
Cleocin
Buy cleocin 150mg visa
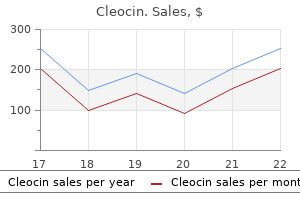
A weaker association was found between the concentrations of pentachlorophenol in urine and hexachloro benzene in serum acne 9gag cheap cleocin 150mg on-line, which was statistically significant only for men. These results suggested that formation of the cysteine conjugate is a quantitatively important meta bolic pathway in humans, especially in persons with high hexachlorobenzene body burdens. Moreover, pentachlorobenzenethiol is a urinary marker of the internal dose of hexachlorobenzene and of glutathione-mediated metabolism (To-Figueras et al. In rats fed hexachlorobenzene for 4 weeks, subsequent food deprivation appeared to enhance the toxic response (liver hypertrophy), implying decreased mobilization of hexachlorobenzene residues into fat and resulting in greater accumulation of hexachlorobenzene in plasma, liver, brain and adrenal glands (Villeneuve et al. In rhesus monkeys (Macaca mullata) given hexachlorobenzene at a dose of 8, 32, 64 or 128 mg/kg bw per day by gavage for 60 days, body fat and bone marrow had the highest concentrations, followed by adrenal glands, liver, kidney, brain, ovaries, muscle and serum. The serum concentrations did not appear to correspond to the dose (Knauf & Hobson, 1979). After administration of a single intravenous injection of hexachlorobenzene to male beagles, the chemical was initially found primarily in the lung (2 h) but after 8 h was found primarily in the fat. Excretion in these dogs occurred essentially through the bile and faeces, urinary excretion being of less importance (Sundlof et al. Absorption of hexachlorobenzene applied dermally to male Fischer 344 rats increased from 1% to 9. In adult female Sprague-Dawley rats dosed with 50 mg/kg bw hexachlorobenzene by gavage, the chemical was found to concentrate primarily in the fat and also in endocrine glands with large lipid components, such as the follicular fluid of the ovary and thyroid. The concentrations of residues of hexachlorobenzene in nine rats given 50 mg/kg bw per day were significantly (p < 0. The concentrations of residues of hexachlorobenzene in the ovary were greater than those in the thymus, liver or lung (Foster et al. Hexachlorobenzene was found in the milk of cows given the compound (Fries & Marrow, 1976) and in the organs of 18-day-old offspring of rat dams fed a diet containing hexachlorobenzene (Mendoza et al. Toxicokinetics demonstrated that hexachlorobenzene is transferred across the placenta and into breast milk in rodents (Courtney & Andrews, 1985; Courtney et al. A similar 6-day study of pregnant hamsters and guinea-pigs showed that the hamster fetuses had fivefold greater concentrations of hexachlorobenzene than the guinea-pig fetuses (Courtney et al. The distribution in infants showed concentration in fat, bone marrow and adrenal glands (Bailey et al. When pregnant Sprague Dawley rats were given a diet containing hexachlorobenzene during gestation and lactation (35 nmol/100 g diet [100 g/kg diet]), about 0. A large proportion of the hexachlorobenzene body burden was lost during lactation, and the concentration in the stomach contents of suckling pups was highest on day 2 after birth (Nakashima et al. The major urinary metabolites were pentachlorophenol, tetra chlorohydroquinone and pentachlorothiophenol. The other urinary metabolites were tetrachlorobenzene, pentachlorobenzene, 2, 4, 5 and 2, 4, 6-trichlorophenols and 2, 3, 4, 6 and 2, 3, 5-6-tetrachlorophenols; 2, 3, 4-trichlorophenol and other tetrachloro phenols were present in traces amounts. Examination of 1 g of liver tissue from adult female Wistar rats given 178 mol/kg bw [50. The authors hypothesized that the sulfur in the latter two compounds was derived from glutathione (Koss et al. Male and female Fischer 344 rats were dosed every other day for 103 days with 50 mol/kg bw [14. Urine was collected periodically and analysed for pentachlorophenol, 2, 3, 5, 6-tetrachlorobenzene-1, 4-diol and penta chlorothiophenol. The combined urinary excretion of these metabolites was greater in females than males, especially during the first 10 weeks. Pentachlorothiophenol was present at particularly high concentrations in the urine of females. The male:female ratios for pentachlorophenol and pentachlorothiophenol in bile were identical to those Figure 1. Excretion of metabolites by both males and females was stimulated by pretreatment with diethylstilbestrol. No sex differences in metabolism were observed in immature rats (Rizzardini & Smith, 1982). A study of the metabolism of hexachlorobenzene in isolated hepatocytes from male and female Fischer 344 adult rats showed that sex differences in metabolism did not explain the differences in porphyria development. The significant metabolites were pentachlorophenol, pentachlorothiophenol and tetrachloro-1, 4-benzenedithiol. Likewise, covalent binding of [14C]hexachlorobenzene to protein after incubation with hepatocytes could not account for the sex-dependent porphyrogenic activity (Stewart & Smith, 1987). Studies in vitro and analysis of tissues after administration of pentachloronitrobenzene in vivo showed that conjugation with glutathione and hydrolysis of the conjugates to yield free pentachlorothiophenol did not differ between males and females. These findings tend to reinforce the view that an active renal secretory mechanism, probably induced by estrogens during sexual maturation, is responsible for the highly efficient excretion of sulfur derivatives of hexachlorobenzene and pentachloronitrobenzene by female rats (To-Figueras et al. The metabolism of [14C]hexachlorobenzene was studied in microsomes derived from 12-week-old male Wistar rats. In addition, a considerable amount of covalent binding of radiolabel to protein was found: 11 pmol covalent binding per 4 mg microsomal protein in an incubation mixture containing 25 mol/L hexachlorobenzene. In order to establish the potential role of reductive dechlorination in the covalent binding, the anaerobic metabolism of hexachlorobenzene was investigated. Incubation at low oxygen concentrations indicated a relationship between covalent binding and micro somal oxidation of hexachlorobenzene. The finding of conversion-dependent covalent binding indicated that less than 10% of the covalent binding occurs during conversion of hexachlorobenzene to pentachlorophenol, and the remainder is produced during conversion of pentachlorophenol to tetrachlorohydroquinone, which is in redox equi librium with the corresponding semiquinone and quinone (chloranil). These results indicate the involvement of chloranil or the semiquinone radical in covalent binding during microsomal hexachlorobenzene metabolism (van Ommen et al. In rats given diets containing either hexachlorobenzene or its metabolite penta chlorobenzene for 13 weeks, both compounds were oxidized to pentachlorophenol and tetrachlorohydroquinone, which were the only two common metabolites excreted in urine. Male and female Sprague-Dawley rats were given five consecutive doses of 1 g/kg bw hexachlorobenzene by gavage over 2 days. The cumulative dose produced porphyria in female but not male rats after a delay of 6 weeks. The hepatic glutathione concentration showed a diurnal cycle in both male and female rats, which was more pronounced in males; the minimum concentration was observed 12 h after dosing. The glutathione concentration in hexachlorobenzene-treated male rats was significantly lower than that in controls at 6, 18 and 24 h, whereas no significant difference was observed in hexachlorobenzene treated female rats. Biliary excretion of a metabolite originating from glutathione conjugation of hexachlorobenzene was higher in male than in female rats. The exposure to hexachlorobenzene led to the development of bullae on sun-exposed areas, hyper pigmentation, hypertrichosis and porphyrinuria. Samples of breast milk from the mothers of these infants were shown to contain hexachlorobenzene (Peters et al. Follow up studies of 32 of the patients have shown that abnormal porphyrin metabolism and active symptomatology persisted 20 years after ingestion of hexachlorobenzene (Peters et al. After exposure beginning in childhood, small stature, small hands and painless arthritis were present. Of particular note, enlarged thyroids were present in 25% of men and 60% of women in comparison with 5% of unexposed persons from this region of Turkey. Two persons died of liver failure; one was a 27-year-old man and the other a 54-year-old woman during treatment for tuberculosis (Cripps et al.
Purchase cleocin paypal
Patient susceptibility to the specific toxin can vary skin care juarez order cheap cleocin line, and changes in mental status or cardiac and respiratory function. Gastrointestinal and clinical features may not correlate directly with the laboratory testing values. Compromise of renal, the clinical features can also be delayed up to 1 month after exposure to the liver, and cardiac function may also occur, depending on the severity and nature toxin. Differential Diagnosis: Sleep disorders related to the use of or withdrawal Course: the course is variable, depending on the chronicity and severity of from hypnotics or stimulants must be ruled out. In patients with symptoms of exposure to the toxin and whether consequent long-term abnormalities develop. Also, children are likely to ingest certain toxic substances and can be Diagnostic Criteria: Toxin-Induced Sleep Disorder (780. The complaint is temporally associated with the presence of an environ mental or ingested toxic agent. An increased sleep latency, reduced sleep efficiency, frequent awaken Sex Ratio: Not known. No mental or medical disorder, other than the one associated with the toxi Familial Pattern: None known. The symptoms do not meet the diagnostic criteria for any other sleep disor Pathology: Many changes can occur, depending on the specific toxin. Fatty degeneration of the heart, liver, and kidneys and bone-marrow depression may also occur with exposure to many organic toxins. Circadian Rhythm Sleep Disorders the circadian rhythm sleep disorders comprise a third section of dyssomnias and are grouped because they share a common underlying chronophysiologic basis. When internal factors, such as neurologic disease, or external factors, such as environmental or social circumstances, produce a circadian rhythm sleep disorder, diagnostic subtypes can be specified with the diagnosis of intrinsic type or extrin sic type, respectively. Three circadian rhythm sleep disorders have intrinsic and extrinsic subtypes: delayed sleep-phase syndrome, advanced sleep-phase syn drome, and non-24-hour sleep-wake disorder. In most circadian rhythm sleep disorders, the underlying problem is that the patient cannot sleep when sleep is desired, needed, or expected. As a result of sleep episodes occurring at inappropriate times, the corresponding wake periods may occur at undesired times. However, intermittent sleep episodes may occur in some disorders, including the irregular sleep-wake pattern. In the 1979 Diagnostic Classification of Sleep and Arousal Disorders, the sleep-wake schedule disorders were divided into two groups: transient and per sistent disorders. This subdivision has not been retained in the International Classification of Sleep Disorders because the duration of a disorder can now be specified and coded separately on axis A. For additional information on the chronophysiologic basis of this group of dis orders, the reader is referred to current texts on circadian rhythms, chronobiolo gy, and chronophysiology. If the cause of the altered sleep timing is another sleep ing of takeoff and arrival, and individual susceptibility. The sleep-wake distur disorder, sole diagnosis should be of the specific sleep disorder; diagnosis of the bances generally abate after two to three days in the arrival location. For example, are often associated with, but are not entirely dependent upon, sleep deprivation. Because the primary sleep diag ing of physiologic functions other than sleep and waking may take eight or more nosis is narcolepsy, however, the patient should not receive a second diagnosis of a days. Similarly, patients with mood performance impairment similar to those experienced by shift workers. Only the primary psychiatric diagnosis should be stated, Associated Features: Social or occupational dysfunction may occur, related to however, unless the sleep pattern is unrelated to the mental disorder or the mental decrements in daytime alertness and performance in the new time zone. Jet lag disorder is in remission and the sleep disorder is the predominant diagnosis. Only if the timing of sleep is the predom inal distention, dependent edema, and intermittent dizziness that can occur solely inant cause of the sleep disturbance and is outside the societal norm would a diag or largely as a function of airplane cabin conditions and are not truly symptoms nosis of a circadian rhythm sleep disorder be stated. If the setting of limits is a function of a caretaker, the sleep inconvenience, which, although sometimes severe, is self-limiting, with very few disorder is more appropriately diagnosed within the extrinsic subsection of the apparent symptoms by the third day after the flight. An alternating pattern of good and poor sleep may also occur for up to a Arousal Disorders. The Predisposing Factors: Reports are mainly anecdotal, but some experimental simpler term shift work sleep disorder is preferred to the previous longer and more evidence suggests that individuals over age 50 are more likely to suffer from jet cumbersome term, work shift change in conventional sleep-wake schedule. Neurotic extroverts have been found to phase adjust faster than neurotic introverts and, thus, would be expected to experience less jet lag. Synonyms and Key Words: Jet lag, transmeridian flight desynchronosis, air travel, transmeridian dyschronism. Time zone change (jet lag) syndrome consists of varying degrees of diffi culties in initiating or maintaining sleep, excessive sleepiness, decrements in Pathology: After rapid air travel across several time zones, the endogenous cir subjective daytime alertness and performance, and somatic symptoms cadian system remains aligned to the environmental time cues of the home time (largely related to gastrointestinal function) following rapid travel across zone. Because the adjustment process of the circadian system is slow, averaging multiple time zones. Altered appetite or gastrointestinal function toms can last for several days after the flight. An increase in the frequency of nocturnal awakenings to urinate the amount of jet lag experienced in homeward versus outward directions per se. General malaise Daytime symptoms are thought to be caused by (1) waking behaviors suddenly E. The symptoms do not meet criteria for any other sleep disorder producing which phase adjust more rapidly than others. Complications: Subjective distress about not sleeping well and social embar Minimal Criteria: A plus C. Self-treat ment, especially involving the use of large amounts of alcohol, may complicate Severity Criteria: the clinical picture. Menstrual irregularities in female air crew have been attrib uted to repeated jet lag, but clear and convincing data on this subject are lacking. Patients with bipolar (manic-depressive) disorder may experience an exacerba Moderate: Moderate insomnia or moderate excessive sleepiness, as defined on tion, with a higher likelihood of mania following eastward flights and depression page 23. Polysomnographic Features: In general, polysomnographic studies have Duration Criteria: shown a greater number of arousals and a greater percentage of stage 1 sleep dur Acute: 7 days or less. Subacute: More than 7 days but less than 3 months; symptoms are associated Sleep efficiency is consequently mildly reduced, usually no more than 10% from with more than one episode of time-zone change. Prolongation of sleep latency and reduction of slow-wave sleep occur Chronic: 3 months or longer; symptoms are associated with multiple episodes quite variably, the latter possibly more dependent on age than on the time zone of time-zone change. Most often, the second half of the sleep period is the more severely disrupted, whether the flight was eastbound or westbound. Bibliography: Other Laboratory Test Features: Actigraphy may demonstrate a disrupted Aschoff J, Hoffman K, Pohl H, Wever R. Re-entrainment of circadian rhythms after phase shifts of the sleep-wake pattern consistent with time zone (jet lag) syndrome. Desynchronization of body temperature and performance circadian rhythm as a result of outgoing and homecoming transmeridian flights. Differential Diagnosis: In most cases, the syndrome is self-limited and does Sasaki M, Endo S, Nakagawa S, Kitahara T, Mori A. A review of human physiological and performance excessive sleepiness, such as psychophysiologic insomnia or the obstructive sleep changes associated with desynchronosis of biological rhythms. The symptoms began within 1 or 2 days after air travel across at least two time zones. Decreased daytime performance schedule, acute-phase shift of sleep, frequently changing sleep-wake schedule. These figures, however, do not involve individuals with early morning work, which may Shift work sleep disorder consists of symptoms of insomnia or excessive comprise another group at risk.
150mg cleocin visa
Practice guideline for the treatment of patients with eating disorders acne vulgaris description buy discount cleocin on-line, third edition. Paciente pediatrico, con trastornos de la conducta alimentaria, obeso y geriatrico. Australian and New Zealand clinical practice guidelines for the treatment of anorexia nervosa. Epidemiology and risk factors of eating disorders: a two-stage epidemiologic study in a Spanish population aged 12-18 years. New contributions to the prevalence of eating disorders in Spanish adolescents: detection of false negatives. Prevalence of eating disorders among adolescent and young adult scholastic population in the region of Madrid (Spain). Estudio de prevalencia de trastornos de la conducta alimentaria en adolescentes de Zaragoza. Prevalencia de trastornos de la conducta alimentaria en las adolescentes navarras. Prevalencia de trastornos de la conducta alimentaria en la poblacion adolescente de la comarca de Osona [tesis doctoral]. Core interventions in the treatment and management of anorexia nervosa, bulimia nervosa and related eating disorders. Incidence, prevalence and mortality of anorexia nervosa and other eating disorders. Campana de informacion contra el abuso de laxantes y diureticos en la anorexia y la bulimia nerviosa. Los Trastornos de Conducta Alimentaria (Anorexia y Bulimia), un grave problema de nuestro tiempo [folleto informativo]. Melbourne, Victoria (Australia): the Royal Australian and New Zealand College of Psychiatrists; 2005. A critical examination of the amenorrhea and weight criteria for diagnosing anorexia nervosa. Blood levels of brain-derived neurotrophic factor correlate with several psychopathological symptoms in anorexia nervosa patients. Individual and family eating patterns during childhood and early adolescence: an analysis of associated eating disorder factors. Quality of rearing practices as predictor of short-term outcome in adolescent anorexia nervosa. A controlled family study of anorexia nervosa and bulimia nervosa: psychiatric disorders in first-degree relatives and effects of proband comorbidity. Controlled family study of anorexia nervosa and bulimia nervosa: evidence of shared liability and transmission of partial syndromes. Alteraciones alimentarias en ninos y adolescentes argentinos que concurren al consultorio del pediatra. Micali N, Holliday J, Karwautz A, Haidvogl M, Wagner G, Fernandez-Aranda F, et al. Childhood eating and weight in eating disorders: a multi-centre European study of affected women and their unaffected sisters. Assessment of sociocultural influences on the aesthetic body shape model in anorexia nervosa. Comparison of personality risk factors in bulimia nervosa and pathological gambling. Childhood obsessive-compulsive personality traits in adult women with eating disorders: defining a broader eating disorder phenotype. Features of childhood sexual abuse and the development of psychiatric and substance use disorders. Coming to terms with risk factors for eating disorders: application of risk terminology and suggestions for a general taxonomy. Anorexia nervosa and major depression: shared genetic and environmental risk factors. The relation among perfectionism, obsessive-compulsive personality disorder and obsessive-compulsive disorder in individuals with eating disorders. Impulsivity in women with eating disorders: problem of response inhibition, planning, or attention Relationship of weight and eating disorders in type 2 diabetic patients: a multicenter study. Disordered eating behaviour and microvascular complications in young women with insulin-dependent diabetes mellitus. Lamerz A, Kuepper-Nybelen J, Bruning N, Wehle C, Trost-Brinkhues G, Brenner H, et al. Prevalence of obesity, binge eating, and night eating in a cross-sectional field survey of 6-year-old children and their parents in a German urban population. Health and sociodemographic factors associated with body weight and weight objectives for women. Evidence of diffuse atrophy of the thyroid gland in patients with anorexia nervosa. Prevencion de trastornos del comportamiento alimentario con un programa multimedia. Internet-based innovations for the prevention of eating disorders: a systematic review. A meta-analytic review of eating disorder prevention programmes: encouraging findings. Randomized, controlled trial of an internet-facilitated intervention for reducing binge eating and overweight in adolescents. Reducing maladaptive weight management practices: developing a psychoeducational intervention program. Impact of interactive school-based media literacy lessons for reducing internalization of media ideals in young adolescent girls and boys. Definition and outcome of a curriculum to prevent disordered eating and body-shaping drug use. Dissonance and healthy weight eating disorder prevention programmes: long-term effects from a randomized efficacy trial. Internet-delivered targeted group intervention for body dissatisfaction and disordered eating in adolescent girls: a randomized controlled trial. Guia clinica para la atencion a los trastornos de la conducta alimentaria en el Area 3 de Madrid. Development and validation of the Eating Disorder Diagnostic Scale: a brief self-report measure of anorexia, bulimia, and binge-eating disorder. Discriminant validity of the Eating Attitudes Test according to American Psychiatric Association and World Health Organization criteria of eating disorders. De Irala J, Cano-Prous A, Lahortiga-Ramos F, Gual-Garcia P, Martinez-Gonzalez M, Cervera Enguix S. Prevalencia de casos clinicos de trastornos del comportamiento alimentario en mujeres adolescentes de la Comunidad de Madrid. Cross-cultural assessment of eating disorders: psychometric properties of a Spanish version of the Bulimia Test-Revised. Prevalencia de los trastornos de la conducta alimentaria: consideraciones metodologicas. The eating disorder examination: a semi structured interview for the assessment of the specific psychopathology of eating disorders. Reliability and validity of the child version of the Eating Disorder Examination: a preliminary investigation. Tratamientos psicologicos eficaces para trastornos del comportamiento alimentario. Atencion primaria y trastornos de la alimentacion: nuestra actitud frente a ellos (I). A randomized trial on the efficacy of a 2 month tube feeding regimen in anorexia nervosa: A 1-year follow-up study.

Buy cleocin 150mg cheap
Children and young of privacy acne natural treatment 150mg cleocin amex, the fair use of data and the people in their bedrooms can be exposed concerns of parents. Software do a better job of holding these companies such as Snapchat has even been designed to account; we need to demand that our to limit the readability of shared content by children be protected. We have more work making it unavailable after a user-determined to do in designing and building ethical, time selection. WhatsApp, Signal and responsible and trustworthy technologies others offer encrypted communication for children. Many parents also struggle with conficting messages that they should limit screen time, on the one hand, or get the latest device so their children can keep up, on the other. So the task is to fnd ways to provide children with the support and guidance they need to make the most of their online experiences. They also worried that books and the printing press would lead to what today As seen in previous chapters, whether we would call information overload. Their use by children is harder loneliness, stress, depression or problems to monitor. Conversely, children who beneft from digital devices gather information on them, too. For example, a report from the high-connectivity contexts fnd it diffcult to Swedish Media Council described how estimate how much time they spend with parents in Sweden were at once quite digital technology, because they are more positive about the benefts their children or less using it all of the time. Some experts say children still interact with one another as much as before and that the interactions A new generation gap are of similar quality. It is the venues for social interaction that have changed Parents, educators and those with to digital. More attention should be given to what Adults who think children spend too Connected children point out that adults children are doing much time engaging with screens are the ones missing out, as one girl online and why. I can share with her each moment that connected the same room without saying a single word she or I live every day. We talk with family members by allowing them all the time through Skype and I never felt that to connect, communicate and share he left home. Therefore, solutions to support families devices and not spending enough time I fnd it diffcult to understand how my in making effective use on school studies. Many parents and caregivers experiencing a range of appropriate, do not have the time, knowledge or informative and entertaining content. European countries, parents seemed to adapt their style from a more restrictive To whom do children turn when they strategy with younger children to a more encounter problems online A study show that children tend to frst turn involving children between the ages of 7 to other children to talk about their and 18 in Bahrain found that restrictions online experiences. As a result, appropriate behaviour and provision School of Economics and many parents are restrictive in managing and protection have a positive effect Political Science. The evidence thought to be more valuable, such as summarized here looks at screen time and face-to-face socializing, reading books or its impact on mental well-being, social exercising. One reason for this shift is the growing recognition that digital While parents and caregivers may think they technologies offer many opportunities for are protecting their children by restricting the children to pursue developmentally valuable time spent on digital technology, this may activities, and these opportunities are both not be the case. She realized Alexa Rachel Botsman could tell jokes, do maths or give interesting For generations, our trust in technology has facts. Looking a little happens if I, say, step into an autonomous sheepish, she asked me if it was okay to be car Did she think it had feelings or decide whether to go left or right, to swerve even deserved respect The next generation will grow up in an age this simple experiment is a telling illustration of autonomous agents making decisions in of a profound technological shift.
Buy generic cleocin 150mg on-line
Veterans 65 years and older comprise 70% of those with diabetes skin carecom order cleocin 150 mg fast delivery, reflecting the older age distribution of this population. Standards of care are determined on the basis of all clinical data available for an individual patient and are subject to change as scientific knowledge and technology advance and patterns evolve. The Champions and the Work Group also provided direction on inclusion and exclusion criteria for the evidence review and assessed the level and quality of the evidence. The specialties and clinical areas of interest included endocrinology, internal medicine, nutrition, pharmacy, health education, nursing, medical management, ambulatory care, and family practice. A strong recommendation indicates that the Work Group is highly confident that desirable outcomes outweigh undesirable outcomes. If the Work Group is less confident of the balance between desirable and undesirable outcomes, they give a weak recommendation. Thus, differences in recommendations across guidelines may reflect differences in the grading system used as well as differences in the evidence reviewed and/or how the strength of the evidence is evaluated by the Work Group. Additional information regarding these categories and their definitions can be found in Appendix A. The categories for the recommendations included in the 2017 version of the guideline can be found in the section on Recommendations. In order to report the strength of all recommendations using a consistent format. The process for developing the initial draft is described in more detail in Drafting and Submitting the Final Clinical Practice Guideline. Once a near-final draft of the guideline was agreed upon by the Champions and Work Group members, the draft was sent out for peer review and comment. For transparency, all reviewer feedback was posted in tabular form on the wiki site, along with the name of the reviewer. All feedback from the peer reviewers was discussed and considered by the Work Group. Summary of Patient Focus Group Methods and Findings When forming guideline recommendations, consideration should be given to the values of those most affected by the recommendations. It is important to note the focus group was a convenience sample and the Working Group recognizes the limitations inherent in the small sample size. Less than 10 people were included in the focus group consistent with the requirements of the federal Paperwork Reduction Act, 1980. Thus, the Working Group made decisions regarding the priority of topics to discuss at the focus group. These limitations, as well as others, were considered throughout the use of the information collected from the discussion for guideline development. The following concepts are aspects of care that are important to patients that emerged from the discussion. Additional details regarding the patient focus group methods and findings can be found in Appendix D. Using shared decision-making, consider all treatment options and develop a treatment plan based on the balance of risks, benefits, and patient-specific goals, values, and preferences. A structured algorithm accompanies the guideline to provide an overview of the recommendations in the context of the flow of patient care and clinician decision making and to assist with training providers. The algorithm may be used to help facilitate translation of guideline recommendations into effective practice. Clinicians must be skilled at presenting their patients with understandable and actionable information regarding both individual treatments and levels and locations of care. Use of an empathetic and non-judgmental (versus a confrontational) approach facilitates discussions sensitive to gender, culture, and ethnic differences. The information that patients are given about treatment and care should be culturally appropriate and also available to people with limited literacy skills. It should also be accessible to people with additional needs such as physical, sensory, or learning disabilities. Family involvement should be considered if appropriate, especially in elderly patients. Lastly, they should involve the patient in prioritizing problems to be addressed and in setting specific goals regardless of the selected setting or level of care. The algorithm serves as a tool to prompt providers to consider key decision points in the course of an episode of care. The use of the algorithm format as a way to represent patient management was chosen based on the understanding that such a format may promote more efficient diagnostic and therapeutic decision making and has the potential to change patterns of resource use. Standardized symbols are used to display each step in the algorithm and arrows connect the numbered boxes indicating the order in which the steps should be followed. We recommend shared decision-making to enhance patient knowledge Strong for Reviewed, and satisfaction. We recommend that all patients with diabetes should be offered ongoing Strong for Reviewed, individualized diabetes self-management education via various modalities New-replaced tailored to their preferences, learning needs and abilities based on available resources. We suggest offering one or more types of bidirectional telehealth Weak for Reviewed, interventions (typically health communication via computer, telephone or New-replaced other electronic means) involving licensed independent practitioners to patients selected by their primary care provider as an adjunct to usual patient care. We recommend setting an HbA1c target range based on absolute risk Strong for Reviewed, reduction of significant microvascular complications, life expectancy, New-added patient preferences and social determinants of health. We recommend assessing patient characteristics such as race, ethnicity, Strong for Reviewed, chronic kidney disease, and non-glycemic factors. We recommend an individualized target range for HbA1c taking into Strong for Reviewed, account individual preferences, presence or absence of microvascular New-replaced complications, and presence or severity of comorbid conditions (See Table 2). We recommend that in patients with type 2 diabetes, a range of HbA1c Strong for Reviewed, 7. We suggest that providers be aware that HbA1c variability is a risk factor Weak for Reviewed, for microvascular and macrovascular outcomes. We recommend a nutrition intervention strategy reducing percent of energy Strong for Reviewed, from carbohydrate to 14-45% per day and/or foods with lower glycemic New-added index in patients with type 2 diabetes who do not choose the Mediterranean diet. We recommend against targeting blood glucose levels <110 mg/dL for all Strong Reviewed, hospitalized patients with type 2 diabetes receiving insulin. We recommend insulin be adjusted to maintain a blood glucose level Strong for Reviewed, between 110 and 180 mg/dL for patients with type 2 diabetes in critically Amended ill patients or those with acute myocardial infarction. We recommend against the use of split mixed insulin regimen for all Strong Reviewed, hospitalized patients with type 2 diabetes. We suggest a regimen including basal insulin and short-acting meal time or Weak for Reviewed, basal insulin and correction insulin for non-critically ill hospitalized New-added patients with type 2 diabetes. We suggest providing medication education and diabetes survival skills to Weak for Reviewed, patients before hospital discharge. We recommend performing a comprehensive foot risk assessment Strong for Not Reviewed, annually. We recommend referring patients with limb-threatening conditions to the Strong for Not Reviewed, appropriate level of care for evaluation and treatment. We suggest screening for retinopathy at least every other year (biennial Weak for Not Reviewed, screening) for patients who have had no retinopathy on all previous Amended examinations. We recommend that all females with pre-existing diabetes or personal Strong for Not Reviewed, history of diabetes and who are of reproductive potential be provided Amended contraceptive options education and education on the benefit of optimizing their glycemic control prior to attempting to conceive. We recommend that all females with pre-existing diabetes or personal Strong for Not Reviewed, history of diabetes who are planning pregnancy be educated about the Amended safest options of diabetes management during the pregnancy and referred to a maternal fetal medicine provider (when available) before, or as early as possible, once pregnancy is confirmed. We recommend shared decision-making to enhance patient knowledge and satisfaction. Key principles include the patient/family readiness, provision of benefits and harms of all options in understandable tools, and incorporation of preferences. This should include, at a minimum, diagnosis, difficulties in management, and times of transition or development of complications.
Order 150 mg cleocin otc
Physiologically neuromyotonia is characterized by continuous motor unit and muscle bre activity which is due to peripheral nerve hyperexcitability; it is abolished by curare (cf skin care for eczema 150 mg cleocin overnight delivery. Neuromyotonia may be associated with autoantibodies directed against presynaptic voltage-gated K+ channels. Around 20% of patients have an 239 N Neuronopathy underlying small cell lung cancer or thymoma, suggesting a paraneoplastic aeti ology in these patients. Neuromyotonia has also been associated with mutations within the voltage-gated K+ ion channel gene. Neuromyotonia usually improves with symptomatic treatments such as car bamazepine, phenytoin, lamotrigine, and sodium valproate, in combination if necessary. Paraneoplastic neuromyotonia often improves and may remit after treatment of the underlying tumour. Cross References Fasciculation; Myokymia; Myotonia; Paramyotonia; Pseudomyotonia; Stiffness Neuronopathy Neuronopathies are disorders affecting neuronal cell bodies in the ventral (ante rior) horns of the spinal cord or dorsal root ganglia, hence motor and sensory neuronopathies, respectively. Cross Reference Neuropathy Neuropathy Neuropathies are disorders of peripheral nerves. These clinical patterns may need to be differentiated in practice from disor ders affecting the neuronal cell bodies in the ventral (anterior) horns of the spinal cord or dorsal root ganglia (motor and sensory neuronopathies, respectively); and disorders of the nerve roots (radiculopathy) and plexuses (plexopathy). Clinical signs resulting from neuropathies are of lower motor neurone type (wasting, weakness, reex diminution, or loss). Mononeuropathies often result from local compression (entrapment neuropathy), trauma, or diabetes. Polyneuropathies may have genetic, infective, inammatory, toxic, nutritional, and endocrine aetiologies. Many neuropathies, particularly polyneuropathies in the elderly, remain idiopathic or cryptogenic, despite intensive investigation. If these other signs are absent, then isolated nuchal rigidity may suggest a foraminal pressure cone. It may also occur in syndromes causing predominantly axial (as opposed to limb) rigidity. This nuchocephalic 241 N Nyctalopia reex is present in infants and children up to the age of about 4 years. Beyond this age the reex is inhibited, such that the head is actively turned in the direction of shoulder movement after a time lag of about half a second. Cross References Age-related signs; Primitive reexes Nyctalopia Nyctalopia, or night blindness, is an impairment of visual acuity specic to scotopic vision, implying a loss or impairment of rod photoreceptor function. Patients may spontaneously complain of a disparity between daytime and noc turnal vision, in which case acuity should be measured in different ambient illumination. The nature of the nystagmus may permit inferences about the pre cise location of pathology. Observations should be made in the nine cardinal positions of gaze for direction, amplitude, and beat frequency of nystagmus. However, since it is the slow phase which is pathological, it is more elo quent concerning anatomical substrate. The intensity of jerk nystagmus may be classied by a scale of three degrees: 1st degree: present when looking in the direction of the fast phase; 2nd degree: present in the neutral position; 3rd degree: present when looking in the direction of the slow phase. Pendular or undulatory nystagmus: In which the movements of the eyes are more or less equal in ampli tude and velocity (sinusoidal oscillations) about a central (null) point. This is often congenital, may be conjugate or disconjugate (sometimes monocular), but is not related to concurrent internuclear ophthalmo plegia or asymmetry of visual acuity. A slow phase with exponentially increasing veloc ity (high-gain instability, runaway movements) may be seen in congenital or acquired pendular nystagmus. The pathophysiology of acquired pendular nys tagmus is thought to be deafferentation of the inferior olive by lesions of the red nucleus, central tegmental tract, or medial vestibular nucleus. Central vestibular: unidirectional or multidirectional, 1st, 2nd or 3rd degree; typically sustained and persistent. Cerebellar/brainstem: commonly gaze-evoked due to a failure of gaze-holding mechanisms. Congenital: usually horizontal, pendular-type nystagmus; worse with xation, attention, and anxiety. Many pathologies may cause nystagmus, the most common being demyelina tion, vascular disease, tumour, neurodegenerative disorders of cerebellum and/or brainstem, metabolic causes. Pendular nystagmus may respond to anticholinesterases, consistent with its being a result of cholinergic dysfunction. Periodic alternating nystagmus responds to baclofen, hence the importance of making this diagnosis. These symp toms are thought to reect critical compromise of optic nerve head perfusion and are invariably associated with the nding of papilloedema. Obscurations mandate urgent investigation and treatment to prevent permanent visual loss. Cross Reference Papilloedema Obtundation Obtundation is a state of altered consciousness characterized by reduced alert ness and a lessened interest in the environment, sometimes described as psy chomotor retardation or torpor. An increased proportion of time is spent asleep and the patient is drowsy when awake. Cross References Coma; Psychomotor retardation; Stupor Ocular Apraxia Ocular apraxia (ocular motor apraxia) is a disorder of voluntary saccade initia tion; reexive saccades and spontaneous eye movements are preserved. Ocular apraxia may be overcome by using dynamic head thrusting, with or without blinking (to suppress vestibulo-ocular reexes): the desired xation point is achieved through reex contraversive tonic eye movements to the midposition following the overshoot of the eyes caused by the head thrust. Cross References Apraxia; Saccades Ocular Bobbing Ocular bobbing refers to intermittent abnormal vertical eye movements, usu ally conjugate, consisting of a fast downward movement followed by a slow return to the initial horizontal eye position. The sign has no precise localizing value, but is most commonly associated with intrinsic pontine lesions. Its patho physiology is uncertain but may involve mesencephalic and medullary burst neurone centres. Cross Reference Ocular dipping Ocular Dipping Ocular dipping, or inverse ocular bobbing, consists of a slow spontaneous down ward eye movement with a fast return to the midposition. This may be observed in anoxic coma or following prolonged status epilepticus and is thought to be a marker of diffuse, rather than focal, brain damage. Reverse ocular dipping (slow upward ocular bobbing) consists of a slow upward movement followed by a fast return to the midposition. Cross Reference Ocular bobbing Ocular Flutter Ocular utter is an eye movement disorder characterized by involuntary bursts of back-to-back horizontal saccades without an intersaccadic interval (cf. Ocular utter associated with a localized lesion in the paramedian pontine reticular formation. It has occasionally been reported with cerebellar lesions and may be under inhibitory cerebellar control.
Purchase cleocin with amex
Disorder of memory includes the hip pocampal defects of diminished storage and accelerated forgetting; deja vu and jamais vu also occur skin care facts purchase cleocin on line amex, as described above. There may be altered states of consciousness such as a fugue, with impaired registration. Panoramic recall, in which the patient may feel that he is rapidly re-enacting long periods of his life, is also described. Affective Disorder of Memory Memory is not only disturbed by organic damage to the brain itself; it is also affected by emotion. This is certainly true of normal, healthy people, in whom the affective state strongly infuences the processes of remembering and forgetting. It is also true of those with affective and schizo phrenic psychoses, and of neuroses and personality disorders. There is also substantial evidence of an association between depression and generic memory impairment. It is thought that mood disorder, such as depression, reduces the amount of cognitive processing resources available for a given task, and in the memory domain this is manifest as defcits in the elaboration, organization, encoding and retrieval of material into and out of memory (Dalgleish and Cox, 2002). This mood-congruent memory effect is similar but distinct from state-dependent memory, which refers to the memory bias for material that is learned in a particular mood and is more easily retrieved if the individual is in that same mood during retrieval. Rates of forgetting are infuenced by the personal meaningfulness of the information, the conceptual style of the individual, the degree of processing and elaboration of the information and age. It is likely that normal forgetting is determined by disuse or interference by more recently learned or more vivid material and underpinned by physiological or metabolic processes (Lezak et al. In proac tive interference, newly learned material interferes with the recall of previously learned material. In retroactive interference, previously learned material interferes with the recall of newly learned material (see Eysenck and Keane, 2010 for a fuller discussion). The process of repression or selective forgetting, however, suggests that forgetting is not simply down to errors in the fling and retrieval mechanism. Forgetting is subject to the infuence of affect: which sensations are registered, what is retained and for how long and what information is available for recall. Other forms of active forgetting exist, including motivated forgetting which subsumes repression as an example, and also the deliberate forgetting of where we put our glasses yesterday when we are looking for them today! Directed forgetting is the term for the process by which we actively use executive control proc esses within the prefrontal cortex to forget items that we do not wish to recall. It is obvious from the foregoing that forgetting is an important and normative process. Questions are answered with fuency, and the story appears to be believed implicitly by the pseudologic himself. This usually occurs with an associated personality disorder of histri onic or dissocial type, and often when the individual is experiencing a major life crisis such as facing criminal proceedings. The picture is of a very isolated person, without family or friends, drifting into the accident and emergency department of a large hospital in a strange city late at night, with stories of his own exploits and importance and the unfortunate vicissitudes he has experienced. With personality disorders and also with affective disorders, especially at times of heightened emotion, memory is falsifed and distorted, and events and circumstances are misrepresented. So the grandiose delusions and memory disturbance of general paresis may result in falsifcation and distortion of events remembered. Similarly, confabu lation as in the Korsakov state is associated with falsifcation. This was stated by a patient who had quite suddenly come to believe that all her actions were being observed and, subsequently, her behaviour controlled. This is a backdating of delusion to a time before the patient was ill, based on an admixture of remembered true events and delu sional elaboration of the meaning of those events. This has been described by some authorities as a form of confabulation (Nathaniel-James and Frith, 1996; McKenna et al. In the original study, when subjects were presented with narratives and asked to recall them, con fabulation was defned as recall of information not present in the original narrative. The degree of confabulation was related to problems in suppressing inappropriate responses and formal thought disorder. It is clear that it is very uncommon in a spontane ous form, and when it does occur it always seems to take the form of so-called fantastic confabu lation Simple, momentary, or provoked confabulations, on the other hand, appear to be commonplace. As well as occurring in the normal state and in personality disorders, it is a prominent feature of affective disturbances. Memory itself was accurate, but on remonstrating on any particular point of fact, further depressive explanations of events would be given. For instance, the marriage licence was described as a forgery, and com plicated legal explanations were given as to why the house did not belong to her and her husband. In mania, unacceptable events or opinions may be brushed aside as not having occurred and unrealistic goals pursued as though there were nothing to prevent their attainment. A person makes a witty remark, or writes a haunting melody, without realizing that he is quoting (plagiarizing) rather than producing something original. The process is seen when words or phrases come into popular usage for a few months or years by some process of mass spread, in which people using the expression believe they are introducing a new idea. This is a defect of recall that can be seen as a successful defence mechanism; it helps to maintain the integrity of the person. However, in the affect of hope lessness, reactivation of memories of previous failures is a frequent reason for perpetuating neurotic thinking and behaviour (Engel, 1968). Psychogenic amnesia may appear without any organic disease being present, but the presentation of organic brain disease is always modifed by psy chogenic factors (Pratt, 1977). Misnaming objects and momentary loss of memory for words in healthy subjects may result from faulty retrieval from short and long-term memory stores rather than from the psychoana lytic explanation of repression. Such errors may be categorized as acoustic or semantic; acoustic errors tending to occur in short-term stores of up to 30 seconds and semantic ones in long-term stores after more than fve minutes (Shallice and McGill, 1977). Dissociative (Hysterical) Fugue the symptoms pertaining to dissociative (conversion) disorders (hysteria) in the International Classifcation of Diseases (World Health Organization, 1992) are of two types: conversion and dissociation. In dissociation, there is a narrowing of the feld of consciousness, with subsequent amnesia for the episode. The person appears to be in good contact with his environment and usually behaves appropriately, maintaining basic self-care, although he sometimes displays disinhibition. The duration of the episode can be very variable, from a few hours to several weeks, and the subject may travel considerable distances. As he walked about the streets, he found he was near an airport terminal and, to his surprise, he discovered that he was in Montreal. Germane to his adventure was the history of a catastrophic row and the breakdown of his marriage just before he took off. Thus the features of dissociative fugue are dissociative amnesia, purposeful travel beyond the usual everyday range and maintenance of basic self-care (World Health Organization, 1992). The Ganser state is very rarely seen in English prisons but, when it does occur, it is more likely in those awaiting trial than those already sentenced (Enoch, 1990). There has been considerable argument as to whether this condition is primarily hysterical or an organic psychosis, with different authors supporting each contention (Latcham et al.
Purchase cleocin without prescription
The association of occupational exposure to extremely low frequency electromagnetic fields and the risk of neurodegenerative diseases skin care quiz products discount 150 mg cleocin visa. Maternal cell phone use during pregnancy and child cognition at age 5 years in 3 birth cohorts. Cell phone exposures and hearing loss in children in the Danish National Birth Cohort. Radiofrequency hyperthermia in the palliative treatment of mucinous carcinomatosis of appendiceal origin: optimizing and monitoring heat delivery in western patients. The influence of repetitive delivery of radiofrequency current in catheter ablation. Treatment of striae distensae combined enhanced penetration platelet-rich plasma and ultrasound after plasma fractional radiofrequency. Mobile phone signal exposure triggers a hormesis-like effect in Atm+/+ and Atm-/ mouse embryonic fibroblasts. Ataxia telangiectasia mutated deficiency does not result in genetic susceptibility to 50Hz magnetic fields exposure in mouse embryonic fibroblasts. Electromagnetic field exposure and male breast cancer risk: a meta-analysis of 18 studies. Effects of 50-Hz magnetic field exposure on hormone secretion and apoptosis-related gene expression in human first trimester villous trophoblasts in vitro. Superposition of noise magnetic fields inhibits clustering of fibroblast membrane surface receptors induced by 50 Hz magnetic fields in Chinese hamster lungs. Lipidomic alteration and stress defense mechanism of soil nematode Caenorhabditis elegans in response to extremely low-frequency electromagnetic field exposure. Measurements of the ripple effect and geometric distribution of switched gradient fields inside a magnetic resonance scanner. The influences of extremely low frequency magnetic fields on drug-induced convulsion in mouse. A review on the reproductive health of males exposed to radiation by shipping radar microwave. Low-frequency pulsed electromagnetic field therapy in fibromyalgia: a randomized, double-blind, sham controlled clinical study. Biologic effects and hygienic regulation of electromagnetic fields caused by mobile communication devices. Clinical observation over health state in area subjected to radio frequency electromagnetic fields. Clinical monitoring in areas of exposure to radiofrequency electromagnetic fields. Systematic analysis of the state of man exposed to radio wave irradiation for a long time. Exposure to magnetic fields and survival after diagnosis of childhood leukemia: a German cohort study. Possible mechanisms by which electric fields from power lines might affect airborne particles harmful to health. Comment on the papers: increased exposure to pollutant aerosols under high voltage power lines; and Corona ions from powerlines and increased exposure to pollutant aerosols. Biophysical mechanisms: a component in the weight of evidence for health effects of power-frequency electric and magnetic fields. Childhood cancer in relation to distance from high-voltage power lines in England and Wales: a case-control study. Journal of radiological protection: official journal of the Society for Radiological Protection. Percutaneous Microwave Tumor Ablation Is Safe in Patients with Cardiovascular Implantable Electronic Devices: A Single-Institutional Retrospective Review. Armrests and back support reduced biomechanical loading in the neck and upper extremities during mobile phone use. Vibratory sample magnetometry of middle ear prostheses and manufacturing materials. Biological effects of the action of permanent magnetic fields of various intensities. State of peripheral blood of technical personnel exposed to constant magnetic fields. Occupational 50 Hz magnetic field exposure measurements among female sewing machine operators in Hungary. Occupational exposure to electromagnetic fields and its health effects in electric energy workers. Stress-related endocrinological and psychopathological effects of short and long-term 50Hz electromagnetic field exposure in rats. Recent concept of protection of workers and general population against electromagnetic fields in the European countries. Risk of neoplastic diseases in conditions of exposure to power magnetic fields-epidemiologic investigations. Risk of neoplastic diseases in conditions of exposure to radio and microwave fields-epidemiologic investigations. Duration of conscious reactions in persons exposed to an electric field of 50 Hz frequency. Evaluation of reports on environmental measurements of electromagnetic fields generated by high voltage transmission lines and substations. Practical aspects of taking measurements of electromagnetic fields in the surrounding of overhead transmission lines. Role of Electromagnetic Field Exposure in Childhood Acute Lymphoblastic Leukemia and No Impact of Urinary Alpha Amylase-a Case Control Study in Tehran, Iran. Return to work of a pacemaker bearing worker: the relationship between health problems and electromagnetic interferences. Lack of adverse effects of whole-body exposure to a mobile telecommunication electromagnetic field on the rat fetus. Radio-frequency energy delivery to the anal canal for the treatment of fecal incontinence. A study on the relationship between subjective unpleasantness and body surface vibrations induced by high level low-frequency pure tones. Mobile phone use, exposure to radiofrequency electromagnetic field, and brain tumour: a case-control study. Evidence for the initiation of decompression sickness by exposure to intense underwater sound. Advance of research on effect of extremely low frequency exposure in pregnant period on pregnancy. Do mobile telephones have adverse effects on the functions of implantable cardioverter defibrillators Determinants of gradient field-induced current in a pacemaker lead system in a magnetic resonance imaging environment. Five-year experience with radiofrequency catheter ablation: implications for management of arrhythmias in pediatric and young adult patients. Prediction and measurement of the electromagnetic environment of high-power medium-wave and short-wave broadcast antennas in far field. Tanvir S, Thuroczy G, Selmaoui B, Silva Pires Antonietti V, Sonnet P, Arnaud Cormos D, et al. Effects of 3G cell phone exposure on the structure and function of the human cytochrome P450 reductase. Magnetic field effects on coenzyme B12-dependent enzymes: validation of ethanolamine ammonia lyase results and extension to human methylmalonyl CoA mutase. Impact of selected magnetic fields on the therapeutic effect in patients with lumbar discopathy: A prospective, randomized, single-blinded, and placebo-controlled clinical trial. Advances in clinical and experimental medicine: official organ Wroclaw Medical University. Residential wire codes: reproducibility and relation with measured magnetic fields. Blood cells in vitro exposed to low-intensity electric inrush currents of industrial frequency. No induction of chromosome aberrations in human spermatozoa exposed to extremely low frequency electromagnetic fields. Effects of low intensity radiofrequency electromagnetic fields on electrical activity in rat hippocampal slices.