
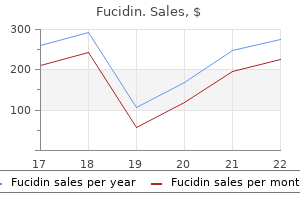
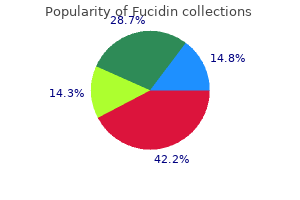
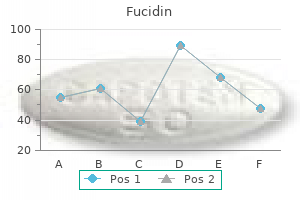
Fucidin
Cheap fucidin 10gm with mastercard
There are several discectomy systems on the market that are correctly considered percutaneous devices antibiotic resistance doxycycline fucidin 10 gm overnight delivery. However, the anatomy is not directly visualized and the process of removing the nuclear tissue is not visually monitored. Sometimes, a small diameter endoscope may be inserted through the lumen of the access cannula, but this is done at the end of the procedure, not while the tissue is being modified. Again, what makes these procedures percutaneous is not the diameter of the device per se, but the lack of direct visualization of internal structures during the operation. On the other hand, endoscopic spine surgery permits direct visualization of the anatomy while the surgeon uses miniature instruments to operate on the tissue. The spine endoscope is designed with a separate optic channel and instrument working channel so that visualization and surgery may occur simultaneously. The operative tips of the instruments emerge from the tip of the scope right next to , and in full view of, the objective lens and are kept in full view during surgery. Most of the percutaneous systems are designed only to be able to remove nucleus tissue from inside the disc. If there is other pathology (extruded fragments, sequestered fragments, annular tears, stenosis, adhesions, etc. For example, if a fragment of herniated nucleus becomes sequestered in the epidural space, the Wolf system contains a flexible tip probe and articulating rongeurs to retrieve it. Similarly, if during a discectomy the surgeon sees that the facet joint is also impinging on the nerve root, the Wolf system contains high-speed burrs and bone punches to permit removal of the impinging bone. As opposed to percutaneous systems that have a single purpose tool that blindly removes nucleus tissue, endoscopic systems, such as the Richard Wolf system, permit the user to visually inspect the anatomy and identify pathology, and utilize different instruments intended to specifically address these conditions. It is a hallmark of all open surgery that the surgeon is able to inspect the anatomy, identify pathology, make intraoperative decisions on how to address problems, and select the most appropriate instruments to address it. Conclusion: Full endoscopic discectomy is a safe and effective surgical alternative to microsurgical discectomy and should be covered, particularly due to the option for either an interlaminar or transforaminal approach as well as a wide array of instrumentation available to address lumbar disc herniation and numerous other pathologies. Full endoscopic lumber procedures allow direct visualization of internal structures while tissue is being modified - a hallmark of traditional surgical technique and should be covered by insurers. Full endoscopic discectomy should not be classified with or confused with percutaneous procedures from either a clinical perspective or a coverage and coding perspective. Literature Excerpt: Full-endoscopic interlaminar and transforaminal lumbar discectomy versus conventional microsurgical technique: A prospective, randomized, controlled study. Objective: Comparison of results of lumbar discectomies in full-endoscopic interlaminar and transforaminal technique with the conventional microsurgical technique. Summary of Background Data: Even with good results, conventional disc operations may result in subsequent damage due to trauma. Endoscopic techniques have become the standard in many areas because of the advantages they offer intraoperatively and after surgery. With the transforaminal and interlaminar techniques, 2 full-endoscopic procedures are available for lumbar disc operations. Methods: One hundred seventy-eight patients with full-endoscopic or microsurgical discectomy underwent follow-up for 2 years. Results: After surgery 82% of the patients no longer had leg pain, and 14% had occasional pain. The full-endoscopic techniques brought significant advantages in the following areas: back pain, rehabilitation, complications, and traumatization. The clinical results of the full-endoscopic technique are equal to those of the microsurgical technique. At the same time, there are advantages in the operation technique and reduced traumatization. With the surgical devices and the possibility of selecting an interlaminar or posterolateral to lateral transforaminal procedure, lumbar disc herniations outside and inside the spinal canal can be sufficiently removed using the full-endoscopic technique, when taking the appropriate criteria into account. Full-endoscopic surgery is a sufficient and safe supplementation and alternative to microsurgical procedures. Key Points: the clinical results of the full-endoscopic technique are equal to those of the microsurgical technique. At the same time, there are advantages in the operation technique and reduced traumatization, including:. Full-endoscopic surgery is a sufficient and safe supplement and alternative to microsurgical procedures. Open and maximally-invasive procedures are necessary in spinal surgery and must be mastered by surgeons so that they also overcome problems and complications encountered when performing full-endoscopic procedures. Nomenclature and classification of lumbar disc pathology: recommendations of the combined task forces of the North American Spine Society, American Society of Spine Radiology, and American Society of Neuroradiology. A prospective, randomized study comparing full-endoscopic interlaminar and transforaminal versus microsurgical revision. Apart from any use as permitted under the Copyright Act 1968, no part may be reproduced by any process without prior written permission from the Commonwealth. You may download, display, print and reproduce this material in unaltered form only (retaining this notice) for your personal, non-commercial use or use within your organisation. Apart from any use as permitted under the Copyright Act 1968, all other rights are reserved. This advice will help to inform government decisions about which medical services should attract funding under Medicare. There are a number of different non-fusion devices available but they all operate on the same biomechanical principle, that is to limit hyperextension of the vertebrae at the level where the implant is inserted and to unload the posterior elements. Non-fusion devices may be divided into two main groups?interspinous spacers and pedicle screw systems. Interspinous spacer devices are, as their name suggests, inserted between the spinous processes and have no rigid fixation to the vertebral pedicles. These devices are all essentially similar and it is the view of the Advisory Panel that data for one device can be reasonably extrapolated to the others. This device differs from the interspinous devices as it may provide more rigid stabilisation and requires a more extensive surgical procedure for its insertion. Although the Dynesys looks superficially similar to standard posterior fusion devices, the structures connecting the vertebral bodies to one another are flexible and are not intended to provide rigid stability. A rigorous assessment of the available evidence is thus the basis of decision making when funding is sought under Medicare. A team from Adelaide Health Technology Assessment, School of Population Health and Clinical Practice, at the University of Adelaide, were engaged to conduct a systematic review of the literature on lumbar non- fusion posterior stabilisation devices for the treatment of symptomatic lumbar spinal stenosis, degenerative spondylolisthesis, herniated disc and facet joint osteoarthritis (primarily with lumbar radicular compromise). Literature searches were conducted up until April 2006 from AustHealth, Cinahl, Cochrane Library, Current Contents, Embase, Pre-medline, ProceedingsFirst, Web of Science and EconLit. Studies that met pre-defined criteria were included to assess the safety and effectiveness of non-fusion devices. Since it is estimated that 71 per cent of patients receive decompression and/or fusion surgery in the private hospital system, it is estimated that another 4,937 patients would undergo these procedures in public hospitals. Therefore, the best estimate of the prevalence of degenerative disorders of the lumbar spine failing to respond to conservative management is estimated to be 16,680 per year. While this would include patients who receive comparative procedures for indications not suitable for non-fusion devices, there would also be a small number of patients who currently do not undergo surgery, but who might be considered for non- fusion stabilisation. Safety There were 11 studies that provided information on the safety of non-fusion devices. Major adverse events such as malpositioning of screws and pedicle fractures occurred in a median of 5 per cent of patients who received the Dynesys. Minor adverse events associated with the Dynesys included dural lesions and superficial wound infections. No studies were available to compare rates of screw loosening or breakage between the Dynesys pedicle screw system and pedicle screw systems associated with fusion surgery. Blood loss appeared to be related to the complexity and invasiveness of the procedure. One study found that the insertion of the Dynesys resulted in slightly more blood loss than a fusion procedure, but in this study 25 per cent more screws were inserted with the Dynesys than with fusion. Lumbar non-fusion posterior stabilisation devices ix Overall, the Dynesys appears to be safe, and was found to be as safe as decompression surgery alone or decompression surgery with fusion. The Dynesys device is the most invasive of the lumbar non-fusion posterior stabilisation devices because of the insertion of pedicle screws. It is therefore thought that generalising the results of the safety of the Dynesys to the other devises would not result in any underestimation of the safety concerns. Minor complications such as respiratory distress, wound swelling and pain occurred in up to 8 per cent of patients, and major complications such as malpositioned implants occurred in up to 3 per cent of patients. One death was reported that was potentially related to the surgery, caused by pulmonary oedema in a patient with a history of cardiovascular disease.
Buy fucidin in india
Be certain that you permanently discard any pages indicated for removal in the filing instructions in order to avoid confusion later antibiotics for dogs vs humans buy fucidin 10 gm on-line. To execute the filing instructions, simply remove and throw away the pages listed under Remove these Old Pages, and replace them in each case with the corresponding pages from this supplement listed under Add these New Pages. Occasionally new pages will be added without removal of any old material (reflecting new regulations), and occasionally old pages will be removed without addition of any new material (reflecting rescinded regulations)?in these cases the word None will appear in the appropriate column. By keeping and filing the Highlights sections, you will have a reference source explaining all substantive changes in the text of the regulations. Supplement frequency: this Book C (Schedule for Rating Disabilities) was originally supplemented four times a year, in February, May, August, and November. Beginning 1 August 1995, supplements will be issued every month during which a final rule addition or modification is made to the parts of Title 38 covered by this book. The effect of this action is to ensure that this portion of the rating schedule uses current medical terminology and to provide detailed and updated criteria for evaluation of gynecological conditions and disorders of the breast. The final rule incorporates medical advances that have occurred since the last review, updates current medical terminology, and provides clearer evaluation criteria. Examiners must use either Goldmann kinetic perimetry or automated perimetry using Humphrey Model 750, Octopus Model 101, or later versions of these perimetric devices with simulated kinetic Goldmann testing capability. The examiner must document the results for at least 16 meridians 221/2 degrees apart for each eye and indicate the Goldmann equivalent used. Determine the average concentric contraction of the visual field of each eye by measuring the remaining visual field (in degrees) at each of eight principal meridians 45 degrees apart, adding them, and dividing the sum by eight. To determine the evaluation for visual impairment when both decreased visual acuity and visual field defect are present in one or both eyes and are service connected, separately evaluate the visual acuity and visual field defect (expressed as a level of visual acuity), and combine them under the provisions of ?4. The examiner must use a Goldmann perimeter chart or the Tangent Screen method that identifies the four major quadrants (upward, downward, left, and right lateral) and the central field (20 degrees or less) (see Figure 2). The examiner must document the results of muscle function testing by identifying the quadrant(s) and range(s) of degrees in which diplopia exists. When a claimant has both diplopia and decreased visual acuity or visual field defect, assign a level of corrected visual acuity for the poorer eye (or the affected eye, if disability of only one eye is service- connected) that is: one step poorer than it would otherwise warrant if the evaluation for diplopia under diagnostic code 6090 is 20/70 or 20/100; two steps poorer if the evaluation under diagnostic code 6090 is 20/200 or 15/200; or three steps poorer if the evaluation under diagnostic code 6090 is 5/200. This adjusted level of corrected visual acuity, however, must not exceed a level of 5/200. Use the adjusted visual acuity for the poorer eye (or the affected eye, if disability of only one eye is service-connected), and the corrected visual acuity for the better eye (or visual acuity of 20/40 for the other eye, if only one eye is service-connected) to determine the percentage evaluation for visual impairment under diagnostic codes 6065 through 6066. Unless otherwise directed, evaluate diseases of the eye under the General Rating Formula for Diseases of the Eye. With documented incapacitating episodes requiring 7 or more treatment visits for an eye condition during the past 12 months. Note: this code includes orbital trauma, as well as penetrating or non-penetrating eye injury 6010 Tuberculosis of eye: Active. Minimum evaluation if continuous medication is required 10 6014 Malignant neoplasms of the eye, orbit, and adnexa (excluding skin): Malignant neoplasms of the eye, orbit, and adnexa (excluding skin) that require therapy that is comparable to those used for systemic malignancies, i. Any change in evaluation based upon that or any subsequent examination will be subject to the provisions of ?3. If there has been no local recurrence or metastasis, evaluate based on residuals Malignant neoplasms of the eye, orbit, and adnexa (excluding skin) that do not require therapy comparable to that for systemic malignancies: Separately evaluate visual and nonvisual impairment. If there is no replacement lens, evaluate based on aphakia (diagnostic code 6029) 6029 Aphakia or dislocation of crystalline lens: Evaluate based on visual impairment, and elevate the resulting level of visual impairment one step. Concentric contraction of visual field: 1 With remaining field of 5 degrees: Bilateral. Note 1: Natural menopause, primary amenorrhea, and pregnancy and childbirth are not disabilities for rating purposes. Chronic residuals of medical or surgical complications of pregnancy may be disabilities for rating purposes. Note 2: When evaluating any claim involving loss or loss of use of one or more creative organs or anatomical loss of one or both breasts, refer to ?3. Footnotes in the schedule indicate conditions which potentially establish entitlement to special monthly compensation; however, almost any condition in this section might, under certain circumstances, establish entitlement to special monthly compensation. General Rating Formula for Disease, Injury, or Adhesions of Female Reproductive Organs (diagnostic codes 7610 through 7615): Symptoms not controlled by continuous treatment. Conditions associated with pelvic organ prolapse include: uterine or vaginal vault prolapse, cystocele, urethrocele, rectocele, enterocele, or any combination thereof. Any change in evaluation based upon that or any subsequent examination shall be subject to the provisions of Sec. Rate chronic residuals to include scars, lymphedema, disfigurement, and/or other impairment of function under the appropriate diagnostic code(s) within the appropriate body system (No. Rate chronic residuals to include scars, lymphedema, disfigurement, and/or other impairment of function under the appropriate diagnostic code(s) within the appropriate body system. Rate chronic residuals according to impairment of function due to scars, lymphedema, or disfigurement (e. A-1 Appendix A to Part 4 ? Table of Amendments and Effective Dates Since 1946 Sec. A-5 6704 Subparagraph (1) following December 1, 1949; criterion March 11, 1969; criterion September 22, 1978. A-10 8914 Added October 1, 1961; criterion September 9, 1975; criterion March 10, 1976. Retinal dystrophy (including retinitis pigmentosa, wet or dry macular degeneration, early-onset macular degeneration, rod and/or cone dystrophy). Lungs and Pleura Tuberculosis Ratings for Pulmonary Tuberculosis (Chronic) Entitled on August 19, 1968: 6701. Ratings for Pulmonary Tuberculosis Initially Evaluated After August 19, 1968: 6730. Complete or incomplete pelvic organ prolapse due to injury or disease or surgical complications of pregnancy. Burn scar(s) of the head, face, or neck; scar(s) of the head, face, or neck due to other causes; or other disfigurement of the head, face, or neck. Burn scar(s) or scar(s) due to other causes, not of the head, face, or neck, that are deep and nonlinear. Burn scar(s) or scar(s) due to other causes, not of the head, face, or neck, that are superficial and nonlinear. Other specified and unspecified schizophrenia spectrum and other psychotic disorders. Major or mild neurocognitive disorder due to another medical condition or substance/medication-induced major or (No. Maxilla or mandible, chronic osteomyelitis, osteonecrosis, or osteoradionecrosis of. C-17 Retinal dystrophy (including retinitis pigmentosa, wet or dry macular degeneration, early-onset macular degeneration, rod and/or cone dystrophy. This publication is accessible from the World Federation of Hemophilias website at Mahlangu Department of Hematology, Christian Medical Haemophiia Comprehensive Care Centre, College, Vellore, Tamil Nadu, India Johannesburg Hospital and Department of Molecular Medicine and Haematology, Faculty of Dr. Brewer Health Sciences, National Health Laboratory Department of Oral Surgery, The Royal Infrmary, Services and University of the Witwatersrand, Glasgow, Scotland Johannesburg, South Africa Dr. Mauser-Bunschoten, Kathy Mulder Van Creveldkliniek and Department of Bleeding Disorders Clinic, Health Sciences Center Hematology, University Medical Center Utrecht, Winnipeg, Canada Utrecht, the Netherlands Dr. Bleeding Disorders Comprehensive Care Program, University of Calgary, Foothills Hospital and Dr. Adolfo Llinas Melbourne, Australia Department of Orthopaedics and Traumatology, Fundacion Santa Fe University Hospital Fundacion Cosme y Damian and Universidad de los Andes and Universidad del Rosario, Bogota, Colombia Dr. Ludlam Comprehensive Care Haemophilia and Trombosis Centre, Royal Infrmary, Edinburgh, U. Acknowledgements A professional agency was engaged to assist with the literature search and to grade the evidence. In addition, given the fact that many recommendations are based on expert opinion, a draf version of these guidelines was circulated to many others involved in hemophilia care outside of the writing group. Dose schedules and other treatment regimens are continually revised and new side-efects recognized. Tese guidelines are intended to help develop basic standards of care for the management of hemophilia and do not replace the advice of a medical advisor and/or product insert information. Any treatment must be designed according to the needs of the individual and the resources available. By compiling Introduction The frst edition of these guidelines, published in systems around the world.
Diseases
- Primary pulmonary hypertension
- Sulfatidosis juvenile, Austin type
- Pulmonary fibrosis /granuloma
- Corneal dystrophy
- Negative rheumatoid factor polyarthritis
- Transposition of great vessels
- Nicotine withdrawal
- DOPA-responsive dystonia
- Christianson Fourie syndrome
Cheap fucidin 10 gm without prescription
Surgical incision care Please Remember: **If you notice any increased or change in drainage antibiotic bladder infection buy fucidin 10gm online, redness, swelling, or have a fever of 101. Your surgical incision may be closed with dissolvable sutures and steri-strips, staples or sutures. If you have staples or visible sutures, these will need to be removed 10 to 14 days after your surgery. Arrangements for a home care nurse can be made in the hospital by our home care coordinators. Once your incision is no longer draining, you may take off the dressing and leave the incision open to air. Caution and common sense are recommended and a safe rule of thumb for positions is if it hurts, then dont do it. Driving You can drive when you feel up to driving and are not taking narcotic pain medications or after clearance by your surgeon. This is usually 2 to 3 weeks after a laminectomy and discectomy and 4 to 6 weeks after a lumbar fusion. Begin with short trips first and get out of the car every 30 to 45 minutes to walk around and reposition. You will begin to feel yourself after 2 to 3 weeks and improve over the following weeks. You should tell your employer you will be out of work for approximately 8 to 12 weeks but may be able to return earlier than that. You should start out slowly and work up to walking 30 minutes at least twice a day. Between the narcotic pain medications you will be discharged with and the stress your body has undergone in surgery, you will be tired. Lifting and activity restrictions will be gradually removed as the healing process takes place. Remember to keep your spine in the neutral position and maintain good posture throughout the day. The best way to lift an object is as follows: - Stand close to the object, with feet firmly planted, and in a wide stance. Pushing and pulling objects greater than 5 lbs for the first 6 weeks after surgery is not recommended. If possible, always push rather than pull and remember to pace yourself and take frequent breaks. If side sleeping provides the most benefit, then make sure your legs rest on top of each other with your knees bent or have your top leg slightly forward. Avoid resting your top knee on the bed and sleeping with your arms under your neck and head. A pillow placed behind the body and tucked under the back and hips can help you from rolling out of this position. When sleeping on your back, avoid sleeping with your arms over your head because this puts too much stress on your shoulders and neck. A log roll means to keep your back straight and avoid twisting when rolling from side to side and onto your back. If getting out of bed on the right side ? log roll onto your right side and use your left hand to push yourself up onto your right elbow. Slowly drop your lower legs off the bed as you push yourself up onto your right hand and into a sitting position. It is important to maintain your normal spinal curves when sitting to help minimize this stress, because slouching or sliding down in your chair unnecessarily places strain on your back. Choose a chair that provides support for your lower back and allows your feet to be flat on the floor with your knees the same level as your hips. After surgery, avoid sitting in soft chairs and on couches where your hips drop below your knees. If a chair is too high for you, place your feet on a small stool or box to help maintain correct sitting posture. If you have a telephone that you constantly twist to answer, move the phone so it is in front of you. Support the arm that is holding the phone by placing that elbow on the desk or arm rest and keep your neck in good alignment. You may also want to consider using a headset or headphones if you are on the telephone quite often. Items should always be placed within easy sight and access and keyboards should be placed directly in front of you. To get out of a chair, slide to the edge of the chair and straighten your hips and knees to lift yourself from the chair. If a chair has arm rests use your hands to assist you and remember to keep your back straight. To return to a sitting position, move backwards until the backs of your legs are touching the chair. Place one foot in front of the other and keeping your back straight, lower yourself to the edge of the chair by bending at the hips and knees. This can be found on the orange card or checkout form that you received at one of your clinic visits to the Johns Hopkins Spine Service. If you cannot locate your record number, please contact your surgeons office for help. If you do not complete the survey before your visit you will be asked to arrive 30 minutes early to your follow-up appointment. A staff member will provide you with a paper copy to be completed prior to your visit. X-rays If you cannot have x-rays at Johns Hopkins, please call the office for a prescription ahead of time. It is important to obtain x-rays at your 6 week follow up appointment to evaluate healing. Physical Therapy At your 6 week follow-up appointment in the clinic, you may be given a handout of lower back exercises to begin at home. You may also be given a prescription for outpatient physical therapy, depending on how well you have recovered so far. Walking is a great way to increase your energy level and decrease pain and stiffness. Even if the surgery is not 100% successful, you are probably better and are walking further than you were before surgery. Your own attitude and pro-active approach to your care will lead to a faster recovery. Remember, as we mentioned before, the chances of surgery resolving your leg pain are very high compared to relieving your back pain. Dont stop doing things if you still have pain, simply find an easier way to do them. Inactivity will cause you to stiffen up and will lead to more pain and discomfort. If you dont have time to exercise, try these helpful hints: Take the stairs instead of the elevator Park far away from work or shopping centers and walk to the entrance Stand up and stretch every hour when sitting at a desk Thanks again you choosing the Johns Hopkins Spine Service! Brian Neuman 410-287-5394 (Call between 8:30am - 4:30pm, Monday - Friday) On-call emergency: 410-955-5000 410-955-6070 (Call between 4:30pm - 8:30am weekdays, Saturday - Sunday). The negative effects of smoking are clear: One in every three people who starts smoking will die prematurely of a smoking-related illness, according to the American Lung Association. The benefits of smoking cessation begin within a few minutes of your last cigarette and continue for life, even for people with lung disease. The Risks of Smoking Although the link between smoking and lung cancer is well known, smoking is even more likely to cause a range of other illnesses. According to a 2003 survey published in Morbidity and Mortality Weekly Report, some 8. The most common smoking-related illness was chronic bronchitis (35% of cases), emphysema (24%), heart attacks (19%), non-lung cancer (12%), strokes (8%), and lung cancer (1%). The true number of people affected by smoking is probably much higher than the researchers stated because this study depended on people to report whether a doctor had ever told them they had a certain condition. In addition, the researchers did not look at non- debilitating conditions, such as impotence and sinusitis, that are often caused by cigarette smoking.
Order 10gm fucidin free shipping
Pregnancy and childbirth With good management antibiotics for uti canada order fucidin 10gm visa, women who carry the altered gene causing haemophilia have no more problems with delivering a healthy baby than other mothers. Ideally, if planning a pregnancy, discussing this with a haemophilia specialist who may refer to a genetic counsellor. When the pregnancy is confrmed, contacting the Haemophilia Centre for advice on local obstetric services with experience of haemophilia. Asking the haemophilia and obstetrics teams to consult with each other to plan for a smooth and safe pregnancy and delivery and care for the newborn 11. Checking with the Haemophilia Centre before having any invasive procedures, such as chorionic villus sampling or amniocentesis. Discussing suitable choices for anaesthesia, especially an epidural, with the Haemophilia Centre and obstetrics teams. A normal vaginal delivery is usually recommended unless there are obstetric complications. Identifying the sex of the baby If a pregnant woman knows she carries the altered gene causing haemophilia, it is advisable to determine the sex of the baby before birth, preferably with a non-invasive test with minimal risk to the foetus, such as ultrasound. The woman and her partner can choose if they want to be told the sex of the baby or not before delivery even if the haemophilia and obstetric teams are aware. If neither the couple nor the medical staff know the sex of the baby and no other genetic testing of the foetus has been carried out, the pregnancy and birth will be managed as if the baby is a male with haemophilia to ensure the baby is delivered safely. Testing for haemophilia before birth For a woman or couples who wish to test for haemophilia before birth, there are two main testing options:. Prenatal diagnostic testing: a test during the pregnancy to check the sex of the baby. For these options to be available the gene alteration in the family must be known. There may also be substantial costs involved for these tests and procedures and it may be valuable to clarify this and options for support beforehand. If a pregnant woman has a history of haemophilia in the family and does not know whether she carries the gene, it is important to let the obstetrics team know so that they can plan a safe delivery of the baby with the haemophilia team. This is made by genetic engineering and contains little or no material from human blood or animals. There are several brands available manufactured by different pharmaceutical companies. On demand ? before surgery, childbirth or dental treatment, or after an injury or accident, or once a bleed has started. Factor concentrates are infused (injected) into a vein at home by parents trained to treat their child, or by people themselves when they are confdent enough to do it, or at the Haemophilia Centre. It is used for treating some people with mild haemophilia A and some women with bleeding disorder symptoms. It can help to treat mouth or nosebleeds, gut bleeding or bleeding after dental work. Hormone treatment, such as oral contraceptives (birth control pills), can help women who have heavy menstrual bleeding. Inhibitors After treatment with a clotting factor product, some people with haemophilia may develop antibodies ? known as inhibitors - which make treatment less effective. There are a number of ways to treat inhibitors and many people are successful in overcoming them while others have ongoing problems. Current treatment for people with moderate or severe haemophilia aims to prevent bleeding, pain and joint damage. In Australia the usual treatment for most children and young people with severe haemophilia is prophylaxis, where factor concentrate is injected twice to three times a week to keep factor levels high enough to prevent spontaneous bleeds. Many children and young people have benefted from prophylaxis, which reduces the risk of developing the arthritis and joint problems often experienced by those older people who grew up without adequate treatment due to limited product. This helps to prevent bleeds and protect joints as well as maintaining a healthy body and mind. Even when treating with factor replacement regularly, bleeding into joints and muscles may still occur. Most people with haemophilia will need treatment for injuries apart from minor cuts and scratches or in preparation for surgical and some dental procedures. People with mild haemophilia will not need prophylaxis and will only need treatment for a bleed when it occurs, usually after trauma or injury, or when they are preparing for surgery or some dental work. The local Haemophilia Centre team will help with learning how to recognize a bleed and deal with it promptly, and how to prevent and rehabilitate injuries and bleeds. Treatment product safety Haemophilia treatment product safety is a high priority for the Australian Red Cross Blood Service, government agencies such as the National Blood Authority and the Australian government regulator, Therapeutic Goods Administration, manufacturers, and the bleeding disorders community. There have been no reports that viruses have been transmitted by recombinant products. During the early 1990s many people with bleeding disorders also found that they had been exposed to hepatitis C through the clotting factor concentrates they used for their treatment. The risk of new infections from using human blood products is now thought to be extremely low. However it cannot be entirely excluded, particularly if the risk came from a new or unknown type of blood-borne virus or other micro-organisms causing disease. This can mean taking the opportunity to enjoy what life has to offer, maintaining a healthy lifestyle and good relationships and participating in all sorts of activities, including play, travel, sports, career and other activities that are sustaining or inspiring. At the various stages of life, issues can arise for a person with a bleeding disorder or their family that impact on their ability to enjoy their life. It could be as simple as knowing how to arrange the necessary documents and treatment product to travel. Or for parents, how best to help a child to play and have fun while dealing with the potential for bruises and bleeds. Or it could be dealing with more complicated situations and emotions such as feeling overwhelmed by diagnosis, or that you or your child is somehow different from others, or taking the next step in a personal relationship. The Haemophilia Team is there to help and can give you advice or talk over any problems or concerns. State and Territory Haemophilia Foundations have newsletters to keep members updated and social activities such as family camps, men and womens groups and grandparents groups where people can meet, talk about common experiences and enjoy a meal or a day out. Haemophilia Foundation Australia also has a Youth Program run by young people affected by bleeding disorders. Develop a relationship with the Haemophilia Team to keep in touch about your or your childs wellbeing and any health issues that might arise. With knowledge and planning most people live well with haemophilia and lead active and independent lives. Important Note: this booklet was developed by Haemophilia Foundation Australia for education and information purposes only and does not replace advice from a treating health professional. Always see your health care provider for assessment and advice about your individual health before taking action or relying on published information. The incidence of hemophilia A and B is about 1/5000 males worldwide and affects individuals of all races and socioeconomic groups. Genetic counseling is recommended for families and individuals affected by hemophilia. One third of hemophilia A is due to spontaneous mutations and affected patients have no family history. The risk that a mother of an affected male is a carrier of hemophilia A is about 80%. Pathophysiology Coagulation consists of two processes: primary and secondary hemostasis. An initial platelet plug is established and subsequently replaced by a more stable fibrin clot through secondary hemostasis. Secondary hemostasis involves the coagulation cascade: a sequence of reactions that ultimately leads to the formation of the stable fibrin clot. Clinical Presentations There is a spectrum of disease severity among hemophiliacs. The relative deficiency of activity is manifest by frequency and causes of bleeding episodes. Therefore severe disease is likely to present early in life, while mild and moderate disease may present later.
Order fucidin with mastercard
In a medical context antimicrobial cutting boards 10gm fucidin with amex, it can be paraphrased as the rarer the condition for which we are testing, the greater the percentage of the positive tests will be false positives. It tested the feasibility, utility and reproducibility of results of symptom-limited exercise testing in ambulatory cardiac patients and apparently healthy subjects. A database of more than 10 000 individuals was developed over a period of 10 years. This is based on greatest value in terms of diagnostic outcome: low-risk subjects are likely to have a normal response and high-risk subjects the reverse. In a study of 5 103 patients with symptoms suggestive of angina pectoris in whom the overall sensitivity of the investigation was 70 per cent and specificity 66 per cent, there was a progressive increase in positive predictive value ? 21 per cent, 62 per cent and 92 per cent for low, intermediate and high pre-test probability, respectively ? and a fall in the negative predictive value ? 94 per cent, 72 per cent and 28 per cent, respectively. With the intermediate group, exercise evaluation alone may be insufficient as some authors have noted a statistically significant difference between the pre-/post-test predictive values (P < 0. A significant false-negative rate following investigation does not sit easily in the regulatory environment. One meta-analysis of exercise testing for coronary artery disease in women revealed an overall sensitivity of 61 per cent and a specificity of 70 per cent, comparable to males, but of limited value due to the high number of both false-positive and false-negative results. When an exercise recording is equivocal or abnormal, and the probability of coronary artery disease is intermediate or high, then further evaluation will be clinically indicated. Using exercise or a beta-agonist (such as dobutamine) to increase myocardial oxygen requirement, stress echocardiography demonstrates ventricular wall motion abnormality in the presence of myocardial ischaemia. In one study, the three-year event-free survival in a group of patients of mean age 68 with a normal stress echocardiogram was 97. Another study found a one per cent six-year annual mortality in a large group of patients of mean age 54 years with a normal exercise echocardiogram. But a third, which was the largest that has assessed long-term survival and outcome following a normal stress echocardiogram, concluded that prognosis was not necessarily benign. However, it has to be carried out in an experienced centre and more long-term outcome data are needed. The 8 radiation dose is quite high and is equivalent to 18 mSv, exceeding the radiation dose received during coronary angiography by a factor of two or three although with the most modern equipment, doses are often lower. Imaging takes place following maximum stress and three hours later to permit redistribution of the isotope. Both modalities depend crucially on the prevalence of coronary disease in the population being studied. Many regulatory authorities would regard these figures as failing to provide adequate confidence for certification. It is neither completely sensitive nor completely specific but it is non-invasive. From the certificatory point of view, it may be indicated as the investigation of election when, for example, evidence of satisfactory revascularization is being sought following coronary surgery/angioplasty/stenting. The recommendation to perform the investigation depends on both the clinical and the certificatory situation. The unit is named after Rolf Maximillian Sievert, Swedish medical physicist (1896?1966). It is capable of defining antomy, function, flow, tissue perfusion and the anatomy of the larger coronary vessels. It has an established role in the investgation of the the cardiomyopathies and in the definition of congenital heart disease. It is also useful in the assesment of the ischaemically damaged ventricle, and the great vessels. Electron-beam Computerized Tomography and Multi-Detector Computed Tomography Coronary Angiography 1. At a recent American College of Cardiology consensus conference, a 70 per cent predictive accuracy for obstructive disease was identified for the technique but with lower specificity. It is not required for regulatory purposes but may prove useful once there are more data on its prognostic power. If an aircrew member undergoes the investigation for whatever reason, and the result suggests the possibility of coronary artery disease, further investigation is indicated using available techniques. It has not yet replaced coronary angiography in the pre-intervention assessment of coronary artery disease. If other tests have not been reassuringly negative during an assessment, this investigation may be warranted and certification may not be possible without it. It carries a very small risk of death ? less than one in 5 000 in healthy individuals (such as an aircrew population) with a slightly higher risk of vascular damage to the vessel of entry or due to stripping of the intima of the coronary artery. In private flyers, the procedure is difficult to justify for certificatory purposes alone, except at the insistence of the individual. In these people, the tendency to regard them as fit, based only on their coronary anatomy, should be regarded with caution as they may subsequently demonstrate a myocardial abnormality. They include hypertension, hyperlipidaemia, diabetes, smoking, obesity and lack of exercise. The Metabolic Syndrome (sometimes known as 10 Syndrome X or Reavens Syndrome ? hypertension, hyperlipidaemia, insulin resistance and trunkal obesity) carries a significantly increased risk of such event. Vascular risk factors predict coronary artery disease and coronary artery disease predicts coronary events. Hypertension has been called the most powerful and predictive of all the vascular risk factors although in reality age is the most important. To assess one risk factor in isolation is not appropriate as they all interact powerfully and multiple risk factors present in minor extent are as lethal as a single one present in large extent. There is no provision in Annex 1 which directly relates to vascular risk factors but in the introduction to Chapter 6, Note 2 states that predisposing factors for disease, such as obesity and smoking, may be important for determining whether further evaluation or investigation is necessary in an individual case. If the 10-year cardiovascular mortality is < 5 per cent and there is no evidence of target organ damage, slightly higher levels are tolerable in the short term. In the presence of diabetes and micro-albuminuria, the lower target of 130/80 mm Hg is applicable. A pressure consistently >160/95 mmHg is disqualifying from all classes of medical certification. On commencement or following change in treatment or its dosage, the pilot should be assessed temporarily unfit until there is evidence of stable control and freedom from side effects, such as orthostatic hypotension. Intervention against vascular risk factors is influenced to some extent by the presence or absence of other risk factors and whether or not there is evidence of target organ damage (left ventricular hypertrophy, loss of vascular compliance, reduced renal function, micro-albuminuria in diabetes). From the point of view of good clinical practice, which should be inseparable from good regulatory practice, the European Society Committee for Practice Guidelines (like other groups) has developed risk tables, calculating 10-year cardiovacsular mortality in males and females in high- and low-risk countries, which relate age, systolic blood pressure, total cholesterol and smoking. A subject in middle age with a 10-year mortality of > 5 per cent is in need of specialist advice. Pilots, on the basis of their regular medical review and need to maintain medical fitness, should be in an ideal position to instigate preventative strategies with the object of health maintenance. It has a trajectory of many years duration and may present abruptly with some cerebrovascular or myocardial event. In Europe, there is a north-south gradient, death from coronary heart disease being three times more common in the north than in the southern olive belt. There is also an East-West gradient: heart-attack rates in Western Europe are generally lower than those in Eastern 12 Europe. South Asians, for example, both locally and following emigration, now demonstrate rates that are generally some 50 to 60 per cent higher than those observed in the West. Numerous factors, including inherited metabolic anomalies and insulin resistance, are involved. Japan and China, sharing with other countries in the Far East commendably low mean levels of plasma cholesterol and some of the lowest heart-attack rates in the world, are showing signs of increase in the prevalence of coronary artery disease. Japanese who emigrate to the United States tend, like other migrant populations, to assume the risk of their country of adoption. In one Contracting State, a unit of alcohol is defined as 15 mL of pure alcohol (ethyl alcohol, ethanol), which is equivalent to one standard serving of beer, wine or spirits. If not accompanied by food, one unit of alcohol will entail a blood alcohol concentration of c. Salim Yusuf of McMaster University, Canada, involving > 29 000 people in 52 countries (published in 2004). The presence of one or more vascular risk factors implies a greater probability of event in an individual without identifying whether or when it might occur. It remains what has been called the prevention paradox that the greatest number of events will be seen in those individuals with a near-normal vascular risk profile ? on account of their far greater numbers. Predictions on the probability of an event, which should be over a defined period, often a year, should be based on data from an age- and sex-matched control population.
Syndromes
- Kidney stones
- Any fracture in an infant too young to walk or crawl
- Coughing
- Active crying
- Enriched breads and fortified cereals
- Aspirin or nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, Motrin, Advil, or Aleve
- Exercise regularly.
- Falls while climbing at work or during recreation can cause spinal cord injuries. Defensive driving and wearing seat belts greatly reduces the risk of serious injury if there is an automobile accident.
Discount 10gm fucidin with amex
To which extent this event occurs in physiological condition is matter of investigation because the ratio between uncleaved and cleaved Gpcs varies according to the gpc family member and the tissue- specific context antibiotic resistance food purchase 10 gm fucidin with visa. The N-terminal Gpc fragment is not membrane-associated and, once generated, it can remains linked to its C-terminal half through one or more disulfide bridges (De Cat et al. Thus, proteolytic processing can provide a molecular strategy to rapidly make available a secreted Gpc product, if needed, as such a form could be released from producing cells simply following redox changes of the extra- cellular environment. The human and mouse genome contain six Gpc family members, Gpc-1 to Gpc-6 in humans and gpc-1 to gpc-6 in mice (De Cat and David, 2001; Fico et al. However, sequence relationships and exon organizations suggest that mammalian gpcs consist of two distinct subfamilies (De Cat and David, 2001; Fico et al. The first subfamily includes gpc-1, -2, -4 and -6 genes with amino acid sequence homology ranging from 40?60% and composed of nine exons. The other subfamily incorporates gpc-3 and -5, with amino acid sequences 40% identical and containing eight exons. Of note, gpc-6 maps near to gpc-5 on mouse chromosome 14 and on human chromosome 13. Gpc-4, which is most homologous to gpc-6 maps to chromosome Xq26 near to gpc-3, which is highly related to gpc-5 (De Cat and David, 2001; Fico et al. Therefore, members of the different subfamilies are inclined to cluster on the same chromosome. Whether gpc subfamilies and the genomic linkage of different members have evolved from a series of gene and genome duplications is still a matter of debate. In support of this possibility there are studies in organisms such as Drosophila and zebrafish showing the existence of distinct orthologs for each mammalian subfamily and their genomic linkage (Filmus and Capurro, 2008). It will be interesting to examine to what extent the appearance of gpc subfamilies might underlie the evolution of functional similarities in members of the same subfamily and functional differences among those more divergent. In this context, studies on Dally and Dally-like aimed at distinguish their activity on Hh have shown that Dally-like but not Dally is required for Hh response in a Drosophila cultured cell assay (Williams et al. Intriguingly, Gpc-4 and -6, which are the mammalian Gpcs most closely related to Dally-like, complement Dally- like function in this biological system (Williams et al. In contrast, Dally and its ortholog Gpc-3 exhibit trans-dominant negative activities (Williams et al. These Signalling Mechanisms Underlying Congenital Malformation: the Gatekeepers, Glypicans 23 studies suggest a large trend in which related Gpc members may have evolved similar activities in distinct cellular contexts, but further understanding will come from studies on other signalling activities. Glypicans: From structural compounds to signalling molecules Once considered as acting merely as structural components of the extra cellular matrix, Gpcs are now widely recognized as essential modulator of many biological processes. These include their role as carriers in cellular uptake of growth promoting polyamines such as spermine (Casero and Marton, 2007; Fransson et al. The mechanisms underlying polyamines uptake has been analyzed in several systems and discussed in previous reports (Belting, 2003; Fransson et al. To date, Gpcs are also considered as potential carriers of cell-penetrating peptides. Cell- penetrating peptides are short cationic peptides extensively studied in medicine as drug delivery agents for the treatment of different diseases including cancer and virus infection (Rajendran et al. Therefore, Gpcs mediated uptake of cell-penetrating peptide is currently evaluated as a new strategy to enhance target-specific delivery of a large variety of entrapped therapeutic drugs. Research on Gpcs has further increased due to the discovery that they act at the interface between the extra cellular environment and the inner cellular domain to fine tune inputs triggered by key secreted regulatory proteins. Being mostly extracellular, Gpcs are involved in the regulation of various signalling pathways triggered by secreted peptides including that of Wnt, Fgf, Hh, bone morphogenic protein (Bmp), insulin-like growth factor and hepatocyte growth factor (Fico et al. The functional relevance of Gpcs as signalling modulators has come from the genetic analysis and embryological manipulation of Gpcs in different species and in cultured cells (Table 1). This table reports the major phenotypes observed by genetic and embryological studies on glypican genes and the main involved signals For example, in vitro studies have shown that Gpc4 positively modulated hepatocyte growth factor activity during renal epithelial branching morphogenesis (Karihaloo et al. Mice lacking Gpc3 are affected by overgrowth, renal cystic dysplasia and limb defects. Some of these phenotypes are consistent with defects in Wnt and Bmp signalling pathways, respectively (Grisaru et al. Additional studies have also shown that the developmental overgrowth observed in gpc3- null mice is, at least in part, a consequence of the hyperactivation of the Hh pathway indicating that Gpc3 inhibits Hh Gallet et al. Interestingly, Gpc5 stimulates the proliferation of rhabdomyosarcoma cells by eliciting a positive action on Hh signalling (Li et al. Signalling Mechanisms Underlying Congenital Malformation: the Gatekeepers, Glypicans 25 these findings reveal that members of the Gpc family can display opposite roles in the regulation of a given signalling protein. It has been proposed that Lon-2 negatively regulates Bmp signalling as lon-2 mutants recapitulate phenotypes caused by Bmp over-expression (Gumienny et al. Another example is the Zebrafish knypek, which encodes the gpc homolog to mammalian Gpc4/Gpc6 (Topczewski et al. In particular, reducing Gpc4 (Xgly4) disrupts cell movements during gastrularion (Ohkawara et al. We have also shown that loss-of Gpc4 function in Xenopus embryos impairs forebrain patterning and cell survival from early neural plate stages onwards, and that these early developmental defects result in brains affected by microcephaly at later stages (Fig. Inhibition of Fgf signalling results in dorsal forebrain phenotypes similar to those of Xgly4 depleted embryos, indicating that establishment and patterning of the dorsal forebrain territory may require modulation of Fgf signalling by Xgly4 (Galli et al. Side view of Xenopus embryos at tail bud stage showing expression of the dorsal forebrain marker emx-2 as detected by whole mount in situ hybridization (arrow in all panels). Xenopus embryos were injected at 2 cell stage with morpholino oligos to interfere with Gpc-4 activity. Injections were done by using control morpholino (controlMo), or morpholino targeting gpc-4 (gpc-4Mo). In Drosophila the Gpc Dally-like is required for Hh signalling in the embryonic ectoderm whereas both Gpcs Dally and Dally-like are required and redundant in Hh movement in developing wing imaginal discs (Han et al. Additional studies on the wing disc patterning have also demonstrated that in Dally and Dally-like mutants the distribution and signalling of Wnt and Bmp family members, Wingless (Wg) and Decapentaplegic (Dpp) respectively, are altered (Nybakken and Perrimon, 2002). Overall, these and other studies reveal that different cell types can take advantage of Gpc-mediated regulation to control signal supply during distinct developmental processes. In addition, they show that vertebrate and invertebrate Gpcs have diverse and specialized functions towards a given signalling protein including their capability of enhancing or suppressing its activity in a stage- and/or tissue-specific regulated manner. One question that has arisen is whether these properties are conferred by their unique structural motifs. Gpcs trafficking and shedding can both lead to a gain of signal, down-regulation properties and cell non-autonomous activities (Yan and Lin, 2009). These issues are the subjects of intense investigation, and a growing body of data is being published on Gpc mechanism of action. Also, the Gpc-dependant Fgf binding and activation of receptors is nearly abolished when cells are treated with chlorate to inhibit Gpc sulfatation (Steinfeld et al. Potential mechanisms of action may include immobilizing of the ligand, increasing its local concentration, presenting it to a signalling receptor, or otherwise modifying the molecular encounters between ligands and receptors. The expected overall effect is thus enhancing receptor activation at low ligand concentrations. This includes the binding and stimulation of Wg (the drosophila homolog of Wnt) signalling in the wing imaginal disc by Dally as well as the ability of human Gpc-5 to interact with Hh and enhance its growth promoting activity in rhabdomyosarcoma cells Yan and Lin, 2009; Li et al. Recent studies have revealed that the co-receptor function of Gpcs can also provide a new paradigm of cell-cell communication. In the stem cell niche associated with germ cells the Gpc Dally is critical for making and maintaining the female germ cells (Hayashi et al. However, in this stem cell niche, dally is expressed by the cap cells, which also produce the Dpp signalling molecule, but not in the receiving cells (germ cells), which instead express Dpp receptor (Hayashi et al. These findings have raised questions and interest about the underlying molecular mechanisms. Studies in cultured cells have provided evidence that Dally enhances Dpp signalling in trans through a contact- dependent mechanism allowing the complementation of co-receptor-receptor complexes in adjacent cells (Dejima et al. Therefore, unlike typical co-receptor functions, Dally can serves as a trans co-receptor for Dpp when it has to enhance its signalling on neighboring cells. So far the mechanism for contact-dependent signalling has been mainly attributed to membrane-bound ligands and receptors such as Delta-Notch and Ephrins and their receptor tyrosine kinases (Hainaud et al. The fact that Gpcs act as trans activator partners establishes new strategies for crosstalk between adjacent cells during tissue assembly and maintenance. As co-receptors and trans co-receptor, Gpcs modulate ligand-receptor encounters that can activate and inhibit cell proliferation, motility, and differentiation.
Cheap fucidin 10 gm fast delivery
The Guides main goal is to promote better management of acute low back pain to reduce chronicity infection prevention and control generic fucidin 10gm with amex. Based on extensive international experience the development in New Zealand of clinical guidelines for problems such as low back pain is part of an international trend towards evidence based healthcare ? led by the New Zealand Guidelines Group. Developed to international standards, the methodology and the Guide to Assessing Psychosocial Yellow Flags have already received international acclaim. Since the 1987 work of the Quebec Task Force on Spinal Disorders (see Table 1), evidence based guidelines for acute low back pain have been produced in the United States, the United Kingdom and New Zealand. However, international research indicates that evidence based guidelines alone will not encourage treatment providers to adopt best clinical practice. The implementation strategy therefore involves: ll Educational forums that include local treatment providers and at least one member of the Expert Panel. The Panel noted there is an opportunity for health professionals to broaden their skills in the management of acute and recurrent low back pain. This review process began in late 2001 using methods based on principles promoted by the Cochrane Collaboration and the New Zealand Guidelines Group. A search was conducted for articles published since 1999, using major electronic databases and the keyword back pain. The results of this review were collated and divided into key areas for presentation to the Expert Panel. In addition to those concerned solely with acute low back pain, many applied to recurrent, sub-acute or chronic low back pain. Advice on Returning to Work Rationale this search identied literature on advice on return to work (employment), modifying work tasks and medical work certication. These were reviewed and summarised, and professional organisations and Panel members were invited to submit relevant literature. The Expert Panel considered each of the studies and produced a draft document, which has been revised to produce this nal version. The Expert Panel found no evidence that international research does not apply in New Zealand. This assessment can be used to target effective early management and prevent the onset of these problems. Be aware of, and take into account, reading difculties and different cultural backgrounds. This Quick Reference Guide to Assessing Psychosocial Yellow Flags in Acute Low Back Pain is to be used in conjunction with the full document. Professor of Spine Biomechanics, Faculty of Applied Health Sciences, Department of Kinesiology, University of Waterloo mcgill@uwaterloo. But after writing two textbooks based on our hundreds of scientific publications, I feel as though I have McGill, S. Low back disorders: Here are few thoughts for exercise professionals who deal with Evidence based prevention and issues related to the assessment and design of therapeutic exercise rehabilitation, Second for the back, to assist them in becoming elite professionals. Many Edition, Human clinicians follow a recipe for assessment, treatment or performance Kinetics Publishers, training. The program and approach Back: Assessment and introduced here will help you to become an elite corrective exercise therapeutic execise, and training specialist. The cause (and elimination of it) the first step in any exercise progression is to remove the cause of the pain, namely the perturbed motion and motor patterns. Giving this type of client stretches such as pulling the knees to the chest may give the perception of relief (via the stimulation of erector spinae muscle stretch receptors) but this approach only guarantees more pain and stiffness the following day as the underlying tissues sustain more cumulative damage. Eliminating spine flexion, particularly in the morning when the discs are swollen from the osmotic superhydration of the disc that occurs with bedrest, has been proven very effective with this type of patient. Realize that the spine discs only have so many numbers of bends before they damage. Keep the bends for essential tasks such as tying shoes rather than using them up in abdominal training. Many lifestyle and occupational examples are provided in the textbook Low back disorders: Evidence based prevention and rehabilitation to guide the elimination of the cause of a clients back troubles ? the clinician will find that half of 2 their initial effectiveness will be due to preventing the cause (ie, a flawed movement pattern)! Consider the client who stands slouched where the back muscles are chronically contracted to the point of chronic muscle pain. The clinician addresses the postural cause and corrects standing to shut the muscles off and remove the associated crushing load from the spine. Building the scientific foundation: Myths and controversies regarding spine function and injury mechanisms are common. Consider the cause of back troubles, specifically the common perception regarding common injury pathways in which the back is hurt in an event. Generally statistics are compiled from epidemiological approaches which ignore the large role of cumulative trauma. Compensation board data is often used however, and they ask clinicians to fill out reports and name the event that caused the injury. Kinesiologists and clinicians know that twisting is different from generating twisting torque, but very few of the individuals filling out the reports will know. Further, despite the injury reporting system geared to the reporting of the event associated with the injury, very few back injuries occur this way. For example the damaging mechanism leading to herniation, or prolapse, is repeated lumbar flexion requiring only very modest concomitant compressive loads (Callaghan and McGill, 2001). With repeated flexion cycles the annulus breaches layer by layer with progressive delamination of the layers (Tampier et al 2007). This allows gradual accumulation of nucleus material between the delaminated layers. The location of the annulus breaches can be predicted by the direction of the bend. Specifically, a left posterior-lateral disc bulge will result if the spine is flexed with some additional right lateral bend (Aultman et al, 2004). Subsequent twisting leads circumferential rents in the annulus that tends to make McKenzie extension approaches for these clients useless, or even exacerbating (Marshall and McGill, 2010). This is critical information for the clinician, both in terms of prevention and in treatment. Avoiding this specific directional cause will lead to optimal therapeutic exercise design together with elimination of activities in the patients daily routine identified as replicating the cause. Many therapy approaches have the objectives of strengthening muscle and increasing spine range of motion. This is problematic (Parks et al, 2003) since those who have more motion in their backs have a greater risk of having future back troubles. Strength may, or may not, help a particular individual as strength without control and endurance to repeatedly execute perfect form increases risk. Interestingly, the differences between many troubled backs (the chronic back with recurrent episodes) and matched asymptomatic controls performing the same jobs have been shown to be variables other than strength or mobility. Rather deficits in motion and motor patterns have been documented as being more critical and thus should be targets for therapeutic exercise. Generally, they walk, sit, stand and lift using mechanics that increase back loads. Many of them have stronger backs but are less endurable than matched asymptomatic controls (McGill et al, 2003). They tend to have more motion in their backs and less motion and load in their hips. A common aberrant motor pattern is known as gluteal amnesia (McGill, 2007) which may be both a 3 common consequence of back troubles and probably a cause of them as well. Obviously for this category of client, exercises to enhance the integration of the gluteal muscles will help their backs, and also their knees. Optimal back exercise therapy results from the identification of these patients with perturbed patterns followed by specific corrective exercise ? this precedes all other exercise therapy. The science of spine stability: Effective spine stabilization approaches must begin with a solid understanding of what stability is. From a spine perspective it has little to do with the ability to balance on a gym ball. This is simply the ability to maintain the body in balance which is important but does not address the unstable spine.
Buy fucidin 10 gm low cost
In order to examine the learning curve of fellows antibiotic treatment for mrsa order fucidin 10gm without a prescription, exposure parameters of the first 50 procedures were compared with the last 50 performed (Table 33). Some variability can be expected as a result of normal variations in calibrations and in performance of dosimetry devices. Other potential concerns relate to the guidance that might be provided to facilities in the proper measurement of air kerma or absorbed dose. For example, the wide variance in results for the two trials of Participant A indicates the difference that feedback on methods and techniques can make. For any facility, resources must be available to check ones measurements and verify their accuracy. Obtaining agreement to within 10% requires careful attention to details regarding dosimetric measurements. Our intercomparisons of dosimetry using Gafchromic media (Figures 3, 4 A and 4 B) demonstrate that results among various centers can be consistent, with the usual variations expected due to procedure setup, calibration of electronic dosimeters, and normal variances due to testing conditions (e. However, results are not guaranteed and those of Participant E demonstrate an unusual variance. Therefore, it is essential that participants in any dosimetry program be provided with resources to verify the accuracy of their measurements. As a result of our intercomparisons of calibrations, it was decided to make Participant B the repository and standard of this exercise for all Gafchromic media results. This provided a resource of confidence in the consistency of all further patient-oriented dosimetry. It avoided errors that might result from the different methodologies of the participants. The observed differences in demographics demonstrate how body mass and patient age vary widely among institutions and countries due to many different factors, including genetic heritage, diet, patient selection and more. Considering the fact that body mass plays an important role in fluoroscopic and fluorographic dose rates, it might be predicted that certain countries are at greater risk for high dose delivery to patients than are others. Body mass index and maximum skin dose Figures 6B, 7C,F,I and 8C,F,I demonstrate how body mass index is related to the maximum skin dose for all cardiac procedures, where maximum skin dose is defined as that measured with the radiochromic film. The data from some centers (Table 6) suggest this with a relatively strong correlation while most others demonstrate a weak or absent correlation. The positive slope is likely related to the automatic methods of dose and dose rate control by the fluoroscope with increasing body mass. These factors might be location of the diseased vessels, tortuosity of vessels, extent and type of disease, number of involved vessels, etc. For coronary ablation procedures, Figures 7I and 8I suggest diverse relationships. For Participant B body mass index seems to play a minimal role in maximum skin dose. While the correlation was not found to be significant, a lack of statistical significance does not mean that the trend is not correct. The marked scatter about the regression line for Participant F demonstrates a greater variation in procedures than those for Participant B. Examination in Table 16 of the fluoroscopy-on times shows that the on-times for Participant F are more than twice those of Participant B on the average. But, there exists a marked difference in the age distribution of ablation patients for Participant F (mean 38. Body mass index is not a strong predictor of high skin dose risk to patients from fluoroscopy. Other factors appear to play a more important role in determining the likely dose delivered to a patient. A large patient will exacerbate dose rate delivery when an exceptionally high dose procedure is performed. The fact that the data show positive trends with increasing fluoroscopy time is an obviously anticipated result. The widely scattered data within each facility are likely due to variations in body habitus, geometric beam orientations, and varying settings of the fluoroscope for each procedure. But the wide variation in slope of the relationship indicates that some centers are better able to conserve dose with increasing fluoroscopy time. The obvious factors involved would be due to either differences in procedural techniques or due to differences in equipment performance, or both. In fact, Participant F noted that his physicians frequently used high electronic magnification and that this often caused the machine to operate at unusually high dose rates in fluoroscopy. The simple linear regression illustrates that the rate of dose build-up with time at the study centers varies by a factor of about 4, suggesting that considerable dose savings can be achieved through effective operational use and/or design of equipment. The higher doses for very short fluoroscopy times during coronary angiography Figure 8. A suggests that modes of operation which bypass recording of time during fluoroscopy must have been used by Participant F. In researching the causes for this result, Participant F discovered that the magnification modes frequently used by the physicians resulted in much higher skin dose rates than previously identified during routine physics investigations. Other factors found to result in the higher doses were the use of higher pulse-rate fluoroscopy and probable smaller distance between the patient and the X ray tube. Potential factors not thoroughly investigated include potentially different patient populations with different complexities in procedures. The intent of this investigation was not to completely answer all questions regarding the reasons for these differences, but rather to make measurements to determine weather differences exist. In this case, it is clear that a situation existed that was unknown to the facility and dose monitoring made the discovery possible. While difficulty of procedures could potentially explain this result, the use of higher dose rate modes is the more likely explanation. The higher doses for Participant F suggest that higher dose rate modes of operation or higher dose rate geometries must have been employed compared to those used by Participant B. As previously noted, the fluoroscopy-on time alone does not explain the larger doses delivered at site F. If Participant F employed greater geometric magnification than those of Participants B, then higher dose rates for similar fluoroscopy times would result as a matter of the inverse-square law. Participant F noted that the physicians did not always move the image receptor toward the patient. Also, on one of the fluoroscopy units for Participant F, it was noted that the X ray field was larger than anticipated. The fact that this shows more in the ablation procedures than in the other cardiac procedures reflects the fact that less cine-images are acquired and more fluoroscopy is used during the ablation procedures. We speculate this might be due in part to our method of ascertaining maximum skin dose which may be more conservative than some. It might also be due to a more aggressive use of collimation by some of our participants and a higher dose rate employed by others. Dose calibration strip and maximum skin dose Data on skin dose as derived by visual inspection from a dose calibration strip might be useful as a real-time device to monitor skin dose during a procedure. When used cautiously for guidance, the strip will be useful in monitoring skin dose in real time for individual patients and should be accurate to within a factor of two. There exist some physical obstacles to correctly using a dose calibration strip, as, for example, the well-known Mach effect. Some research into standardizing the use of this visual estimate of dose is a matter for future investigation. The lack of correlation of the results suggests strongly that placement of the skin dose monitor a priori over the critical skin area is next to impossible and use of a skin dose monitor during cardiac procedures might be more misleading than helpful. Effect of physician experience the major emphasis of training programs in invasive cardiology is generally related to the possible increased risk of complications with less attention is devoted to the radiation exposure of patients. The authors do not comment on this finding and discussion is limited to comparison between fluoroscopy times in the two groups. Also in the present work, the exposure of patients was significantly increased during fellows training, this increase being mainly due to fluoroscopy, as more time is required for manipulating catheters by a less experienced operator and maybe a less thorough knowledge how to use the equipment. Other parameters increased to a lesser extent: this is of note, as cine runs determine 60-70% of exposure in diagnostic examinations. It is likely that the close supervision by staff members made this possible: since the senior cardiologists were almost always scrubbed and beside the fellows, they must have stopped them from manipulating the catheter after an agreed upon time had expired.
Purchase fucidin 10 gm fast delivery
Closure Check the left L4-L5 foramen and Lumbar Interbody Fusion site for any bone fragments or extraneous soft tissue infection 5 weeks after birth discount 10gm fucidin overnight delivery. Once satisfactory decompression of the exiting and traversing nerve roots is confirmed the wound should be closed. L(mm) W(mm) A(?) H(mm) L(mm) W(mm) A(?) H(mm) 3410-2506 25 11 0 6 3410-2806 28 11 0 6 3410-2507 25 11 0 7 3410-2807 28 11 0 7 3410-2508 25 11 0 8 3410-2808 28 11 0 8 3410-2509 25 11 0 9 3410-2809 28 11 0 9 3410-2510 25 11 0 10 3410-2810 28 11 0 10 3410-2511 25 11 0 11 3410-2811 28 11 0 11 3410-2512 25 11 0 12 3410-2812 28 11 0 12 3410-2513 25 11 0 13 3410-2813 28 11 0 13 3410-2514 25 11 0 14 3410-2814 28 11 0 14 3410-2515 25 11 0 15 3410-2815 28 11 0 15 3410-2516 25 11 0 16 3410-2816 28 11 0 16 3414-2506 25 11 4 6 3414-2806 28 11 4 6 3414-2507 25 11 4 7 3414-2807 28 11 4 7 3414-2508 25 11 4 8 3414-2808 28 11 4 8 3414-2509 25 11 4 9 3414-2809 28 11 4 9 3414-2510 25 11 4 10 3414-2810 28 11 4 10 3414-2511 25 11 4 11 3414-2811 28 11 4 11 3414-2512 25 11 4 12 3414-2812 28 11 4 12 3414-2513 25 11 4 13 3414-2813 28 11 4 13 3414-2514 25 11 4 14 3414-2814 28 11 4 14 3414-2515 25 11 4 15 3414-2815 28 11 4 15 3414-2516 25 11 4 16 3414-2816 28 11 4 16 3418-2507 25 11 8 7 3418-2806 28 11 8 6 3418-2508 25 11 8 8 3418-2807 28 11 8 7 3418-2509 25 11 8 9 3418-2808 28 11 8 8 3418-2510 25 11 8 10 3418-2809 28 11 8 9 3418-2511 25 11 8 11 3418-2810 28 11 8 10 3418-2512 25 11 8 12 3418-2811 28 11 8 11 3418-2513 25 11 8 13 3418-2812 28 11 8 12 3418-2514 25 11 8 14 3418-2813 28 11 8 13 3418-2814 28 11 8 14 3418-2815 28 11 8 15 3418-2816 28 11 8 16 16 Dimension Dimension Part No. L(mm) W(mm) A(?) H(mm) L(mm) W(mm) A(?) H(mm) 3610-2607 11 26 0 7 3610-2807 11 28 0 7 3610-2608 11 26 0 8 3610-2808 11 28 0 8 3610-2609 11 26 0 9 3610-2809 11 28 0 9 3610-2610 11 26 0 10 3610-2810 11 28 0 10 3610-2611 11 26 0 11 3610-2811 11 28 0 11 3610-2612 11 26 0 12 3610-2812 11 28 0 12 3610-2613 11 26 0 13 3610-2813 11 28 0 13 3610-2614 11 26 0 14 3610-2814 11 28 0 14 3610-2615 11 26 0 15 3610-2815 11 28 0 15 3610-2616 11 26 0 16 3610-2816 11 28 0 16 3614-2607 11 26 4 7 3614-2807 11 28 4 7 3614-2608 11 26 4 8 3614-2808 11 28 4 8 3614-2609 11 26 4 9 3614-2809 11 28 4 9 3614-2610 11 26 4 10 3614-2810 11 28 4 10 3614-2611 11 26 4 11 3614-2811 11 28 4 11 3614-2612 11 26 4 12 3614-2812 11 28 4 12 3614-2613 11 26 4 13 3614-2813 11 28 4 13 3614-2614 11 26 4 14 3614-2814 11 28 4 14 3614-2615 11 26 4 15 3614-2815 11 28 4 15 3614-2616 11 26 4 16 3614-2816 11 28 4 16 3618-2607 11 26 8 7 3618-2807 11 28 8 7 17 3618-2608 11 26 8 8 3618-2808 11 28 8 8 3618-2609 11 26 8 9 3618-2809 11 28 8 9 3618-2610 11 26 8 10 3618-2810 11 28 8 10 3618-2611 11 26 8 11 3618-2811 11 28 8 11 3618-2612 11 26 8 12 3618-2812 11 28 8 12 3618-2613 11 26 8 13 3618-2813 11 28 8 13 3618-2614 11 26 8 14 3618-2814 11 28 8 14 3618-2615 11 26 8 15 3618-2815 11 28 8 15 3618-2616 11 26 8 16 3618-2816 11 28 8 16 Dimension Dimension Part No. L(mm) W(mm) A(?) H(mm) L(mm) W(mm) A(?) H(mm) 3710-2408 24 32 0 8 3714-2409 24 32 4 9 3710-2409 24 32 0 9 3714-2410 24 32 4 10 3710-2410 24 32 0 10 3714-2411 24 32 4 11 3710-2411 24 32 0 11 3714-2412 24 32 4 12 3710-2412 24 32 0 12 3714-2413 24 32 4 13 3710-2413 24 32 0 13 3714-2414 24 32 4 14 3710-2414 24 32 0 14 3714-2415 24 32 4 15 3710-2415 24 32 0 15 3714-2416 24 32 4 16 3710-2416 24 32 0 16 3714-2417 24 32 4 17 3710-2417 24 32 0 17 3714-2418 24 32 4 18 3710-2418 24 32 0 18 3714-2419 24 32 4 19 3710-2419 24 32 0 19 3718-2409 24 32 8 9 3732-2409 24 32 12 9 3718-2410 24 32 8 10 3732-2410 24 32 12 10 3718-2411 24 32 8 11 3732-2411 24 32 12 11 3718-2412 24 32 8 12 3732-2412 24 32 12 12 3718-2413 24 32 8 13 3732-2413 24 32 12 13 3718-2414 24 32 8 14 3732-2414 24 32 12 14 3718-2415 24 32 8 15 3732-2415 24 32 12 15 3718-2416 24 32 8 16 3732-2416 24 32 12 16 3718-2417 24 32 8 17 3732-2417 24 32 12 17 3718-2418 24 32 8 18 3732-2418 24 32 12 18 3718-2419 24 32 8 19 3732-2419 24 32 12 19 3734-2409 24 32 14 9 3720-2908 29 38 0 8 3734-2410 24 32 14 10 3720-2909 29 38 0 9 3734-2411 24 32 14 11 3720-2910 29 38 0 10 3734-2412 24 32 14 12 3720-2911 29 38 0 11 3734-2413 24 32 14 13 3720-2912 29 38 0 12 3734-2414 24 32 14 14 3720-2913 29 38 0 13 3734-2415 24 32 14 15 3720-2914 29 38 0 14 3734-2416 24 32 14 16 3720-2915 29 38 0 15 3734-2417 24 32 14 17 3720-2916 29 38 0 16 3734-2418 24 32 14 18 3720-2917 29 38 0 17 3734-2419 24 32 14 19 3720-2918 29 38 0 18 19 Dimension Dimension Part No. L(mm) W(mm) A(?) H(mm) L(mm) W(mm) A(?) H(mm) 3810-4008 18 40 0 8 3810-4508 18 45 0 8 3810-4009 18 40 0 9 3810-4509 18 45 0 9 3810-4010 18 40 0 10 3810-4510 18 45 0 10 3810-4011 18 40 0 11 3810-4511 18 45 0 11 3810-4012 18 40 0 12 3810-4512 18 45 0 12 3810-4013 18 40 0 13 3810-4513 18 45 0 13 3810-4014 18 40 0 14 3810-4514 18 45 0 14 20 3810-4015 18 40 0 15 3810-4515 18 45 0 15 3810-4016 18 40 0 16 3810-4516 18 45 0 16 3816-4008 18 40 6 8 3816-4008 18 40 6 8 3816-4009 18 40 6 9 3816-4009 18 40 6 9 3816-4010 18 40 6 10 3816-4010 18 40 6 10 3816-4011 18 40 6 11 3816-4011 18 40 6 11 3816-4012 18 40 6 12 3816-4012 18 40 6 12 3816-4013 18 40 6 13 3816-4013 18 40 6 13 3816-4014 18 40 6 14 3816-4014 18 40 6 14 3816-4015 18 40 6 15 3816-4015 18 40 6 15 3816-4016 18 40 6 16 3816-4016 18 40 6 16 3830-4008 18 40 10 8 3830-4008 18 40 10 8 3830-4009 18 40 10 9 3830-4009 18 40 10 9 3830-4010 18 40 10 10 3830-4010 18 40 10 10 3830-4011 18 40 10 11 3830-4011 18 40 10 11 3830-4012 18 40 10 12 3830-4012 18 40 10 12 3830-4013 18 40 10 13 3830-4013 18 40 10 13 3830-4014 18 40 10 14 3830-4014 18 40 10 14 3830-4015 18 40 10 15 3830-4015 18 40 10 15 3830-4016 18 40 10 16 3830-4016 18 40 10 16 3832-4008 18 40 12 8 3832-4008 18 40 12 8 3832-4009 18 40 12 9 3832-4009 18 40 12 9 3832-4010 18 40 12 10 3832-4010 18 40 12 10 3832-4011 18 40 12 11 3832-4011 18 40 12 11 3832-4012 18 40 12 12 3832-4012 18 40 12 12 3832-4013 18 40 12 13 3832-4013 18 40 12 13 3832-4014 18 40 12 14 3832-4014 18 40 12 14 3832-4015 18 40 12 15 3832-4015 18 40 12 15 3832-4016 18 40 12 16 3832-4016 18 40 12 16 Dimension Dimension Part No. L(mm) W(mm) A(?) H(mm) L(mm) W(mm) A(?) H(mm) 3810-4508 18 45 0 8 3810-5008 18 50 0 8 3810-4509 18 45 0 9 3810-5009 18 50 0 9 3810-4510 18 45 0 10 3810-5010 18 50 0 10 3810-4511 18 45 0 11 3810-5011 18 50 0 11 3810-4512 18 45 0 12 3810-5012 18 50 0 12 3810-4513 18 45 0 13 3810-5013 18 50 0 13 3810-4514 18 45 0 14 3810-5014 18 50 0 14 3810-4515 18 45 0 15 3810-5015 18 50 0 15 3810-4516 18 45 0 16 3810-5016 18 50 0 16 3816-4508 18 45 6 8 3816-5008 18 50 6 8 3816-4509 18 45 6 9 3816-5009 18 50 6 9 3816-4510 18 45 6 10 3816-5010 18 50 6 10 3816-4511 18 45 6 11 3816-5011 18 50 6 11 3816-4512 18 45 6 12 3816-5012 18 50 6 12 3816-4513 18 45 6 13 3816-5013 18 50 6 13 3816-4514 18 45 6 14 3816-5014 18 50 6 14 3816-4515 18 45 6 15 3816-5015 18 50 6 15 3816-4516 18 45 6 16 3816-5016 18 50 6 16 3830-4508 18 45 10 8 3830-5008 18 50 10 8 3830-4509 18 45 10 9 3830-5009 18 50 10 9 3830-4510 18 45 10 10 3830-5010 18 50 10 10 3830-4511 18 45 10 11 3830-5011 18 50 10 11 3830-4512 18 45 10 12 3830-5012 18 50 10 12 3830-4513 18 45 10 13 3830-5013 18 50 10 13 3830-4514 18 45 10 14 3830-5014 18 50 10 14 3830-4515 18 45 10 15 3830-5015 18 50 10 15 3830-4516 18 45 10 16 3830-5016 18 50 10 16 3832-4508 18 45 12 8 3832-5008 18 50 12 8 21 3832-4509 18 45 12 9 3832-5009 18 50 12 9 3832-4510 18 45 12 10 3832-5010 18 50 12 10 3832-4511 18 45 12 11 3832-5011 18 50 12 11 3832-4512 18 45 12 12 3832-5012 18 50 12 12 3832-4513 18 45 12 13 3832-5013 18 50 12 13 3832-4514 18 45 12 14 3832-5014 18 50 12 14 3832-4515 18 45 12 15 3832-5015 18 50 12 15 3832-4516 18 45 12 16 3832-5016 18 50 12 16 Dimension Dimension Part No. Suspected or documented allergy or intolerance to knowledgeable in the implants material and surgical composite materials, aspects and who has been instructed as to its mechanical 9. Patients with a known hereditary or acquired bone are interbody fusion devices intended for use as an aid in friability or calcification problem should not be considered spinal fixation. These devices must not be used for pediatric cases, angles designed to adapt to a variety of patient anatomies. Radiopaque markers have been use would be too large or too small to achieve a successful embedded within the implants, which are designed to allow result. Any case that requires the mixing of metals from two Surgical approach different components or systems. Any patient having inadequate tissue coverage over Cage System is to be implanted via posterior approach. Foreign body reaction to the implants including possible used with supplemental fixation. Patients should have at tumor formation, auto immune disease, and/ least six (6) months of non operative treatment prior to or scarring. Pregnancy, Neurovascular compromise including paralysis temporary 28 or permanent retrograde ejaculation in males, or other intermediary between the company and the patient, types of serious injury. Deep venous thrombosis, thrombophlebitis, and/or sale by or on the order of a physician. Urinary retention or loss of bladder control or other the surgeon is responsible for this choice which depends types of urological system compromise. Scar formation possibly causing neurological responsible for additional stresses and strains on the compromise or compression around nerves and/or pain. Fracture, microfracture, resorption, damage, or deformation or failure of the implants. The size and shape penetration of any spinal bone (including the sacrum, of the bone structures determine the size, shape and type pedicles, and/or vertebral body) and/or bone graft or bone of the implants. Once implanted, the implants are graft harvest site at, above, and/or below the level of subjected to stresses and strains. Herniated nucleus pulposus, disc disruption or surgeon at the time of the choice of the implant, during degeneration at, above, or below the level of surgery. Reproductive system compromise, including sterility, may cause fatigue or fracture or deformation of the loss of consortium, and sexual dysfunction. This may result in further side effects or embolism, atelectasis, bronchitis, pneumonia,etc. This fact is especially true in spinal surgery where issues of premature weight bearing, activity levels, and the other patient conditions may compromise the results. The surgeon must of this product without bone graft or in cases that do not warn the patient of the surgical risks and made aware of develop a union will not be successful. The surgeon must warn the operating procedures, including knowledge of surgical patient that the device cannot and does not replicate the techniques, good reduction, and correct selection and flexibility, strength, reliability or durability of normal healthy placement of the implants are important considerations in bone, that the implant can break or become damaged as a the successful utilization of the system by the surgeon. Patients who smoke involved in an occupation or activity which applies have been shown to have a reduced incidence of bone inordinate stress upon the implant (e. These patients should be advised of this fact and walking, running, lifting, or muscle strain) the surgeon must warned of this consequence. Obese, malnourished, and/ or advice the patient that resultant forces can cause failure of alcohol / drug abuse patients and those with poor muscle the device. Patients who smoke have been shown to have and bone quality and / or nerve paralysis are also poor an increased incidence of non-unions. In such cases, orthopaedic devices may be Patients with previous spinal surgery at the levels to be considered only as a delaying technique or to provide treated may have different clinical outcomes compared to temporary relief. Surgeons must instruct patients in detail about the decision by a physician to remove the device should take limitations of the implants, including, but not limited to , the into consideration such factors as: impact of excessive loading through patient weight or. The risk to the patient of the additional surgical procedure activity, and be taught to govern their activities accordingly. Migration of the implant, with subsequent pain and/or expected with a normal, healthy spine, and the patient neurological, articular or soft tissue lesions. Such completeness of the set and integrity of the components patients must be advised of this fact and warned of the and/or instruments. Those detailed instructions are provided in and the presence of any cracks, bending, bruising or the surgical technique brochure supplied by L&K Biomed. External support may be should be stored in a dry environment, protected from recommended by the physician from two to four months direct sunlight and at an ambient temperature in their postoperatively or until x-rays or other procedures confirm original packaging. So all implants used in surgery must be sterilized by the fusion mass in order to prevent placing excessive the hospital prior to use. Otherwise, Instruments are stress on the implants which may lead to fixation or implant supplied non-sterile and may be re-used. Trained must instruct patients to report any unusual changes of the personnel must perform cleaning and mechanical operative site to his/her physician. Patients with previous spinal surgery at the package, all instruments and implants must be level(s) to be treated may have different clinical outcomes disassembled (if applicable) and cleaned using neutral compared to those without a previous surgery. Use the neutral pH enzyme soaking solution that has Steam Gravity 270?F (132? C) (Dry time, been prepared. Use a soft-bristled brush to gently clean the device should be used to enclose the case or tray in order to (particular attention shall be given to crevices, lumens, maintain sterility. Lumens should be cleaned and details of sterilization have an importanteffect, for all with a long, narrow, soft-bristled brush. Note: the enzyme solution should be changed on a regular basis in order to ensure its effectiveness. Remove the device from the enzyme solution and rinse Any Health Care Professional (e. Thoroughly flush lumens, holes and identity, durability, reliability, safety, effectiveness and/or other difficult to reach areas. Prepare the neutral pH cleaning (detergent) solution and Further, if any of the implanted spinal system component(s) place in a sonication unit. Completely submerge device in cleaning solution and performance specifications or otherwise does not perform sonicate for 10 minutes, preferably at 45-50 kHz. Repeat Steps 5 and 6 with freshly prepared cleaning your name and address, the nature of the complaint and solution. These instruments should be cleaned following the manual cleaning procedure above. All implants and instruments used in surgery must be 1104-ho, 145, Gasandigital 1-ro, Geumcheon-gu, sterilized by the hospital prior to use. Richard Salib KeiperSpine Orthopedic Surgeon Institute for Low Back and Neck Care Panelist Dr. All content is for educational and discussion purposes only and is not considered to represent training certification. Disruptive Technology Platform - coflex Interlaminar Family of Products ? >100,000 implantations w/ > 15 Years Clinical & Commercial History ? World class clinical results ? 3 prospective randomized multi-center studies ? Uniquely differentiated mechanism of action compared to interspinous devices 2. No Me-Too Products ? Comprehensive portfolio of 1st or 2nd to market degenerative & scoliosis technologies ? coflex-F recently launched in U. Proven International Operations ? Profitable with market leadership in Germany ? Sold in > 45 different countries 5. Non-Fusion or Stabiliza9on for Stenosis Fusion versus non-fusion or stabilization-whats been the history of non-fusion stabilization Please discuss morbidity, indications, risk factors, point of service trends, and device related attributes which favor inpatient versus outpatient point of service. Non-Fusion or Stabilization Facet Joint Degeneration ? Damaged cartilage ? Synovitis/synovial cysts ? Osteophyte formations ? Subchondral bone cysts ? Capsule/ligament relaxation ? Subluxations Is stabilization needed Non-Fusion or Stabilization Question ? Focusing On Stenosis.
Discount fucidin 10gm with amex
The introduction or delivery for introduction into interstate commerce of a device that is not in compliance with its conditions of approval is a violation of law antibiotics for uti urinary tract infection buy cheap fucidin 10gm. If the final printed labeling is not identical, any changes from the final draft labeling should be highlighted and explained in the amendment. Subsequently Integra Template was approved for the repair of scar contractures when other therapies have failed or when donor sites for repair are not sufficient or desirable due to the physiological condition of the patient (P900033/S008). Integra Template will also be marketed as Integra Omnigraft Dermal Regeneration Matrix (Omnigraft), specifically for the indication in the treatment of partial and full-thickness neuropathic diabetic foot ulcers that are greater than six weeks in duration, with no capsule, tendon or bone exposed, when used in conjunction with standard diabetic ulcer care. The dermal replacement layer consists of a porous, three-dimensional matrix, comprised of bovine collagen and chondroitin-6-sulfate (C6S) that is designed with a controlled porosity and defined degradation rate. The temporary epidermal layer is made of a thin polysiloxane (silicone) layer to provide immediate wound coverage and control moisture loss from the wound. For diabetic foot ulcers that are non-responsive to conventional therapy, alternative practices include skin substitutes, cellular or tissue derived products, or surgical alternatives such as arterial bypass grafting where vascular supply is insufficient and skin grafts. The Integra product line is currently approved for marketing in the United States, European Union, Canada, Mexico, Argentina, Brazil, Colombia, Costa Rica, Peru, South Africa, Turkey, United Arab Emirates, Saudi Arabia, Israel, Egypt, Serbia, Jordan, Japan, New Zealand, Australia, and Singapore for use in partial and full thickness wounds and reconstructive surgery. For the specific adverse events that occurred in the clinical study, please see Section X below. Study Design Patients were enrolled and treated between April 1, 2010 and June 5, 2014. Subjects who met the entry criteria were enrolled in the two week Pre- Treatment Phase and followed while they received standard of care treatment (e. The primary safety endpoint was the incidence of adverse events recorded during the 16 week Treatment Phase and three monthly visits of the Follow-up Phase. The primary effectiveness endpoint was the percentage of subjects with complete closure of the study ulcer as assessed by the Investigator, during the Treatment Phase. Follow-up Schedule Prior to randomization, subjects entered a two week Screening/Run-in (Pre- Treatment) Phase during which subjects were treated with debridement and Standard of Care for diabetic foot ulcers. During the Treatment Phase, subjects were treated and evaluated weekly for up to 16 weeks or until the study ulcer completely healed. Four weeks after either the study ulcer was confirmed completely healed or the final Treatment Visit (week 16), subjects entered the 12-week Follow-up Phase. During the Follow-up Phase, subjects attended monthly visits for safety and effectiveness outcomes, such as ulcer recurrence, adverse events and a Quality of Life Questionnaire. Clinical Endpoints the primary safety objective was to evaluate Integra Template safety through weekly assessments during the 16 week Treatment Phase and monthly visits during the three month Follow-up Phase. Evaluations included both monitoring for adverse events and changes in serum chemistry parameters. The primary effectiveness endpoint was the percentage of subjects with complete wound closure as assessed by the Investigator during the 16 week Treatment Phase. In the primary effectiveness analysis, the Last Observation Carried Forward principle was used for post-baseline time points with missing assessments. All subjects that discontinued before 100% wound closure during the Treatment Phase were not replaced and were considered treatment failures for the primary and secondary endpoint evaluations. Covariate analyses in the Intent- to-Treat population assessed the correlation of factors on ulcer healing and the robustness of the primary analysis. The following additional effectiveness endpoints were evaluated during the Treatment Phase: 1) percentage of subjects with complete wound closure (assessed by computerized planimetry), 2) time to complete wound closure (assessed by the Investigator), 3) time to complete wound closure (assessed by computerized planimetry), 4) the rate of wound closure (assessed by computerized planimetry), 5) the incidence of study ulcer recurrence, determined during the Follow-up Phase, and 6) changes in the Quality of Life metrics, evaluated throughout the study. At the conclusion of the Treatment and Follow-Up Phases of the study, 106/154 (68. Study Population Demographics and Baseline Parameters the baseline demographics in the Integra and Control arms were comparable for all parameters including, but not limited to , severity and type of diabetes, gender, race, age, and ulcer size area (Table 2). The most common reasons for reapplications were non-adherence with fluid accumulation and infection. Subject compliance in ulcer offloading was assessed via subject diary review and subject interviews. In this analysis, high levels of overall subject offloading compliance were observed for both Integra. They are also listed in descending order according to their frequency in the Integra cohort. Patient Death ? Four Control subjects and zero Integra subjects died during the study. None of the subjects in this trial had the treatment discontinued or the trial terminated due to laboratory abnormalities. Changes in the serum chemistry that were deemed clinically significant by the Investigators were reported as adverse events. Effectiveness results Primary Effectiveness Endpoint the primary effectiveness endpoint was complete closure of the study ulcer, as assessed by the investigator, during the 16-week Treatment Phase. Secondary Effectiveness Outcomes Complete Wound Closure ? Computerized Planimetry ? During the Treatment Phase, 77/154 (50. Rate of Wound Size Reduction ? the rate of wound healing (% healed/week) or rate of wound size reduction was measured via planimetric assessment (during the Treatment Phase) and calculated with the following formula: Rate (% healed/week) = 7 * [(Baseline wound size) ? (Post-baseline wound size)] / [(Baseline wound size) * (days in clinical trial)] 2 2 the average wound size at baseline was 3. The rate of wound size reduction observed at the end of the Treatment Phase for Integra and Control subjects was 7. All analysis models for the primary and secondary endpoints were adjusted for the baseline wound size and the baseline age of ulcer. Non-Fenestrated Integra Template ? Fenestrating and meshing (at a 1:1 ratio) of Integra Template was permitted (at the discretion of the investigator) to allow for drainage in the presence of exudate or hematoma. Poolability of Sites ? Site poolability was assessed prior to pooling the data from the different investigational sites. The results of this analysis demonstrated that the effect of site was not statistically significant and the overall results for complete wound closure were not site-dependent. Subject Withdrawal from the Study ? the reasons for subject withdrawal/discontinuation from the Treatment, and Study. Table 5 ? Reasons for Subject Withdrawal from Treatment Phase Premature Integra Control Total Termination Reason N = 154 N = 153 N = 307 n (n/N %) n (n/N %) n (n/N %) Adverse Event 13 (8. Demographics of the Withdrawn Population were compared and no evidence of selection bias in subject withdrawal was observed. These analyses included comparisons of the following factors for Integra and Control cohorts who withdrew during the Treatment Phase: 1) baseline study ulcer size, 2) the mean wound size reduction during the two week Run-In period, 3) the proportion of plantar to dorsal wounds and 4) baseline ulcer severity. The average baseline ulcer duration of Control subjects who withdrew during the Treatment Phase was longer than Integra subjects. Based on the computerized planimetry assessment prior to subject withdrawal during the treatment phase, a majority of withdrawals were due to the lack of treatment effectiveness in both groups, and the observed higher percentage of withdrawal in the control group appeared to be a reflection of the inferior performance of the Control treatment as compared to the Integra treatment. Therefore, the loss of these subjects did not significantly alter the evaluation of device safety or effectiveness. The pivotal clinical study included 35 Principal Investigators and 80 Sub-Investigators at sites that randomized subjects. The information provided does not raise any questions about the reliability of the data. Integra Bilayer Matrix Wound Dressing (which has the same composition as Integra Template) was cleared on August 14, 2002 for the management of partial and full thickness wounds, pressure ulcers, venous ulcers, diabetic ulcers, chronic vascular ulcers, surgical wounds (donor sites / grafts, post-Mohs surgery, post-laser surgery, podiatric, wound dehiscence), trauma wounds (abrasions, lacerations. Integra Wound Matrix Dressing (which contains the same dermal layer, but not the silicone layer of Integra Template), was cleared on September 10, 2002 for the same indications as the Integra Bilayer Matrix Wound Dressing. The complaint was filed because a physician thought that the product could have caused the deficiency based on his research that bovine thrombin has been known to cause the deficiency. The submitted data provided a reasonable assurance that the device is effective for the treatment of partial and full-thickness neuropathic diabetic foot ulcers that are greater than six weeks in duration, with no capsule, tendon or bone exposed, when used in conjunction with standard diabetic ulcer care. The specific conclusions are: the study met the pre-specified primary effectiveness criterion of complete study ulcer closure, (as assessed by the investigator during the 16-week treatment period). Specifically, Integra Template was statistically superior in the: 1) percentage of subjects with complete study ulcer closure, as assessed by computerized planimetry. No significant differences between treatment groups were observed for General Health, Social Functioning, Role Emotional, Mental Health or Vitality Modules of this questionnaire. With the exception of baseline ulcer size and baseline ulcer age, no other study covariate. This observation is consistent with previous clinical studies of diabetic neuropathic foot ulcers. The submitted data provided a reasonable assurance that the device is safe for the treatment of partial and full- thickness neuropathic diabetic foot ulcers that are greater than six weeks in duration, with no capsule, tendon or bone exposed, when used in conjunction with standard diabetic ulcer care. The specific conclusions are: Safety assessments included clinical visits during the two week Pre-Treatment Phase, weekly assessments during the 16 week Treatment Phase, and monthly assessments during the three month Follow-up Phase.