristics of multifocal atrial tachycardia b. Recognize and medically manage multifocal atrial tachycardia in patients of varying ages (eg, fetus, infant, child, adolescent, young adult) 2. Understand the factors associated with electrophysiologic study (eg, indications, contraindications, risks, and limitations) and catheter- or surgical- based ablation therapy for multifocal atrial tachycardia 3. Recognize and medically manage atrial flutter in patients of varying ages (eg, fetus, infant, child, adolescent, young adult) 2. Understand the factors associated with electrophysiologic study (eg, indications, contraindications, risks, and limitations) and catheter- or surgical- based ablation therapy for atrial flutter 3. Recognize intracardiac electrophysiologic characteristics of atrial fibrillation b. Recognize and medically manage atrial fibrillation in patients of varying ages (eg, fetus, infant, child, adolescent, young adult) 2. Understand the factors associated with electrophysiologic study (eg, indications, contraindications, risks, and limitations) and catheter- or surgical- based ablation therapy for atrial fibrillation 3. Differentiate junctional ectopic tachycardia by surface electrocardiographic criteria 3. Recognize intracardiac electrophysiologic characteristics of junctional ectopic tachycardia b. Understand the mechanisms and natural history of junctional ectopic tachycardia 2. Recognize and medically manage junctional ectopic tachycardia in patients of varying ages (eg, fetus, infant, child, adolescent, young adult) 2. Understand the factors associated with electrophysiologic study (eg, indications, contraindications, risks, and limitations) and catheter- or surgical- based ablation therapy for the congenital type of junctional ectopic tachycardia 3. Differentiate orthodromic reentry via accessory pathway by surface electrocardiographic criteria 3. Recognize intracardiac electrophysiologic characteristics of orthodromic reentry via accessory pathway b. Understand the mechanisms and natural history of orthodromic reentry via accessory pathway c. Recognize and medically manage orthodromic reentry via accessory pathway in patients of varying ages (eg, fetus, infant, child, adolescent, young adult) 2. Understand the factors associated with electrophysiologic study (eg, indications, contraindications, risks, and limitations) and catheter- or surgical- based ablation therapy for orthodromic reentry via accessory pathway 3. Recognize and manage the consequences of orthodromic reentry via accessory pathway 9. Recognize the clinical features of the permanent form of junctional reciprocating tachycardia 2. Differentiate the permanent form of junctional reciprocating tachycardia by surface electrocardiographic criteria 3. Recognize intracardiac electrophysiologic characteristics of the permanent form of junctional reciprocating tachycardia b. Understand the mechanisms and natural history of the permanent form of junctional reciprocating tachycardia c. Recognize and medically manage the permanent form of junctional reciprocating tachycardia in patients of varying ages (eg, fetus, infant, child, adolescent, young adult) 2.
Order zanaflex uk
Lacosamide is a novel anticonvulsant with a favorable phar- Frequently reported treatment-emergent adverse events are macokinetic profile including low protein binding spasms medicine order zanaflex overnight delivery, a long half- shown in Table 65. Acute and long-term effects of lacosamide in an animal model of status epilepticus. Lacosamide: an investigational drug for adjunctive treat- of 200 to 400 mg/day are likely to have optimum effect with ment of partial-onset seizures. Efficacy and safety of oral lacosamide as adjunc- tive therapy in adults with partial-onset seizures. Early onset of efficacy in the initial weeks of treatment Dizziness is the most common adverse event, followed by with lacosamide: a pooled analysis of three phase 2/3 trials. Lacosamide in painful diabetic peripheral neuropathy: a the availability of a parenteral formulation has the potential phase 2 double-blind placebo-controlled study. The cumulative spontaneous after observing its benefits in various types of intractable gen- remission rate over the first 12 months of seizures is about eralized seizures. Seizures are almost always intractable to treatment (2) reported control of seizures and an improvement in elec- with traditional anticonvulsant drugs. The ultimate prognosis is dismal for most dromes that have an age-related onset during a critical period patients and depends heavily on the cause of the spasms, pre- of brain development that can cause a characteristic regression existing neurologic and developmental status, the presence or or plateau of acquired developmental milestones at seizure absence of other seizures concomitant with the spasms, and onset and subsequent long-term cognitive impairment. William West wrote a letter to Lancet in which he a patient with preexisting mental retardation and a structurally described an unusual condition affecting his 4-month-old son, abnormal brain What is the optimal dosage of these drugs, James, as a peculiar form of infantile convulsions (14). Does the ultimate out- went on to describe a reduction in developmental trajectory in come depend on timing of treatment More than 160 years after this ical description of what we now know as infantile spasms. West, most of these questions In 1952, Gibbs and Gibbs described the classical interictal remain unanswered. These observa- tions support the theory that the developing brain experiences a Efficacy and Dosage significant stress response to various etiologies that results in this age-dependent epileptic encephalopathy. Spasms were controlled initially in Parameter for the medical treatment of infantile spasms has con- 65% of patients, but the relapse rate was high. Limiting its use is the characteristic concentric constric- however, Lombroso (12) showed a higher rate of normal cog- tion of visual fields. However, there is insufficient evidence mended for infantile spasms, can produce dangerous side of efficacy and safety to recommend any of these therapies at effects. The patient is glucose three times daily with Chemstix, and recognize spasms monitored in the outpatient clinic weekly for the first month so as to keep an accurate seizure calendar. Blood pres- erly trained parents report no seizures in a child whose waking sure is measured and an electrocardiogram performed. Over the next 6 weeks, the Recommended Protocols for Prednisone dose is gradually tapered. Usually, a response is seen within the first If prednisone is chosen because of its oral formulation and 7 days; if within 2 weeks no response is noted or a steroid lower incidence of serious side effects, the pretreatment labora- effect is evident, the lot is changed. Usually, the best result is temporary relief, effects of posterior pituitary and cortico-adrenal hormones in the epileptic because 70% to 90% of patients with multiple seizure types subject. Infantile spasms: outcome and prognostic (125), myoclonic astatic seizures begin between 7 months and factors of cryptogenic and symptomatic groups. Long-term cognitive outcomes of a cohort of children with cryptogenic infantile spasms treated with high-dose and Related Disorders adrenocorticotropic hormone. A long-term follow-up study of 214 children with the syn- nisone therapy in infantile spasms. Long-term outcome of West syndrome: a study of adults with short duration corticotropin therapy in infantile spasms. Arch directly on amygdala neurons to down-regulate corticotropin-releasing Dis Child. In vivo and in vitro effects of adrencorticotropic hormone infantile spasms: effects of hormonal therapy. Pathophysiology of massive infantile spasms: perspective on the spasms caused by corticotropin. Response of infantile spasms to infants given adrenocorticotropic hormone for infantile spasms. Long-term response to zonisamide in case of acquired aphasia and convulsive disorder. Effects of high-dose intravenous intractable infantile spasms: a multicentre, open-label, add-on trial. Moreover, the available anticonvulsant drugs neither influence Although multiple new agents have been introduced in the process of epileptogenesis in humans nor alter the underly- recent years, with attendant marketing considerations, many ing brain dysfunction that expresses itself as epilepsy. The identified drugs such as topiramate, it does not always recog- chapter has also been reorganized; drugs whose chemical nize potentially useful compounds, predict activity in humans, structure are related to pre-existing parent compounds are dis- or test antiepileptogenic potential (11). Newer models, such cussed first under the derivative compound section, followed as pilocarpine, kainate, or electrically induced post-status by a section devoted to compounds that are novel in their epilepsy models, are aimed at mimicking human disease and chemical structure. However, eslicarbazepine fied by the fact that seven of the compounds discussed in the acetates unique structure at the 10,11-position results in prior version of this chapter are no longer in development. Eslicarbazepine actetate undergoes In the fourth edition of this textbook, this chapter dis- biotransformation via presystemic first-pass hepatic hydrolysis cussed 11 anticonvulsant drugs (19). Oxcarbazepine and R-licarbazepine discussed in this chapter, are now covered in Chapters 64 and are minor active metabolites formed by non-cytochrome P450 65, respectively. Eslicarbazepine acetate displays linear phar- novel sodium- and calcium-channel blocker, structurally macokinetics. Peak plasma concentration Cmax occurs 2 to 3 hours multiple mouse and rat models suggesting broad-spectrum post dose. It has an elimination half-life of approximately 20 to anticonvulsant activity (15). In addition to its potential use as 24 hours, reaching steady state after 4 to 5 days (22). Eslicarbazepine acetate is not harmaline-induced tremor model of essential tremor, and pre- highly protein-bound (30%). In in vitro studies, it had no vented hyperalgesia in neuropathic pain models (16). Eslicarbazepine does not appear to significantly affect the plasma concentrations of R-warfarin. In preliminary stud- Levetiracetam Derivatives: Brivaracetam ies, serum concentrations of lamotrigine and topiramate were significantly reduced by b. Results from three recent multicenter, randomized, leads to anticonvulsant effect. Patients with refractory partial epilepsy were activity against secondarily generalized motor seizures in randomized to receive eslicarbazepine acetate (400, 800, or corneally kindled mice, and prevents clonic convulsions in 1200 mg depending on the study) or placebo for a 12-week audiogenic-susceptible mice (30). In addition, the responder rate Brivaracetam is rapidly absorbed following oral adminis- (defined as equal to or greater than 50% reduction in seizure tration, displays linear pharmacokinetics, binds weakly to frequency) was also higher in those patients treated with esli- plasma proteins, and has an approximately 8 hour half-life carbazepine acetate (800 mg: 36%, P 0. Hyponatremia (reported in 4/1050 patients) and demonstrated in vitro to have some impact on metabolizing rash (reported in 13/1050 patients) were rare. Brivaracetam has been shown to slightly reduce Another difference is that eslicabazepine acetate was effective carbamazepine concentrations, while slightly increasing levels when administered once per day in clinical trials. There is no ing a nontoxic valproate derivative, has shown the most change in exposure in elderly and renally impaired patients, promise of advancing in development. There is presently an absence of data from clin- shown to moderately reduce the estrogen and progesterone ical trials as they are yet to be performed.
Cheap zanaflex 2mg otc
Rev Stomatol Chir face the alternative between choosing absorba- Maxillofac Chir Orale 2016; 117: 96-100 spasms youtube order zanaflex overnight delivery. Clinical four-six months, or permanent, whose effects are performance of a dermal fller containing natural enduring but may cause serious damages. J Clin Aesthet fllers is always preferable since they do not cause Dermatol 2010; 3: 42-47. Combining super- edge of the chemical features of the substances fcial glycolic acid (alpha-hydroxy acid) peels with has to be provided by the physician. In this way, microdermabrasion to maximize treatment results the patient is informed of the potential side effects and patient satisfaction. Most of all, sive cosmetic procedures: prevention and man- the patient should have the possibility to choose agement. Delayed lipogran- uloma of the cheek following autologous fat injec- tion: report of 2 cases. Long-term complications as- Conflicts of interest sociated with permanent dermal fllers. Ethics and the facial plas- cular adverse events associated with facial tic surgeon. Eur Arch Otorhinolaryngol 2016; 273: soft tissue fillers: recognition, prevention, and 2323-2327. J Clin Aesthet problemi di legittimazione giuridica della chirur- Dermatol 2013; 6: 22-29. Ethics, Legal Issues, and consent for Silicone-induced granuloma after buttock aug- fllers. M arkedBradyycardiaorTotalI rreggularR hyythm 3secondm arks 6secondstrip R ate = Cardiac cyclein6secondstrip x10 R ate= Revision 1 Date: December 2013 Page 2 of 4 Adenosine (antiarrhythmic) Prescribing Protocol Caffeine and theophyllines antagonise the effects of adenosine; a higher Important Drug Interactions dose of adenosine may be required. Dipyridamole inhibits cellular uptake of adenosine, increasing the risk of bradycardia, so that the dose for stopping a tachycardia may be much less than usual. Stop dipyridamole 24 hours before planned use of adenosine or use lower initial dose of adenosine (a quarter to a half). Carbamazepine has been reported to increase the degree of heart block produced, so lower the initial dose of adenosine. Presentation 6 mg in 2 mL vial the patient should have cardiac monitoring throughout the procedure. A defibrillator and emergency resuscitation equipment must be available for Monitoring requirements immediate use. Induction of Atrioventricular Node Reentrant Tachycardia With Adenosine: Differential Effect of Adenosine on Fast and Slow Atrioventricular Node Pathways. No missed Notes beats Rhythm Regular or Irregular depending Rhythm Regular atrial and ventricular on conduction ratio Rate Atrial rate usually normal and ventricular rate 40-60 if Rate Atrial rate usually normal (60- junctional & 20-40 if 100) Ventricular rate slow (<60) ventricular P wave Normal4. A Steerable Cardiac Ablation Catheter Remote Control System is a prescription device that is external to the body and interacts with the manual handle of a steerable cardiac ablation catheter to remotely control the advancement, retraction, rotation, and deflection of a compatible, steerable ablation catheter used for the treatment of cardiac arrhythmias in the right side of the heart. The device allows reversion to manual control of the steerable cardiac ablation catheter without withdrawal of the catheter and interruption of the procedure. Do not use in patients who are contraindicated for cardiac catheterization procedures. Amigo is not to be used to manipulate a catheter except under visualization with fluoroscopy. Care should be taken not to advance the catheter against the side wall of the vessel or heart with excess force. Please refer to Figures 1 and 2 below, as well as the devices Instructions for Use and accompanying User Manual for additional details. As shown in Figure 1, the handle is placed in the corresponding docking station, which in turn is locked into the turret. The turret portion of Amigo provides rotational positioning / orientation of the catheter. The deflection driveshaft interfaces with the deflection knob located on the docking station to move the deflection lever. The remote control unit (Figure 2) is modeled after existing, commercially available catheter handles. The remote controller allows the physician to remotely maneuver the catheter position (insertion, withdrawal, rotation) and tip deflection (bend) from up to 100 feet away. The remote control unit is electronically linked via a 100 ft long extension cable to the catheter controller platform (docking station). The remote controller can only be operated when the infrared light beam (located on the controller body) is interrupted by being held and covered by the operators hand. The results from the animal study also evaluated the accuracy and function of all device electrical controls for proper tip placement within the chambers of the heart. The results from the animal study also evaluated the accuracy and function of all device mechanical controls for proper tip placement within the chambers of the heart. Of the three studies, one study was a 3-center study, while the other two were single-center studies. Evaluation of adverse events for safety, and acute procedural success was the primary effectiveness measurement in all three studies. Chronic success and procedural parameters (procedural time, total fluoroscopy time, operator fluoroscopy time) were the secondary effectiveness measurements. This training program was developed based on the training implemented, and operator performance observed, during the clinical studies mentioned above. In addition, the labeling also complies with special controls to include dedicated sections for a description of compatible catheters and a summary of tests used to evaluate compatibility (description of compatible catheters for each of the docking stations, device technical parameters, mechanical testing summary, in vivo studies summary. Non-clinical mechanical performance testing must demonstrate that the device performs as intended under anticipated conditions of use. The following performance testing must be performed: o Mechanical performance of the system (without catheter connected) o Mechanical performance of the system with compatible catheters connected to verify that the system does not impact catheter function or performance. Assessments must include the following: Side-by side remote control and manual comparisons of catheter manipulation (including all ranges of motion of catheter deflection and tip curl) for all compatible catheters; must include testing for worst-case conditions Evaluation of the accuracy and function of all device control safety features o Simulated-use testing in a bench anatomic model or animal model 2. The following performance testing must be performed: o Electrical performance of the system with compatible catheters connected to verify that the system does not impact catheter function or performance. In vivo Testing must demonstrate that the device performs as intended under anticipated conditions of use, including an assessment of the system impact on the functionality and performance of compatible catheters, and documentation of the adverse event profile associated with clinical use. Evidence must be submitted to address the following: o Manipulation and Positioning: Ability to manipulate compatible catheters to pre- specified cardiac locations and confirm proper anatomic placement and tissue contact; in accordance with the system indications for use and the compatible catheter indications for use. A training program must be included with sufficient educational elements that upon completion of the training program, the clinician and supporting staff can: o Identify the safe environments for device use o Use all safety features of device o Operate the device in simulated or actual use environments representative of indicated environments and use for the indication of compatible catheters. Performance data must demonstrate the sterility of the sterile disposable components of the system. Performance data must support shelf life by demonstrating continued sterility of the device (of the sterile disposable components), package integrity and device functionality over the requested shelf life. Labeling must include the following: o Appropriate instructions, warnings, cautions, limitations, and information related to the intended patient population, compatible ablation catheters, and the device safeguards for the safe use of the device. No serious device-related adverse events were reported in the clinical performance data for use of the device in the right atrium. Procedure-related adverse events (vascular access complications including both major and minor adverse events) were observed in 3. Based on this information, the risk associated with this device is considered acceptable. The probable benefits of the device are also based on data collected in clinical studies as described above. There is no conclusive data that has demonstrated that tactile feedback is critical for ablation success and avoiding complications. The favorable results from the clinical studies seem to suggest that tactile feedback is not critical in a right atrial ablation procedure.
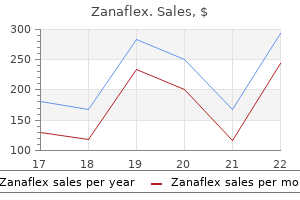
| Comparative prices of Zanaflex | ||
| # | Retailer | Average price |
| 1 | Staples | 606 |
| 2 | Defense Commissary Agy. | 266 |
| 3 | Wegman's Food Markets | 549 |
| 4 | Ingles Markets | 513 |
| 5 | Albertsons | 711 |
| 6 | OSI Restaurant Partners | 976 |
| 7 | Subway | 975 |
| 8 | Ahold USA / Royal Ahold | 834 |
| 9 | Toys "R" Us | 486 |
Purchase zanaflex 2mg mastercard
In a large prospective observational study spasms colon symptoms discount 4 mg zanaflex visa, 594 patients with vernal keratoconjunctivitis and atopic keratoconjunctivitis were included to Antihistamines with Mast Cell-stabilizing evaluate the effcacy of topical cyclosporine. In the United States, Ketotifen fumarate is available complete resolution of symptoms, and approximately 30% of steroid in a generic form and can be purchased over the counter with no users were able to discontinue concomitant topical steroid use. At least two weeks of therapy should be ophthalmic suspension, also appears safe and effective, and the 0. Compared to cyclosporine, Tacrolimus is controlled and symptoms to subside completely. It blocks cellular steroid receptors, inhibiting eye drops may include stinging and burning sensation. Refrigerating mediator release from mast cells and, thereby, suppressing T-cell the drops and/or use refrigerated artifcial tears prior to using these activation and consequent B-cell proliferation [51] Topical tacrolimus medications are effective ways to decrease burning sensation [42]. Oral antihistamines In cases of seasonal allergies, systemic over-the-counter, or Nonsteroidal Anti-infammatory Drugs prescription antihistamines may be helpful for symptoms of rhinitis Specifc prostaglandins are thought to lower the conjunctival and generalized pruritus. In cases of ocular symptoms, randomized threshold for histamine-induced itching, and the prostaglandins trials have shown that topical antihistamines are more effective than may be pruritogenic themselves as well. However, and decreased tear production in some patients, especially those with only ketorolac is indicated for the temporary relief of ocular itching concomitant dry eye [56]. Oral administration of antihistamines results in peak diclofenac have demonstrated efficacy in the treatment of vernal serum levels in 30 minutes to 3 hours, depending on the specifc drug. Thus, these agents have Glucocorticoids a slower onset of action compared with topical agents, unless they are taken prophylactically. Topical corticosteroid administration should be limited for use in patients with refractory symptoms such as symptoms associated Systemic immunomodulators with vernal keratoconjunctivitis and atopic keratoconjunctivitis. Patients with refractory severe disease or vision-threatening allergy Topical corticosteroids are not effective in the early phase allergic may beneft from systemic immunosuppressive therapy. Guidelines reaction; however by inhibiting the production and/or release of the regarding systemic immunosuppressive therapy are not available in the infammatory mediators they are very effective in suppressing the late- literature except for isolated case reports [59,60]. Loteprednol, has been approved in 1998 for medications have not been approved in Europe or the United States the treatment of allergic conjunctivitis. In a previous study it has been demonstrated that in severe cases Topical glucocorticoids should be used with caution in pregnant of ocular allergy, resistant to conventional therapy, systemic treatment women and under the supervision of both an ophthalmologist and an with T-lymphocyte signal transduction inhibitors may ameliorate obstetrician. Allergen immunotherapy is another option for severe both the dermatologic and ocular manifestations [60]. Allergic periocular dermatitis In another study, 4 patients (aged 31-64) with severe atopic If a contact allergy has been established as the cause of periocular keratoconjunctivitis and atopic dermatitis refractory to or dependent on dermatitis, the treatment of choice is to avoid the allergen. Ocular infammation was controlled involving topical therapies, emollients, treatment of infection if present, totally in three patients and partially in one patient [61]. In a 6 year old use of oral antihistamines for pruritus, and avoidance of triggering child with severe and vision threatening vernal keratoconjunctivitis, a factors. Symptoms of atopic dermatitis involving the periocular tissues dramatic improvement and stabilization of his symptoms was achieved may be treated with calcineurin inhibitors [74]. Numerous studies have demonstrated receives increasing doses of an allergen-containing extract, comprised their effcacy in atopic dermatitis [74]. Evidence-based confrmation of of the relevant allergens to which the patient is sensitive, in an attempt the safety of topical calcineurin inhibitors in the treatment of atopic to suppress or eliminate allergic symptomatology [63]. Allergen- dermatitis involving the face has been established in the literature [75]. Future Perspective Allergen specifc immunotherapy is believed to be the only therapeutic With increasing knowledge and advance in medicine engineering option capable of changing the natural course of allergic disease and technology, the future of many disorders including ocular allergy has demonstrated long-term, disease-modifying effects [66]. Given the pivotal role of IgE in the allergic cascade, antibodies directed against IgE or other Allergen specifc immunotherapy may be administered by either allergic mediators represent the future therapeutic approach to allergic the subcutaneous or sublingual route. A relatively new and promising drug that is being methods are effective at treating allergic conjunctivitis [67]. However, introduced into the ocular allergy clinical practice with encouraging in patients with polysensitization, the injection method shows superior results include the recombinant humanized monoclonal antibody results [68]. It has been recently suggested that dust mite gastrointestinal diseases and seasonal rhinoconjunctivitis [79,80]. In a randomized, double-blind placebo- Despite the lack of randomized clinical trials studying this drug in controlled study, authors demonstrated reduced nasal and ocular ocular allergy, few case reports showed omalizumab to be an effective symptoms in adults treated with a dust mite sublingual immunotherapy and promising drug in the in the treatment of severe ocular allergy tablet undergoing allergen challenge in an exposure chamber [71]. The lack of evidence based medicine on the use of these drugs in cases of ocular allergy, make it very diffcult to agree on guidelines Special Situations and recommendations for using these drugs. Clinical trial evaluating the Ocular allergy in pregnancy effcacy and safety are required. The frst step should include non-pharmacologic measures and Conclusion allergen avoidance. If such measures do not control symptoms Ocular allergy is a very common ocular infammatory disorder with adequately, cromolyn sodium eye drops may be tried next. Better understanding exposure is predictable (eg, pollen season), therapy should be initiated of the allergic mechanisms, infammation, and classifcation helps two weeks before [72]. Some forms of ocular allergy can be controlled following symptoms, antihistamine eye drops may be used. Volume 1, Issue 1 J Allergy Immunol 2017; 1:002 allergy are severe enough to require the collaboration of allergists and 23. Current medications for the treatment of nasal and ocular symptoms of allergy Opinion in Allergy & Clinical Immunology. Phlyctenular keratoconjunctivitis with special reference to the staphylococcal type. The central role of conjunctival mast cells in the pathogenesis of ocular allergy. Immunopathogenesis of ocular fever patients: symptom prevalence and severity and infuence on patient allergy: a schematic approach to different clinical entities. J Asthma of nonpharmacologic treatments for acute seasonal allergic conjunctivitis. Vernal keratoconjunctivitis revisited: a case series of 195 patients with Immunol. Am Prolonged effectiveness of bepotastine besilate ophthalmic solution for the J Ophthalmol. Long-term experience with sodium cromoglycate in the epitheliopathy associated with vernal keratoconjunctivitis. An Update on the of ophthalmic sodium cromoglycate and nedocromil sodium in the treatment Therapeutic Approach to Vernal Keratoconjunctivitis. Conjunctivitis of allergic origin: Clinical presentation and to an old story: novel concepts in the pathogenesis of allergic eye disease. Randomized controlled trial of ophthalmic solution in the treatment of severe allergic conjunctivitis. J ragweed allergy immunotherapy tablet in North American and European Ocul Pharmacol Ther. Comparison of ketotifen fumarate ophthalmic solution alone, desloratadine alone, and their combination for inhibition of the signs 73. Immunomodulation and safety of topical allergen challenge model: a double-masked, placebo- and active-controlled calcineurin inhibitors for the treatment of atopic dermatitis. A masked, crossover study of the ocular drying effects of two antihistamines, systematic review of the safety of topical therapies for atopic dermatitis. Br J topical epinastine and systemic loratadine, in adult volunteers with seasonal Dermatol. Effect of cetirizine in a conjunctival provocation treatment of seborrheic dermatitis: a review of pathophysiology, safety, and test with allergens. Use of pimecrolimus cream in disorders other than atopic effect of loratadine on specifc conjunctival provocation test. Severe vernal systemic T-lymphocyte signal transduction inhibitors in the treatment of keratoconjunctivitis successfully treated with subcutaneous omalizumab.
Generic 4 mg zanaflex otc
Tonic seizures: their significance ment-related activity in the human premotor cortex uterus spasms 38 weeks purchase zanaflex canada. Epilepsy and the Reticular E, Andermann F, Chauvel P, Engel J, Lopes da Silva F, Luders H, eds. New Generalized Seizures: From Clinical Phenomology to Underlying Systems York: Alan R Liss; 1987. Quantitative analysis of intracere- partial epilepsy: blinded multiple-observer analysis. Kozhevnikov-Rasmussen syndrome and the new mimicking pseudoseizures: some clinical differences. Progressive neuronal degener- data to that obtained with antero-temporal electrodes Focal status epilepticus and epilepsia partialis continua in scalp electrodes in the localization of epileptiform foci: a study of 26 adults and children. Neurologie epilepsy: seizure localization, cortical propagation and subcortical activa- Zentralblatt. Chapter 13: Focal Motor Seizures, Epilepsia Partialis Continua, and Supplementary Sensorimotor Seizures 183 167. Shuddering attacks in children: seizures: clinical and electroencephalographic findings. A Clinical-Electroencephalographic chogenic seizures: comparison of clinical and ictal characteristics. Sleep and seizures arising in the parasagittal and anterolaterodorsal frontal convexi- Epilepsy: the Clinical Spectrum. Autosomal dominant frontal tonic limb posturing in supplementary sensorimotor seizures. Immediate postictal features most commonly encountered seizures in both children and 4. Others defined as the simultaneous, symmetrical, and synchronous define this phase more broadly and include a variety of involvement of both cerebral hemispheres. These symptoms most likely reflect physiologic sisting of a tonic followed by a clonic phase. Examples of generalized epilepsy syndromes that sequently spreads to the limb girdles. All epilepsies related to circumscribed structural across the spasmodic glottis, producing the tonic epileptic brain lesions such as ischemic stroke, intracranial hemorrhage, cry that may last 2 to 12 seconds. The legs move into forced extension in the hip, diagnosis of a specific epilepsy syndrome. Preictal manifestations the clonic phase follows when the recurrent contractions 2. Ictal manifestations (with loss of consciousness) of the intermediate vibratory period become prolonged and a. Unilateral or activation of structures of the central autonomic network asymmetrical tonic limb posture (figure of four) likewise (insular cortex, amygdala, hypothalamus, periaqueductal gray lateralizes the seizure origin to the hemisphere contralateral to matter, parabrachial complex, nucleus of the tractus solitarius, the extended arm with a specificity of more than 90% (14). Head version is lead to alveolar hypoventilation causing decrease in blood described most frequently; it may occur to either site in differ- oxygen saturation and cyanosis (7). Regular, though often labored, respirations return, as the with focal semiological features. Here, the initial phase of the airway is partially blocked by orotracheal secretions and the seizure is characterized by staring and nonresponsiveness for closed jaw. At the onset of the convulsive result in aspiration if the reflexes protecting the airway are phase, the patient turns her head to the right, this is followed still suppressed. Tiredness, headache, and diffuse muscle sore- extension suggests seizure origin in the right hemisphere (21). Some patients are belligerent and combative Note also that there are a few clonic beats at the onset of the postictally. In a study of 120 secondarily decreasing frequency, similar to those observed in Video 14. This phenomenon is called secondary bilat- lowing syncope as well (28), therefore they cannot be used to eral synchrony. It may occur as a generalized interictal dis- differentiate between seizure and syncope. If the patient needs to be moved, this Ictal Findings should be done at the trunk to avoid joint luxations. In epilepsy monitoring units, simultaneously from the onset over the entire scalp. After about normal background activity, although rhythmic slowing in the 10 seconds, this rhythm is gradually replaced by a slower delta or theta range is more common in patients with idio- rhythm that increases in amplitude and decreases in frequency. During the postictal phase, epileptiform activity is an incidental finding in only about 1% this activity gradually increases in frequency until a normal of healthy humans; therefore, it is a highly specific marker for alpha rhythm returns. These phy revealed variations in the extent of synchrony preceding anticonvulsants may exacerbate seizures or induce status and during different types of seizures. Thus, they should not be used as initial monotherapy and in the latter, synchrony was higher locally than globally, in these patients. Frontal lobe seizures in particular may be bers were too small to reach statistical significance (45). A monotherapeutic anticonvulsant trial should be the initial One part addressed patients with generalized and unclassifi- approach in any patient presenting with epilepsy. In clinical practice, the physician three recent European studies as a monotherapy option in may have to choose an anticonvulsant even though description adults with new-onset epilepsy. In this situation, a broad spec- equally effective and time to discontinuation was equal for trum anticonvulsant should be used. Towards the seizure end, the frequency of the spike-and-wave complexes decreases to 2 Hz. Generalized spike-and-wave complexes are seen a few seconds later, less prominent compared to the seizure in Figure 14. Note that pages A and B are continuous, whereas 10-second epochs were omitted between pages (B and C) and (C and D). Asymmetric termination of secon- darily generalized tonic-clonic seizures in temporal lobe epilepsy. Unique clinical phenomenology can help distinguish primary from secondary generalized seizures in children. Lateralizing signs during seizures in focal evaluating the newer anticonvulsants results were stratified epilepsy. The generalized tonic-clonic seizure Since many patients require life-long therapy, an individual in partial versus generalized epilepsy: semiologic differences. Focal features in patients with idio- interactions with other drugs, potential long-term side effects pathic generalized epilepsy. Focal semiologic and electroen- cephalographic features in patients with juvenile myoclonic epilepsy. Complete seizure cessation with the use of anticon- sive head and eye movements during epileptic seizures. Those who continue to experience disabling limb posturing observed in secondarily generalized tonic-clonic seizures. Natural history of lactic acido- sis after grand-mal seizures: a model for the study of an anion-gap acidosis not associated with hyperkalemia. Serum prolactin concentrations are feature asymmetry and asynchrony, both in their clinical and elevated after syncope. Incidence and prognostic significance of epileptiform monotherapy of an appropriate anticonvulsant. Local versus distant phase synchronization in gen- Epileptic Seizures: Pathophysiology and Clinical Semiology. Ictal hypoxemia in localization-related new antiepileptic drugs, I: treatment of new-onset epilepsy: report of the epilepsy: analysis of incidence, severity and risk factors. Worsening of seizures by oxcarbazepine topiramate for treatment of partial epilepsy: an unblinded randomised con- in juvenile idiopathic generalized epilepsies.
Discount zanaflex 4mg free shipping
Defne ways to deliver consistent operational excellence in the use of injectables 2 spasms on left side of abdomen generic 2 mg zanaflex overnight delivery. Have a process to improve the quality of outcomes and fne tune results if necessary 4. Have a process to manage scheduling and recalls for follow up injection treatments 5. These documents are offered as a starting point for practitioners to develop their own specifc program of policies, procedures, documents, and templates for the safe use of injectables. Each of the components of this initiative must be customized for your particular practice. It is recommended that you confrm that there are not any specifc regulations regarding restrictions on vial splitting of single use vials or off-label use of injectables in the state where you practice. Additionally, it is important to verify that subordinate injectors are working within the scope of their particular state practice licensing act. These items serve as a starting point for the development of policies and procedures regarding injectables. It is important that you have your own specifc set of policies and procedures regarding injectables, as this will document that you have a specifc process for their use according to labeling and off-label use regarding administration in other anatomic areas, vial splitting procedures, and administration beyond the manufacturers time limit. Take a few minutes to write policies and procedures for your offce/clinic, based on the material in this section that will cover the following topics. Offce Policy Regarding Personnel Having Access to Injectables Administrative Staff, Medical Offce Assistant > May order product, receive and unpack shipments, and enter product into inventory Registered Nurses, Physician Assistant (Subordinate Injectors) > May order product, receive and unpack shipments and enter product into inventory. Can reconstitute injectables according to established offce policy and procedures with sterile technique > Can draw up injectables and prepare syringes for injection, according to offce policy and procedures with sterile technique > Can draw up injectables and prepare syringes for injection, according to offce policy and procedures with sterile technique > Can administer injectables as a subordinate injector under the direct supervision of physician employer, according to offce policy and procedures and the scope of their professional license. Use of approved vendors and legitimate distribution channels to obtain approved injectables and devices a. Avoidance of illicit product, reimportation, non-approved distribution channels b. Documentation of receipt of shipment in good quality What is needed here: Forms: Order/Receipt Receiving, Storage, and Inventory of Injectables 1. Segregation of injectables in labeled storage containers/areas to avoid mistakes in usage b. Have an established policy for specifc injectables that require reconstitution regarding concentration of reconstituted product according to X units per cc of injectable, i. If different brands of neurotoxins are being used in the same clinical situation, consider printing the quick reference cards on different colors of paper to prevent mistakes). Identify product, remove from packaging, verify lot # and expiration date of un-reconstituted product. Do not reconstitute two different brands of neurotoxins simultaneously in order to avoid mistakes 5. Reconstitute injectable according to offce policy regarding sterile technique and planned concentration of reconstituted product 7. Complete log form to document: lot # reconstitution date, concentration, expiration date 10. Utilize injectable product according to labeling or off-label, discard unused/expired product and vial as medical waste What is needed here: Quick Reference Tables For Reconstitution of Specifc Brand Neurotoxin, Neurotoxin Reconstitution Form Resources for supplies: a. On label: Administer neurotoxin in a specifc anatomic area, according to labeling. Use neurotoxin vial labeled for single patient use use within X time period, with wastage of unused product according to labeling. If the vial is labeled as a multi-use vial, it may be used in this manner, with appropriate infection control precautions. Off-label use: Administer neurotoxin for an indication not in the approved labeling. Use neurotoxin vial labeled for single patient use use within X time period for multiple patients (splitting of vial contents) and beyond labeled time for use. Alternative Procedure 1 - use vial as a multi-use vial, with multiple product withdrawals, each with a new needle/syringe b. Alternative Procedure 2 - split vial contents into sub-units, with storage in capped syringes that are appropriately labeled c. Alternative Procedure 3 - split vial contents into sub-units, with storage in sterile single-use sterile, non-pyrogenic parenteral medication wvials that are appropriately labeled Establishing an Expiration Date for Reconstituted Injectables 1. Ensure that reconstituted product will not be used beyond established expiration date and that unused product reaching expiration date will be discarded as medical waste Knowledge base regarding off-label use and storage: Peer-reviewed scientifc articles from medical literature give information regarding off-label storage reconstituted neurotoxins and use beyond labeled use within X hours and demonstrate that with proper sterile technique that microbial growth within the vial of reconstituted product does not occur. Reconstituted botulinum type a neurotoxin: clinical effcacy after long-term freezing before use. Lack of Microbial Contamination After Prolonged Storage of Partially Used Botulina Toxin A Preparations. After storage, all vials were cultured and tested negative for microbial contamination. Routine refrigerator storage of medication vials containing reconstituted botulinum toxin does not result in microbial contamination of the contents even after serial re-extraction of solution from these vials, and after handling of such vials by multiple personnel. Storage and subsequent reuse of botulinum toxin appears safe for at least 7 weeks after reconstitution. Multicenter, double-blind study of the effcacy of injections with botulinum toxin type a reconstituted up to six consecutive weeks before application. Cosmetic denervation of the muscles of facial expression with botulina toxin, a dose-response study. Toxin that was reconstituted 30 days produced the same loss of muscle tone as freshly mixed toxin. Reconstituted Botulina Toxin Type A Does Not Loose Potency In Humans If It is Refrozen or Refrigerated For Two Weeks Before Use. Reduced potency after refrigerated storage of botulitum toxin a: human extensor digitorum brevis muscle study movement disorders. Policy for On-label and Off-label Tissue Filler Use On label use tissue fller according to labeling regarding a specifc anatomic area. If physicians use a product for an indication not in the approved labeling, they have the responsibility to be well informed about the product, to base its use on frm scientifc rationale and on sound medical evidence, and to maintain records of the products use and effects. Physicians are not permitted to advertise off-label usage of drugs or devices, as the decision to use them for an indication not in the approved labeling is determined following the establishment of a physician-patient relationship and determination of a therapeutic plan. It is important to document in your medical record the decision to use drugs and devices off-label and to incorporate this into informed consent discussions. Be certain that issues of compliance with applicable regulations of promotion of drugs and devices are followed. Obtain medical history including stated interest in undergoing treatment with cosmetic or therapeutic injectable product a. Review contraindications including patients taking anticoagulants, anti platelet drugs (Plavix, aspirin, non steroidal anti infammatory) b. If this is a repeat injection, make assessment of effect and duration of earlier injection treatments, with adjustments/fne tuning as needed 4. Photographic documentation pre/post injection, including animated views if neurotoxin is being injected 5. Attach or enter label information to medical record, containing lot #, date of reconstitution, concentration, expiration date, b. Follow up call-quality assurance/patient satisfaction/schedule touch up injection if necessary 8. Emergency Situations that Involve injectables Occasionally, patients will experience physiologic responses to cosmetic injectables such as a vasovagal episode or tachycardia. While these are generally self-limiting, there is the need to manage these events in order that no harm come to your patient. Individuals who experience vasovagal episodes can be injured if they fall and strike the foor. Develop offce policies and procedures for situations of vasovagal episodes, tachycardia and similar events. Other types of events may be more uncommon such as lightheadedness or tachycardia that relates to local anesthetic injections containing epinephrine that may be used for nerve blocks or direct infltrations prior to fller injections and light-based procedures.
Purchase zanaflex 4mg amex
Recommendations for the Prevention muscle relaxant used in dentistry purchase zanaflex 4mg online, Detection and Management of Occupational Contact Dermatitis 2019 46 Best practices for hand hygiene emphasize that gloves do not replace the need for hand hygiene, yet failure to perform hand hygiene before donning (putting on) and after doffing (removing) gloves or 82 inappropriately performing hand hygiene while wearing gloves remains an ongoing issue. Overuse of gloves can be avoided by only using them when indicated by a risk assessment. In summary, when gloves are required, correct glove use, including appropriate selection, proper application and safe removal, is essential. Gloves should be intact and clean and dry inside; and hands must be clean and dry when donning gloves. Criteria for selection should be based on setting, likelihood of exposure to blood or body fluids, anticipated length of use, stress that will be 98 placed on the glove, penetration time of substances and need for optimal tactility. Allergy to natural rubber latex gloves is usually a type I, immediate hypersensitivity reaction that can range from mild skin erythema to anaphylaxis and even death. As a result, there has 101 been a move away from using latex gloves in favour of nonlatex gloves, whenever possible. Powdered latex gloves are particularly hazardous since the powder can transfer the latex allergen to the skin, 102 thereby enabling sensitization. Concurrent use of petroleum- or mineral-based skin care products can negatively affect 103 the integrity of latex gloves by causing significant deterioration. It has been suggested that wearing cotton glove liners under gloves helps to maintain skin barrier function. Cotton glove liners provided in health care settings are most commonly single use (disposable). Cotton glove liners that are classified as reusable should be changed between each use and reprocessed according to manufacturers instructions. Workers with more severe dermatitis should avoid wet work activities and may Recommendations for the Prevention, Detection and Management of Occupational Contact Dermatitis 2019 48 need temporary work accommodation (e. Recommendations for the Prevention, Detection and Management of Occupational Contact Dermatitis 2019 49 1. The role of personal protective equipment becomes less important when other more effective controls are available. Some measures to control exposures are more effective than others and the feasibility and applicability of each one depends on many factors. Multifaceted programs involving more than one exposure control measure are common in health care settings, making it difficult to determine the relative effectiveness of individual measures. Since occupational contact dermatitis results from direct contact of a substance with the surface of the skin, controlling exposure to the offending irritant or allergen is the most effective preventive measure. Elimination which physically removes the hazard, or substitution which replaces the hazard, are the preferred controls. Engineering controls, administrative controls and personal protective equipment also have important roles to play in primary prevention. Following hand hygiene best practices to keep the skin intact can also help to prevent occupational contact dermatitis. This is done by detecting and treating occupational contact dermatitis as soon as possible (to halt or slow its progress); encouraging personal strategies at work and home to prevent recurrence; and implementing programs to return people to their original health and function (to prevent long-term problems). Early diagnosis of occupational contact dermatitis is important for secondary prevention. It is important to confirm that the presenting skin disorder is dermatitis, to ascertain whether the dermatitis is work related, and to distinguish between irritant and allergic occupational contact dermatitis. Tertiary prevention aims to prevent impairment and disability in a worker who has developed occupational contact dermatitis by using medical management and appropriate workplace interventions, as well as prevention and control strategies, as appropriate, in the work and 14,106 home environments. Once diagnosed, contact dermatitis should be treated actively and quickly to prevent 107 development of chronic dermatitis. Specific treatment recommendations are out of scope for this document and are provided for information only. Treatment options for occupational contact dermatitis include topical, systemic and physical 108,109 therapies. The causes of occupational contact dermatitis are often multifactorial and treatment decisions should consider the type of occupational contact dermatitis. Despite decades of clinical practice using multiple medical therapies, there are very few randomized 107 controlled trials and little evidence to support specific interventions. Clinical management, including the use of oral and/or physical agents should be guided and monitored by experts with the appropriate knowledge and experience. The combined use of topical corticosteroids and emollients is the mainstay of first-line therapy for contact dermatitis. Alternative treatments for persistent dermatitis may include nonsteroidal anti-inflammatory ointments (e. When localized skin treatment fails, oral corticosteroids, such as prednisone, can be effective in the short term. Alitretinoin, an oral, vitamin A derivative, may be prescribed for severe occupational contact dermatitis. It has both immunomodulating and anti-inflammatory properties; however, it is teratogenic. Potent immunosuppressants, such as cyclosporine, methotrexate or mycophenolate mofetil, have also been used to treat severe occupational contact dermatitis; but, there is no evidence base to support their use and they can also be teratogenic. New products and therapies are always in development, as are new indications for treatment with existing medications and reporting of new adverse effects. It is important to remain prudent and ensure that treatment recommendations are current and consistent with guidance from recognized bodies of expertise. Legislation governing workplace interventions is provided in the Occupational Health 17,113- and Safety Act, as well as through provincial human rights and workers compensation legislation. These modifications can include reducing the number of hours of patient care 116 provided, changing the type of gloves used or changing skin care practices. This occurs when a job can no longer be adequately accommodated or modified for the health and safety of the individual. Workplace modifications, redeployment to a low-exposure area, or the introduction of exposure controls, may lead to improvement or resolution of occupational contact dermatitis in some workers, but these are not always effective solutions. Redeployment may become permanent if resolution of occupational contact dermatitis cannot be achieved. Poor prognosis can negatively impact health-related quality of life and result in prolonged sick leave and unemployment. Early identification of workers with occupational contact dermatitis who are at greater risk of poor outcomes could be useful in guiding risk management strategies and treatment options. Determining the role of various factors in clinical prognosis could help in early identification. Research in this area has investigated quality of life at baseline, severity of occupational contact dermatitis, age, gender, socioeconomic status, atopy and contact allergies as possible risk factors for poor prognosis. Semmelweis, affectionately referred to as the father of infection control, was a leader in infection prevention and control practices that remain essential today in reducing infection transmission risk and increasing patient safety. Normal skin is colonized by a collection of microorganisms that include bacteria, fungi and viruses. Microorganisms that reside on the skin are called resident flora or resident microbiota. Resident Recommendations for the Prevention, Detection and Management of Occupational Contact Dermatitis 2019 54 microbiota have a symbiotic function in humans, but they also can be opportunistic infectious agents if the barriers between microbiota and sterile sites are compromised (e. Transient flora (transient microbiota) are microorganisms that are not normally present on the skin of healthy individuals (e. Hand hygiene, aimed at removing transient flora and 121,122 reducing resident flora, can decrease the risk of transferring microorganisms to patients through direct contact during the delivery of care.
2mg zanaflex
Obstructed intercourse: Vaginal intercourse that is difficult findings can also be attributed to the complexity of human or not possible due to obstruction by genital prolapse or sexual function which is subject to a host of influences muscle relaxant 4211 v purchase 2mg zanaflex free shipping. Anorgasmia: Complaint of lack of orgasm; the persistent 7 arousal, and infrequent orgasm and dyspareunia. Vaginal dryness: Complaint of reduced vaginal lubrica- g nence at orgasm tion or lack of adequate moisture in the vagina. Hypertonic pelvic floor muscle: A general increase in nence at penetration (penile, manual, or sexual device) muscle tone that can be associated with either elevated 4. Vulvodynia: vulvar pain of at least 3 months duration, without clear identifiable cause, which may have 37 potential associated factors. Anodyspareunia: Complaint of pain or discomfort associ- before surgery) 28 ated with attempted or complete anal penetration. Anal laxity: Complaint of the feeling of a reduction in anal after surgery or other interventions tone. Abstinence due to pelvic organ prolapse: Non engagement - Vaginal narrowing: decreased vaginal calibre. Vaginal wind (Flatus): Passage of air from vagina (usually stiff vagina or a foreign body (stitches, mesh exposure, accompanied by sound). Obstructed intercourse: vaginal intercourse is difficult or j female reconstructive surgery. Motivations (here defined as reasons/incentives) discomfort associated with attempted or complete vaginal for attempting to become sexually aroused are scarce or 1,e penetration. Superficial (Introital) dyspareunia: Complaint of pain or normative lessening with lifecycle and relationship discomfort on vaginal entry or at the vaginal introitus. Vulvo-vaginal hypoesthesia: Reduced vulvo-vaginal sen- discoverable on examination of the patient: an objective sitivity to touch, pressure, vibration, or 1 4,34,35,n indication of disease or health problem. Vulvo-vaginal hyperaesthesia: Increased vulvo-vaginal view of the patient, and not all require intervention. The sensitivity to touch, pressure, vibration, or temperature genital examination is often informative and in women with 4. Pudendal neuralgia: elicited or described by the patient as sexual dysfunction can often be therapeutic. A focused burning vaginal and vulva pain (anywhere between the genital examination is highly recommended in presence of anus and the clitoris) with tenderness over the course of the 1,o dyspareunia, vaginismus, neurological disease, genital pudendal nerve. Muscle tone: In normally innervated skeletal muscle, tone is vaginal length, calibre and mobility, presence of scarring created by active (contractile) and passive (viscoelas- and/or pain and estrogenization, and whether or not there is tic) components clinically determined by resistance of the vaginal or labial agglutination. Normal pelvic floor muscles: Pelvic floor muscles which evaluated at it may influence sexual function by both can voluntarily and involuntarily contract and relax. If the patient has had an operation in which a which do not relax, or may even contract when relaxation synthetic mesh is utilized then mesh may be felt in the is functionally needed, for example, during micturition or vagina which may or may not be associated with 40 defecation. Underactive pelvic floor muscles: Pelvic floor muscles to make observations for any pelvic mass or unusual which cannot voluntarily contract when this is appropriate. Examination of the pelvic floor muscles may muscles where there is no voluntary action palpable. Pelvic floor muscle spasm or pelvic floor myalgia: dyspareunia, vaginismus, or history of pelvic trauma are defined as the presence of contracted, painful muscles on present, completing internal exams is difficult and may be palpation and elevated resting pressures by vaginal impossible. This persistent contraction of striated gentle, introital palpation, or performing a Q-tip touch test muscle cannot be released voluntarily. If the contraction of the introitus is recommended prior to any internal is painful, this is usually described as a cramp. Pelvic floor muscle tenderness: occurrence of the examination sensation of pain or painful discomfort of the pelvic floor muscles elicited through palpation. Hypertonicity: A general increase in muscle tone that can associated with increased size of genital hiatus. Deficient perineum/cloacal-like defect: A spectrum of 47,48,50 or passive stiffness in the muscle. As the cause is tissue loss from the perineal body and rectovaginal septum often unknown the terms neurogenic hypertonicity and with variable appearance. Hypotonicity: A general decrease in muscle tone that can just an extremely thin septum between the anorectum and 28 be associated with either reduced contractile activity and/ vagina. As the cause is often research setting, and many do not accurately reflect patient unknown the terms neurogenic hypotonicity and non- rating of improvement. Muscle strength: Force-generating capacity of a mus- use of sexual diaries or event logs, clinician-administered 48,51 cle. Muscle endurance: the ability to sustain near maximal or the evaluation of the efficacy of interventions. Personal interviews are time consuming and have wide variation in application making the 4. Pallor/erythema: Pale or erythematous genital mucosa and researchers feel that questionnaires are the most accurate 2. Loss of vaginal rugae: Vaginal rugae flush with the skin in measuring sexual function. Tissue fragility/fissures: Genital mucosa that is easily include measures which were developed to include concepts broken or damaged important to women with pelvic floor dysfunction and those 4. Vaginal petechiae: A petechia, plural petechiae, is a small that were developed to address sexual health in women (1-2 mm) red or purple spot on the skin, caused by a minor without pelvic floor dysfunction. In general, pelvic floor bleed (from broken capillary blood vessels) condition specific measures are more likely to be responsive 5. Urethral mucosal prolapse: Urethral epithelium turned to change than measures that are not condition specific, outside the lumen although both have been used in the evaluation of women 6. Loss of hymenal remnants: Absence of hymenal remnants with pelvic floor dysfunction. Vaginal dryness: Complaint of reduced vaginal lubrication a domain specific to sexual function. Increasingly, other measures, including those that evalu- ate body image, also impact sexual function and are associated with pelvic floor dysfunction. Identify chronic systemic diseases and their treatments (eg, Diabetes, Multiple Sclerosis, Depression, Hypertension, lichen sclerosis) which can be associated with sexual dysfunction. For women with neurological disease affecting the pelvic nerves clarify light touch, pressure, pain, temperature sensation, and vaginal tone, voluntary tightening of the 5. Pelvic Floor Condition specific sexual function measures: Sexual arousal results in increased blood flow allowing A validated sexual function measure which is developed to genital engorgement, protrusion of the clitoris and augmented include concepts relevant women with pelvic floor vaginal lubrication through secretion from the uterus and dysfunction. Generic sexual function measures: A validated measure vessels in the vaginal walls. Several instruments are available that was developed to evaluate sexual function but does not 65,66 to measure blood flow during sexual stimulation. Functional magnetic resonance imaging: Investigation of anatomical integrity of clitoral structures and the changes neural activation in anatomically localized cerebral in clitoral and labial diameter associated with sexual regions evaluated through monitoring subtle changes in 71 stimulation can be evaluated in B mode. Movement of regional cerebral blood flow that occur with activation of the blood relative to the transducer can be expressed as the neurons. These patterns of activation and deactivation 72 measurement of velocity, resistance, and pulsatility. Laser Doppler imaging of genital blood flow: An temperature, or vibration) using an ascending or descend- imager positioned close to the vulva allows the ing method in order to evaluate the detection threshold. This method has been used to assess vaginal sites including the clitoris, labia minora, and 84,87,88 response to sexual stimulation and correlated with majora as well as vaginal and anal margins. Reflex examination: Evaluating sacral arc integrity, the understanding of microvascular differences in women bulbocavernous reflex can be elicited by squeezing the with provoked vestibulodynia compared to asymptom- clitoris and assessing the contraction of the anal 76 89 atic controls. Magnetic resonance of imaging of the genito-pelvic pricking delivered to perianal skin and observing anal 89 area: Evaluation of the increase in clitoral structure sphincter contraction. Latencies can also be evaluated by volume related to tissue engorgement occurring during stimulating the nerve and evaluating muscle response 76 90 arousal. The electrode also monitors oxygen diffusion 78,79 bulbospongiosus and ischiocavernous are also involved in across the skin. Thermography or thermal imaging of the genital area: hypoesthesia, anorgasmia, and urinary incontinence during Evaluation of genital temperature using a camera detecting 9 97,98 intercourse while hypertonicity may lead to dyspareunia. Details central nervous system disorders (eg, diabetic neuropathy, about recommendations to ensure validity of pressure 99 spinal cord injury) may lead to anorgasmia and decreased measurements are provided elsewhere. Dynamometry measures force in Newton including decreased libido, lack of arousal, vaginal dryness, and (N).