
Toradol
Order toradol 10mg mastercard
The analysis treatment for nerve pain from shingles buy toradol us, in turn, leads to the test of a hypothesis that attempts to interpret the geographical patterns through further epidemiological studies. To explore this postulation, I used spatial Scan Statistics; this allows researchers to measure the significance and location of a general or focused cluster (Kulldorff & Nagarwalla, 1995), subsequently leading to clues about the disease under investigation. Further details about this method appear in a supplement at the end of the dissertation. More methodological considerations also appear in each manuscript comprising the dissertation. In 2010, Ontario’s Excellent Care for All Act stated that high quality health systems must “deliver world-leading effective, patient centered services; efficiently and in a timely manner, resulting in optimal health status for all communities” (Ontario Ministry of Health and Long-Term Care, 2010). In 2016, to complement the Act, Health Quality Ontario stated that creating a safe, effective, patient centred, timely, efficient, and equitable health system requires a systems improvement approach (Health Quality Ontario’s System Quality Advisory Committee, 2016). Health equity is an essential feature of an equitable healthcare system, with concrete implications for policy decisions (Culyer, 2001). Health inequities have been defined as differences in health experiences that “are not only unnecessary and avoidable but, in addition, are considered unfair and unjust” (Kawachi, Subramanian, & Almeida-Filho, 2002; see also Whitehead, 1992). In her ground-breaking work on defining health inequities, Whitehead (1992) maintained that individuals should have a fair opportunity to attain their full and normative health potential, and, what is more, that all inequitable approaches and disadvantages should be avoided. Inequitable approaches include “irrelevant” characteristics such as race/ethnicity, age, gender, education, and income; these should not affect the way a patient is treated unless there are legitimate grounds for the different handling of the patient (Kawachi et al. To quantify inequitable approaches empirically and to inform health equity policies objectively, Culyer (2001) indicates that practical implications for policy on health equity are shaped by 14 “research into the actual distribution of health and sickness: performed in advance of policy initiatives so that the initiatives be informed by the results” (Culyer, 2001; Culyer & Wagstaff, 1993). The most frequently applied method is to compare a health indicator in a disadvantaged group to a similar indicator in a reference, and advantaged, group (Braveman, 2006). However, in a report published by the World Health Organization in 2000, this method was criticized for its prejudged causation effect, as this can obscure differences between groups (Murray, Gakidou, & Frenk, 1999; World Health Organization, 2000). Therefore, some propose measuring health inequities across individuals by means of social groups’ defining criteria, such as community location (Murray et al. This research looks for inequity indicators without applying the previously established markers of social disadvantages (such as income or race). This allows the comparison of sick and healthy individuals rather than rich and poor. The concept of health equity has been categorized as vertical equity (the unequal, but equitable, treatment of unequals) and horizontal equity (the equal treatment of those with equal needs) (Mooney & Jan, 1997). Whitehead’s remarks (1992) encouraged me to look at healthcare associated infections through a different lens. Accordingly, I explored explainable but new and different patterns in the epidemiology of a community-acquired infection, in a quest to locate vertical and horizontal equity policy intervention points to create a fair healthcare system for all. Thesis Overview the dissertation consists of six chapters, as summarized in Figure 1. The first chapter (this chapter) provides a general introduction to the concepts and premises, and the last chapter 15 provides an overall conclusion. Three of the other four chapters represent manuscripts prepared for submission to a peer-reviewed journal. Chapter Two introduces the theoretical lens guiding the conceptual framework of the dissertation. Chapter Four consists of a manuscript titled: “Epidemiology of patients hospitalized with Clostridium difficile infection in the Niagara Region, Ontario, Canada, September 2011 through December 2013: A comparative analysis of community-associated and healthcare-associated Clostridium difficile infections. Chapter Five is a manuscript titled: “A spatial, temporal, and molecular epidemiology study of hospitalized patients infected with community-acquired or healthcare-associated Clostridium difficile in the Niagara Region, Ontario, Canada. It touches on the study limitations, implications for conducting future research and practice, and potential policy implications. A supplement at the end of Chapter Six provides more detail on the methodologies used for the research. Statistical quality control methods in infection control and hospital epidemiology, Part I: Introduction and basic theory. Emergence and global spread of epidemic healthcare-associated Clostridium difficile. International Journal of Environmental Research and Public Health, 12(6), 6948-6964. Clinical Microbiology and Infection: the Official Publication of the European Society of Clinical Microbiology and Infectious Diseases, 18(3), 282-289. Clostridium difficile in beef cattle farms, farmers and their environment: Assessing the spread of the bacterium. Isolation rates and toxigenic potential of Clostridium difficile isolates from various patient populations. For this, and numerous other reasons, including the complexities of healthcare practices, as well as the multiple aspects of diagnosis, treatment, and care delivery settings, scholars in the field of healthcare quality improvement and patient safety argue the need for a systems approach. As two leading researchers in healthcare quality improvement and patient safety make clear: “Systems approaches are necessary for sustained improvement because they consider clinical workflows, care processes, and the overall environment clinicians practice in” (Baker & Axler, 2015). Following this line of thinking, the 2016 recommendations for improving healthcare quality in Ontario urge institutional and organizational leaders to connect with other parts of health systems using their relationship management skills and applying systems thinking throughout their practices (Health Quality Ontario’s System Quality Advisory Committee, 2016). Systems thinking also appears in recommendations for a systems-based approach to reporting (Howley & Chuang, 2011; Petula, 2005). In what follows, I explain my choice of a conceptual framework and show how it shaped my research questions and methodologies. The intent of this approach is to identify and eliminate the hospital-based factors that contribute to the problem. In addition, the cause-and-effect approach using hospital surveillance data alone has proven insufficient, even for hospitals, as we repetitively witness outbreaks; simply stated, this type of approach 31 occasionally lacks the evidence-based support for successful interventions that reduce infection outbreaks. To uncover the epidemiological patterns of diseases, we need a framework that reflects the interrelationships and interdependencies both within and between hospitals and communities. A systems level understanding of the transmission pathways of infections that spread along the continuum of hospitals and communities can prevent emergent infections by making effective interventions. The bottom line is that preventing and reducing transmission in 32 communities reduces the overall burden on healthcare resources. The prevalence has been associated with equity indicators, including crowding and poor ventilation in shelters for the homeless (Figueroa-Munoz & Ramon-Pardo, 2008; Hripcsak et al. In their view, researchers from different disciplines should form an interconnected system of scientific knowledge, accessing research-based information with the ultimate goal of improving and solving health and health equity problems (Pang et al. Other scholars in the field of quality and health systems have supported this proposal, with cross-disciplinary, theory-driven collaboration between hospitals and public health departments noted as a way to broaden the epidemiological tools used to evaluate and investigate causal factors in population health (Perneger, 2005). Finally, I explain the guiding conceptual framework of this research; I show how it directed the formulation of the research questions and the data collection, evaluation, and interpretation. The programs work closely with external organizations, such as public health departments, nursing homes, community care providers, and homecare services, and with services within healthcare organizations, such as laboratories, clinical care services, and 34 occupational health and support services. In my view, this type of framework would be extremely useful, and in this chapter, I propose one possibility. The approach lacks many aspects of the traditional method advocated by the epidemiological triad of host, agent, and environment, the interaction of which produces diseases found both in communities and in hospitals’ emergency departments. Therefore, to better understand the exposure risks and contributing factors to the disease transmission processes, the dynamics of disease transmission and their interplay must be evaluated from all aspects. The present surveillance practices omit the systems’ view that is needed to clearly understand communicable diseases’ processes and the factors contributing to infection formation. As described in Chapter One, program level theories specific to a program are helpful in providing clarity about the component of a program or the mechanism that leads the input to outcomes. They are useful tools to understand evaluation and methods functions (Davidoff et al. However, micro and meso theories lack the scope required to address the complexities of multidimensional preventive strategies at a program and population level. The application of macro theories has been recommended to academics and researchers as a means to uncover assumptions and explain phenomena across multiple different disciplines; this proposed usage fits with the present research. Despite their potential utility, macro-level theories have seldom been applied, however. With the exception of one study applying a macro-level theory or grand theory (systems theory) for management and control of scabies outbreaks, most studies have used mid-level or program-level theories. Initially, the foundations of this theory were set when researchers observed the communication patterns that influenced the behaviour of hybrid corn farmers. Although initially presented as an adoption theory at an individual level, emphasis on innovation and the desire to apply a staged model led to its adaptation for use at an organization 37 level.
Purchase toradol discount
Review article: nutrition and adult inflammatory bowel [32] Corrao G hip pain treatment without surgery order toradol 10 mg fast delivery, Tragnone A, Caprilli R, Trallori G, Papi C, Andreoli A, et al. Am 1999;28(2): vestigators of the Italian Group for the Study of the Colon and the Rectum 423e43. Breastfeeding and risk of Normalization of plasma 25-hydroxy vitamin D is associated with reduced inflammatory bowel disease: a systematic review with meta-analysis. Systematic review: the role of breastfeeding in the development of pediatric Higher plasma vitamin D is associated with reduced risk of Clostridium inflammatory bowel disease. Nutritional status and nutritional therapy in J Gastroenterol Hepatol 2010;25:325e33. Importance of nutrition in inflammatory bowel ronmental factors ininflammatory bowel disease: a case-control study based disease. Aliment Pharmacol Early life environment and natural history of inflammatory bowel diseases. J Pediatr Gastroenterol Nutr 2009;49: [14] Van GossumA, Cabre E, Hebuterne X, Jeppesen P, Krznaric Z, Messing B, et al. J Parenter Enter Nutr 2016 flammatory bowel disease: a systematic review of the literature. Linoleic acid, a dietary n-6 polyunsaturated fatty acid, and the aetiology 2010;105:1799e807. Manipulating the metabolic response to Guidelines for the management of growth failure in childhood inflammatory injury. World Rev [80] Gerasimidis K, Edwards C, Stefanowicz F, Galloway P, McGrogan P, Duncan A, Nutr Diet 2013;106:156e61. Clinical dilemmas in inflammatory bowel disease, new epiphenomenon of the systemic inflammatory response. Vitamin and zinc status pre Changes in energy metabolism after induction therapy in patients with se treatment and posttreatment in patients with inflammatory bowel disease. Energy expenditure and nitro agnose and efficiently treat iron deficiency anaemia in inflammatory bowel gen balance. Pediatr Int 2015;57: the diagnosis and management of iron deficiency and anaemia in inflam 290e4. Measured versus predicted [92] Bonovas S, Fiorino G, Allocca M, Lytras T, Tsantes A, Peyrin-Biroulet L, et al. Clin Nutr Intravenous versus oral iron for the treatment of anaemia in inflammatory 2005;24:1047e55. Inflamm Bowel Dis a randomized controlled trial on ferric carboxymaltose for iron deficiency 2011;17:1587e93. Dig Dis Sci Randomised, double-blind, placebo-controlled trial of fructo 1996;41:1754e9. Malabsorption is a major contributor to [97] Borrelli O, Cordischi L, Cirulli M, Paganelli M, Labalestra V, Uccini S, et al. Nutrition 2006;22: Polymeric diet alone versus corticosteroids in the treatment of active pedi 855e9. Crit Rev Fat composition may be a clue to explain the primary therapeutic effect of Food Sci Nutr 2015;10:1370e8. Guidelines for the management of inflamma [113] Fuchigami T, Ohgushi H, Imamura K, Yao T, Omae T, Watanabe H, et al. The vitamin D status in inflammatory [146] Dziechciarz P, Horvath A, Shamir R, Szajewska H. Gut 2014;63: [150] Fuchssteiner H, Nigl K, Mayer A, Kristensen B, Platzer R, Brunner B, et al. A randomized, placebo-controlled trial of calcium supplementation for [151] August D, Teitelbaum D, Albina J, Bothe A, Guenter P, Heitkemper M, et al. Effect of enterocoated cholestyramine on bowel habit after ileal J Gastroenterol 2005;40(Suppl 16):25e31. Society of Critical Care medicine rhea with ox bile in an ileectomy patient with residual colon. Enteric hyperoxaluria: dependence [155] Nakahigashi M, Yamamoto T, Sacco R, Hanai H, Kobayashi F. Aliment Pharmacol Ther [159] Takagi S, Utsunomiya K, Kuriyama S, Yokoyama H, Takahashi S, Iwabuchi M, 2002;16:1131e5. Aliment Pharmacol Ther European evidence-based consensus on the diagnosis and management of 2006;24:1333e134012. J Crohn Colitis 2012;6: [160] Esaki M, Matsumoto T, Nakamura S, Yada S, Fujisawa K, Jo Y, et al. Does preoperative total parenteral nutrition in patients with ulcerative co [161] Yamamoto T, Shiraki M, Nakahigashi M, Umegae S, Matsumoto K. Perioperative parenteral nutrition in adults with inflammatory prospective cohort study. Consensus review of optimal peri catheter-associated deep venous thrombosis in inflammatory bowel disease. Impact of body mass index and albumin on morbidity and mortality after J Crohns Colitis 2013;7:723e9. Treatment strategies in 135 consecutive patients with enterocutaneous fis Nutrition support in clinical practice: review of published data and recom tulas. Nutritional support sored by the National Institutes of Health, American Society for Parenteral and risk factors of appearance of enterocutaneous fistulas. The second European evidence-based Consensus on the diagnosis and tional status on outcome after hip fracture. Advances in nutritional therapy in severely stressed patients receiving thoracic esophagectomy. Nutritional status, nutrition for the management of inflammatory bowel disease in adults. Gut 2011;60: practices and post-operative complications in patients with gastrointestinal 571e607. Nutritional parameters and short term Clinical features and management of duodenal fistula in patients with outcome in arthroplasty. The role of total parenteral nutrition in inflam in lifestyle associated with long-term home parenteral and enteral nutrition. The impact of nutri enterocutaneous fistula: outcome and factors predictive of increased post tional status on the outcome of lung volume reduction surgery: a prospec operative morbidity. Nutrition as a prognostic indicator in amputa nutritional treatment in Crohn disease. Prevalence of malnutrition in gastric cancer patients undergoing gastrec Nutrition 2011;27:503e4. Nutritional screening for risk prediction in patients scheduled for tion: a prospective 12 month randomised controlled trial. Fish oil fatty acid supplementation in active dietary supplements in pre and postoperative surgical patients: a pro ulcerative colitis: a double-blind, placebo-controlled, crossover study. Randomized clinical trial of the effects of preoperative and postoperative Dietary patterns and self-reported associations of diet with symptoms of oral nutritional supplements on clinical course and cost of care. Pre-operative nutrition support in patients of patients with inflammatory bowel diseases. Lactose malabsorption in pa after digestive surgery: results of a nine-year experience. Clin Nutr 2002;21: tients with inflammatory bowel disease without activity: would it be 59e65. Lancet 1985;2(8448): Early enteral feeding compared with parenteral nutrition after oesophageal 177e80. Influence ribonucleic acid-supplemented diet versus placebo in cancer patients: an of dietary factors on the clinical course of ulcerative colitis: a prospective immunologic evaluation of Impact. Acta Paediatr [224] Bozzetti F, Gavazzi C, Miceli R, Rossi N, Mariani L, Cozzaglio L, et al. World J Gastroenterol 2010;16: parenteral nutrition in the surgical patient: a meta-analysis.
Diseases
- Bonneman Meinecke Reich syndrome
- Urticaria pigmentosa
- Hermaphroditism
- Intestinal spirochetosis
- Myelofibrosis
- Capos syndrome
- Yusho disease
- Savisky syndrome
- Fukuda Miyanomae Nakata syndrome
- Growth mental deficiency syndrome of Myhre
10 mg toradol amex
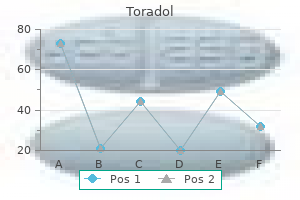
Tere was also beneft with the combined intervention compared with steroid alone for pain and for range of movement at 6 weeks but not the other outcomes pain treatment of the bluegrass cheap toradol 10mg with mastercard. Tere was insufcient evidence to conclude with reasonable certainty in what clinical situations steroid injection, with or without physiotherapy, is most likely to be efective for primary frozen shoulder. All were full papers of studies conducted in Turkey,66 Italy69 and Japan70 between 1996 and 2006. The comparators were steroid injection,66,70 steroid injection and physiotherapy,69 physiotherapy66 and no intervention except for home exercise. Frozen shoulder was diagnosed through physical examination, laboratory tests, subacromial impingement test, clinical history, radiography or ultrasound when described. Quality assessment None of the studies reported the method of randomisation or allocation concealment, and only one stated that blinded outcome assessment was performed; therefore, all three studies have a potentially high risk of bias. Pain All three studies evaluating sodium hyaluronate assessed pain; however, the study by Calis et al. Sodium hyaluronate combined with steroid and physiotherapy versus steroid combined with physiotherapy Rovetta et al. The outcome data for the individual groups in the included trial are available in Appendix 7. Range of movement The range of movement measurements of interest were external rotation, internal rotation and abduction (both passive and active); if internal rotation was not available but hand behind back was reported, this was used as a proxy measure of active internal rotation. Tere was no signifcant diference in passive external rotation or passive abduction between groups (see Table 22). Tere was no signifcant diference in mean external rotation or mean abduction between groups (see Table 22). Quality of life None of the three studies that evaluated sodium hyaluronate assessed quality of life. Adverse events None of the three studies evaluating sodium hyaluronate reported whether or not participants experienced any adverse events. Summary The three included studies investigating sodium hyaluronate used variable doses and in one study sodium hyaluronate was combined with steroid injection and physiotherapy. Because of variations in outcomes reported and comparators used it was not possible to pool data in a meta analysis. The studies did not report participants’ stage of frozen shoulder or previous treatments received. All of the studies had a potentially high risk of bias; none reported the method of randomisation and therefore it was unclear whether they were truly randomised. Because it was unclear whether all studies had enough participants to detect a statistically signifcant treatment efect, it should be kept in mind that where studies did not report a statistically signifcant beneft. One study reported a medium-term beneft in pain outcome when sodium hyaluronate was added to steroid and physiotherapy. The same study also reported a signifcant beneft at medium-term follow-up for internal rotation but not for external rotation or abduction. Another study reported a beneft for function and disability with sodium hyaluronate compared with home exercise but not with physiotherapy or steroid. The same study reported signifcantly better short-term passive external rotation and abduction with sodium hyaluronate than with home exercise and physiotherapy but not steroid injection. A second study reported no evidence of a beneft for external rotation with sodium hyaluronate compared with steroid. In conclusion, a small number of diverse studies of sodium hyaluronate were identifed, all of which may have had a high risk of bias. Tere was insufcient evidence to make conclusions with any certainty about the efectiveness of sodium hyaluronate for primary frozen shoulder and in what situations it is likely to be efective. A summary of the study characteristics is reported in Table 23, with further details available in Appendix 6. Tere were nine two-armed trials,16,40,51,72–74,76–78 two three-armed trials71,75 and one four-armed trial. A variety of physical therapy regimens were used, most of which were physiotherapy modalities. For the purposes of the synthesis, the interventions were grouped based on whether or not at least one component involved mobilisation (of any type) under the supervision of a therapist. Terapies that involved some form of mobilisation (with or without other physical therapies) are described as active therapies. The supervised neglect comparator involved providing patients with an explanation of the natural course of the disease and instructions not to exercise in excess of their pain threshold, to undertake pendulum exercises and active exercises within the painless range and to resume all activities that were tolerated. This study by Stergioulas16 compared laser therapy with placebo laser (with home exercise). Six studies reported that home exercise was used as part of the intervention, although details were limited in some studies. Where specifed the home exercise routines included daily Codman and stretching exercises,66 Codman, stretching and active range of movement exercises,51 daily passive range of movement and pendulum exercises,74 pendulum and pain-free exercises16 and daily stretches. All included patients with some limitation of movement, although the extent of this varied where reported. Primary frozen shoulder was diagnosed through range of movement, biochemical analyses, radiography and clinical diagnosis where reported. The stage of frozen shoulder included was reported by few studies: stage 1 or 2 in the study by Dundar et al. In this study 81% of participants had previously received physical therapy, 61% steroid injections and 6% surgery. The proportion of female participants ranged from 20% to 86% and the mean age of participants ranged from 50 to 62. Only one was of satisfactory quality, reporting the number randomised and both an appropriate method of randomisation and adequate allocation concealment. The main limitation of this study was the study design for the purposes of our review; only limited data were suitable for inclusion in our analysis as diferent sequences of the three same mobilisations were compared at end of treatment (see Appendix 6). Leung and Cheing75 reported that there was no loss to follow-up and loss to follow-up was 15% in the Stergioulas study16 (the majority in the laser group) and 4% in the Vermeulen study40 (with equal numbers from each group). It was unclear whether the method of assignment was truly random in any of these studies and allocation concealment was not reported; therefore, they potentially have high risk of bias. Dropouts were relatively high in the Pajareya study77 (12%, the majority in the control group) and the reporting of satisfaction results was also unclear. The number of participants randomised was inconsistently reported in the study by Maricar and Chok. Dropouts were high in the study by Maricar and Chok (41%)76 and not reported by Wies et al. This study was quasi experimental with a successive cohort as the physical therapy group. The remaining four studies each evaluated diferent physical therapies using diferent comparators; therefore, it was not appropriate to pool the studies in a meta-analysis. The outcome data for individual groups in the included trials are available in Appendix 7. Physical therapy versus physical therapy Tere was no signifcant diference in pain between continuous passive motion and conventional physiotherapy at short-term follow-up (12 weeks) (Table 25). Because of diferences between interventions and comparators it was not appropriate to pool these studies. It is worth noting that there were several factors that could have biased this result. Also, as a successive cohort was recruited afer 2 years (the physiotherapy group), treatment protocols may have changed during the time that elapsed (although the authors did report that a standardised treatment protocol was used). Although the baseline characteristics reported were similar between groups it is possible that there may have been unmeasured diferences between groups. Tere was no signifcant diference between heat pack plus stretching and home exercise (Table 27). The two groups received the three types of mobilisation but in a diferent order over 12 weeks (see Appendix 6). Tere was no signifcant diference in the proportions of patients who reported ‘(much) worse or no change’ at 3 months (13% vs 12%), 6 months (13% vs 10%) or 12 months (9% vs 18%) and ‘better or much better’ at 3 months (87% vs 88%) 6 months (87% vs 90%) or 12 months (91% vs 82%).
Purchase toradol 10 mg
Plasma-derived Mediators (Plasma Proteases) i) by classic pathway through antigen-antibody complexes; these include the various products derived from activation or and interaction of 4 interlinked systems: kinin midsouth pain treatment center jobs buy toradol 10 mg lowest price, clotting, ii) by alternate pathway via non-immunologic agents such as fibrinolytic and complement. These mechanisms are as follows: inflammation are as under: i) Acute phase reactants. Their major role is to protect the normal permeability causing oedema in tissues, augments cells from harmful effects of toxic molecules generated in phagocytosis. These granules contain many substances like proteases, myeloperoxidase, lysozyme, esterase, aryl sulfatase, acid and alkaline phosphatase, and cationic proteins. The diameter of neutrophils ranges from 10 to 15 μm and are actively motile (Table 6. These cells comprise 40-75% of circulating leucocytes and their number is increased in blood (neutrophilia) and tissues in acute bacterial infections. The functions of neutrophils in inflammation are as follows: i) Initial phagocytosis of microorganisms as they form the first line of body defense in bacterial infection. The steps involved are adhesion of neutrophils to vascular endo thelium, emigration through the vessel wall, chemotaxis, engulfment, degranulation, killing and degradation of the foreign material. These are larger than neutrophils but are fewer in number, iii) Free cytokine receptors. The presence of freely circulating comprising 1 to 6% of total blood leucocytes (Table 6. High level of steroid hormones leads to circulating leucocytes, plasma cells and tissue macrophages. Here, it is pertinent to describe the absolute number of eosinophils is increased in the the role of these cells in inflammation. Summary of their following conditions and, thus, they partake in inflammatory morphology, characteristics and functions is given in responses associated with these conditions: Table 6. Basophils (Mast Cells) the basophils comprise about 1% of circulating leucocytes and are morphologically and pharmacologically similar to mast cells of tissue. These cells contain coarse basophilic granules in the cytoplasm and a polymorphonuclear nucleus (Table 6. Chronic inflammatory cell cationic protein, eosinophil peroxidase, neurotoxin) iii. Lymphocytes these cells are larger than lymphocytes with more abundant Next to neutrophils, these cells are the most numerous of cytoplasm and an eccentric nucleus which has cart-wheel the circulating leucocytes (20-45%). Plasma cells are normally lymphocytes are present in large numbers in spleen, thymus, not seen in peripheral blood. These cells are most Their role in antibody formation (B lymphocytes) and in active in antibody synthesis. A, Foreign body giant cell with uniform nuclei dispersed throughout the cytoplasm. B, Langhans’ giant cells with uniform nuclei arranged peripherally or clustered at the two poles. This cell system includes cells derived from 2 sources with g) Growth promoting factors for fibroblasts, blood vessels common morphology, function and origin (Table 6. These include the following cells in different tissues: A few examples of multinucleate giant cells exist in normal i) Macrophages in inflammation. These are seen in tuberculosis and the body as well as participate in immune system of the body sarcoidosis. Their nuclei are like the nuclei of macrophages (Chapter 4); their functions in inflammation are as under: and epithelioid cells. The functions of the periphery in the form of horseshoe or ring, or are clustered mononuclear-phagocyte cells are as under: at the two poles of the giant cell. These multinucleated cells have ii) Macrophages on activation by lymphokines released by T vacuolated cytoplasm due to lipid content. These multinucleate giant cells are variety of biologically active substances as under: derived from cardiac histiocytes and are seen in rheumatic a) Proteases like collagenase and elastase which degrade nodule (Chapter 16). Giant cells in tumours: b) Plasminogen activator which activates the fibrinolytic i) Anaplastic cancer giant cells. Patients who are immuno macrophages but are formed from dividing nuclei of the suppressed from congenital or acquired immunodeficiency neoplastic cells. These are also malignant tumour giant cells which are generally binucleate and are seen in iii) Congenital neutrophil defects. This tumour of the bones has uniform distribution of osteoclastic giant cells spread in the iv) Leukopenia. For instance, ischaemia, presence of vascular and cellular events with emigration of neutrophilic foreign bodies and chemicals cause necrosis and are thus leucocytes, not all examples of acute inflammation show cause more harm. On the other hand, some chronic inflammatory conditions are characterised by neutrophilic 3. For example, typhoid fever is an example of acute the appearance of escaped plasma determines the morpho inflammatory process but the cellular response in it is logic type of inflammation as under: lymphocytic; osteomyelitis is an example of chronic inflammation but the cellular response in this condition is i) Serous, when the fluid exudate resembles serum or is mainly neutrophilic. These are discussed below: ii) Fibrinous, when the fibrin content of the fluid exudate is high. Factors Involving the Organisms iii) Purulent or suppurative exudate is formation of creamy i) Type of injury and infection. Many species and strains of organisms may produces increased secretion of mucous. Vibrio cholerae is not inflammatory response of mucous surface (oral, respiratory, pathogenic if injected subcutaneously but causes cholera if bowel) to toxins of diphtheria or irritant gases. Some organisms produce enzymes where it coagulates, and together with necrosed epithelium, that help in spread of infections. Factors Involving the Host the stomach, duodenum, intestinal ulcers in typhoid fever, i) Systemic diseases. Certain acquired systemic diseases intestinal tuberculosis, bacillary and amoebic dysentery, in the host are associated with impaired inflammatory ulcers of legs due to varicose veins etc. These plasma cells and macrophages with associated fibroblastic conditions render the host more susceptible to infections. Septicaemia is generally accompanied 145 acute bacterial infection is accompanied by intense by systemic effects like toxaemia, multiple small neutrophilic infiltrate in the inflamed tissue, it results in tissue haemorrhages, neutrophilic leucocytosis and disseminated necrosis. The bacteria which cause the blood which cause their effects at the site where they are suppuration are called pyogenic. Microscopically, pus is creamy or opaque in appearance a) Pyaemic abscesses are multiple small abscesses in various and is composed of numerous dead as well as living organs such as in cerebral cortex, myocardium, lungs and neutrophils, some red cells, fragments of tissue debris and renal cortex, resulting from very small emboli fragmented fibrin. Due to tissue destruction, resolution does not occur of septic thrombi in the arteries with relatively larger foci but instead healing by fibrous scarring takes place. Some of the common examples of abscess formation are septic infarcts of the lungs, liver, brain, and kidneys from as under: septic thrombi of leg veins or from acute bacterial i) Boil or furruncle which is an acute inflammation via hair endocarditis (Fig. However, acute resulting from spreading effects of substances like inflammation is associated with systemic effects as well. It is thought to be i) Bacteraemia is defined as presence of small number of mediated through release of factors like prostaglandins, bacteria in the blood which do not multiply significantly. Leucocytosis commonly accompanies the acute culture is done for their detection. When the counts are higher than this with ‘shift ii) Septicaemia means presence of rapidly multiplying, to left’ of myeloid cells, the blood picture is described as highly pathogenic bacteria in the blood. Typhoid fever, an the acute inflammatory process can culminate in one of the example of acute inflammation, however, induces leucopenia following outcomes (Fig. Healing by fibrosis takes place when the tissue represents either a nonspecific reaction to mediators destruction in acute inflammation is extensive so that there released from inflamed tissue or is an immunologic is no tissue regeneration. When the pyogenic bacteria causing acute hyperplasia) and proliferation of mononuclear phago inflammation result in severe tissue necrosis, the process cytic cells in the sinuses of lymph node (sinus histio progresses to suppuration. The abscess, if not drained, may get organised by systemic vasodilatation, increased vascular permeability dense fibrous tissue, and in time, get calcified. These products bring about tissue destruction, Chronic inflammation can be caused by one of the neovascularisation and fibrosis. In chronic inflam When the tissue destruction is extensive, or the bacteria mation, lymphocytes and macrophages influence each other survive and persist in small numbers at the site of acute and release mediators of inflammation. This is brought about by repeated bouts of acute inflammation culminate in activated macrophages which release a variety of biologi chronicity of the process. As a result of necrosis, tion with organisms of low pathogenicity is chronic from the proliferation of small blood vessels and fibroblasts is beginning. As discussed in Chapter 12, chronic inflam inflammatory cells like phagocytes and lymphoid cells.
Purchase 10mg toradol free shipping
Higher Slightly Lower Much Lower Heart rate Cardiac output Stroke volume Mean arterial blood pressure Respiratory rate Total peripheral resistance 11 pain medication for dogs with kidney disease 10 mg toradol fast delivery. During exercise the initial chronotropes and inotropes are the sympathetic nerves that directly innervate the heart. When sympathetic nerves innervating the adrenal medulla are stimulated, epinephrine and norepinephrine are released into the blood. These hormones travel to the heart and perpetuate the response that was initiated by the sympathetic nerves. The constriction of vessels in the lung shunts blood to the areas of the lung that are better ventilated. This results in better ventilation-perfusion matching, which causes more effective oxygenation of blood. This allows each mitochondrion to extract more oxygen from the blood in a given time period. This allows the velocity of blood flow through each vessel to decrease, and the amount of time for oxygen extraction by the mitochondria increases. Discuss the effect long-term endurance training has on the heart and on blood volume. Increases in plasma volume occur shortly after the initiation of intense endurance training. This appears to be caused by an increase in plasma albumin levels, which osmotically draws fluid into the vasculature. Higher plasma volumes cause an increase in venous return, left ventricular end diastolic volume, and stroke volume. Hypertrophy of myocardial muscle also occurs with endurance training, but this is a slower process. The maximal intensity of exercise is not as great as it was when creatine phosphate was being used. To improve the ability of creatine phosphate to provide energy, several bouts of intense exercise should be performed for 5 to 10 seconds with a 30 to 60-second rest between bouts. To improve anaerobic capacity, several bouts of intense exercise should be performed for at most 1 minute in duration with 3 to 5 minutes of recovery between bouts. Compare differences in size, velocity of contraction, fatigability, and metabolism among type 1, type 2a, and type 2b muscle fibers. Fiber Type Type 1 Type 2a Type 2b Fiber name Slow twitch Intermediate twitch Fast twitch Velocity of shortening Low Intermediate High Resistance to fatigue Good Average Poor Diameter Small Intermediate Large Type of metabolism Aerobic Aerobic and anaerobic Anaerobic Exercise Physiology 41 19. Which type of muscle fiber is activated during moderate-intensity, long duration exercise, such as jogging? Which type of muscle fiber is activated during high-intensity, short-term exercise, such as sprinting? The activation of a particular motor unit depends on the size of the α-motor neuron that innervates it. Type 1 fibers are innervated by small α-motor neurons, which have a lower threshold of stimulation than type 2 fibers; type 1 fibers always are stimulated first. Explain why movements become less precise and refined as low-intensity exercise is continued for a prolonged period of time. Initially, low-intensity exercise uses motor units consisting of slow-twitch muscle fibers. These motor units have fewer muscle fibers than motor units with fast-twitch fibers, and this accounts for better control during low-intensity exercises compared with high-intensity exercises. If low intensity exercise is prolonged to the point that glycogen is depleted, the fast-twitch motor units are recruited. Type 1 fibers cannot be converted to type 2 fibers, but type 1 fibers can improve their ability to use anaerobic metabolism, and type 2 fibers can improve their ability to use aerobic metabolism. Type 2b fibers can be converted to type 2a fibers with endurance training, or strength training. This is caused by an increase in capillary and mitochondria content and aerobic oxidative enzyme activity. The cross-sectional area of the muscle decreases, resulting in shorter diffusion distances for oxygen and carbon dioxide. What changes occur in muscle with resistance training, and how long does it take for those changes to occur? Resistance training causes synthesis of proteins in thick and thin filaments, resulting in an increase in cross-sectional area. The aerobic capacity of the muscle decreases, which hinders performance in endurance activities. It takes about 6 to 8 weeks for the addition of protein filaments, but conversion of type 2b to type 2a fibers begins after about 2 weeks. After about 6 weeks of training, 80% of the improvements are from an increase in contractile proteins. The cause of the difference is not known, but it may be due to a greater oxygen-carrying capacity in men caused by a higher hemoglobin content and larger blood volume as well as a higher cardiac output. Women who train heavily have higher levels of catecholamines, cortisol, and β-endorphins. These hormones inhibit the release of luteinizing hormone and follicle-stimulating hormone, which results in decreased levels of estradiol. Studies have shown that physical and emotional stress, diet, and the presence of menstrual irregularity before training also contribute. The duration and intensity of labor are not affected by the level of fitness of the mother, although the perception of pain may be less in physically fit women. Summarize some physiologic changes that occur during pregnancy that affect exercise. After the first trimester, the supine position results in relative obstruction of venous return by the enlarging uterus and a significant decrease in cardiac output. Stroke volume and cardiac output during steady-state exercise are increased significantly. Exercise during pregnancy induces a greater degree of hemoconcentration than does exercise in the nonpregnant state. Because of the increased resting oxygen requirements and the increased work of breathing brought about by physical effects of the enlarged uterus on the diaphragm, decreased oxygen is available for the performance of aerobic exercise during pregnancy. Approximately 300 extra kilocalories per day are required to meet the metabolic needs of pregnancy; this caloric requirement is increased further in pregnant women who exercise regularly. Pregnant women use carbohydrates during exercise at a greater rate than do nonpregnant women; adequate carbohydrate intake for exercising pregnant patients is essential. The intensity of exercise should be such to maintain the heart rate at 65% to 90% of the maximal heart rate except for individuals who are quite unfit; 55% to 64% of maximal heart rate should be used for these individuals. The duration of training should be 20 to 60 minutes of continuous or intermittent (minimum of 10-minute bouts accumulated throughout the day) aerobic activity. The mode of activity should be any activity that uses large muscle groups, which can be maintained continuously and is rhythmic and aerobic in nature, such as walking, jogging, or bicycling. Higher intensity exercise does not need to be performed as long as lower intensity exercises. Proper warm-up and cool-down periods of exercise should be performed: these are increasingly important as the intensity of exercise increases. Resistance training should be progressive, should be individualized, and should provide a stimulus to all major muscle groups. One set of 8 to 10 exercises that conditions the major muscle groups 2 to 3 days per week is recommended. A range of 8 to 12 repetitions of each exercise should be performed; older or more frail individuals should do 10 to 15 repetitions of a lower intensity. Strength is developed best by using heavier weights that require near-maximal tension, with few repetitions. The most successful program to decrease body weight is one that combines exercise with dieting. Such a program decreases weight, decreases fat mass, and maintains or increases fat free mass.
Safe 10mg toradol
Biomechanical Effects of In Vitro Intratendinous Injection and Tendon Fenestration pain medication for dog ear infection buy toradol 10mg low cost. The efficacy of prolotherapy for lateral epicondylosis: A pilot-level randomized controlled trial. The efficacy of prolotherapy using dextrose-morrhuate for lateral epicondylosis: a pilot randomized controlled trial. Poster presentation, Abstract number 235094); International Research Congress on Integrative Medicine and Health; Portland, Oregon. Importance of the Sonographer in the Investigation of Chronic Cerebrospinal Venous Insufficiency. Intratendinous Injection of Platelet-rich Plasma into Lamb Extensor Carpi Radialis Tendon. Autologous Platelet rich Plasma for the Treatment of Chronic Patellar Tendinopathy: Clinical and st Radiographic Outcomes. Effect of an Ultrasound Guided Platelet-rich Plasma Injection for chronic lateral epicondylopathy. Treatment of elbow ulnar collateral ligament injury with platelet-rich plasma: a case report. Sonographic Evaluation of the Subscapularis Tendon after Shoulder Hemiarthroplasty Retrospective Study. Techniques for Interventional Sonography and Thermal Ablation Hands-on th Workshop. Ultrasound-guided Platelet Rich Plasma Therapy of the Tendon – Specific Aims and Background. Nerve Ultrasound Based on a Regional Approach: Shoulder and Neck Hands-on th Workshop. Clinical and Radiological Applications in Prolotherapy and Platelet-Rich Plasma th Research. Cutting-Edge Musculoskeletal Ultrasound: Platelet-rich Plasma Therapy of the Tendon. Dynamic Musculoskeletal Ultrasound for Diagnosis and Treatment of Shoulder Calcific Tendinitis. Tendinosis: Steroid Injection, Tendon Fenestration, or Platelet-Rich Plasma th Injection? Techniques for Interventional Sonography and Thermal Ablation (Hands-on th Workshop). Musculoskeletal Ultrasound: Diagnostic Evaluation of Common Shoulder Problems University of Wisconsin Sports Medicine Symposium. September 18 – 19, 2009, February 26 – 27, 2010, September 28 – 29, 2012, February 16 – 16, 2013, September 20 – 21, 2013, February 21-22, 2014, September 19-20, 2014. Essentials of Musculoskeletal Ultrasound: Diagnostic and Interventional Skills Medical Technology Management Institute. Essentials of Musculoskeletal Ultrasound: Diagnostic and Interventional Skills 33 Medical Technology Management Institute. Achilles, Plantar Fascia and Common Procedures Intermediate Visiting Professorships/Invited Grand Rounds Speaker 1. Musculoskeletal Ultrasound: A complementary tool for diagnosing and treating common sports-related injuries b. Case based review of malignant soft tissue sarcomas of the upper and lower extremity. May 28, 2010 Musculoskeletal Ultrasound of the Shoulder why and how it should be done? Basics of hand and wrist trauma: 2010 September 7, 2011 July 14, 2013 August 27 2014 August 26, 2016 August 2, 2017 September 12 2. Musculoskeletal Cases – 2008 November 6, 2009 March 3, June 16, July 10, November 3, 2010 February 2, April 26, August 20, November 18, 2011 May 5, November 1, 2012 February 7, 2013 January 25, February 22, 2014 June 26 13. Musculoskeletal Fellows Journal Club – August 28, 2015, November 18, 2016, October 20, 2017 14. Musculoskeletal Ultrasound Guided Procedures to Treat Tendon Disease: 2013 January 17 17. Shoulder 1 – Anatomy and Ultrasound Technique with Artifacts – 2017 February 20 37 24. Shoulder 2 – Rotator cuff, biceps, and bursa pathology with Ultrasound Intervention – 2017 May 23 25. Ultrasound of the Knee – Advanced Imaging with Focus on Interventional Procedures: 2011 March 1 State & Regional Community Outreach 2014 What is a Radiologist? Course 832-813– 2009 February 20, March 16, April 21, May 28, July 21, August 18, September 15, October 23, November 12, December 10. Uses of diagnostic ultrasound for msk injury (specifically sports related injury). Ultrasound of Shoulder part I: Normal Anatomy – September 16, 2010, October 6, 2011, October 4, 2012 8. Ultrasound of the Wrist – September 16, 2010, October 6, 2011, October 4, 2012 11. Ultrasound of the Ankle: Normal Anatomy and Common Pathology – September 23, 2010, October 11, 2012 12. Ultrasound evaluation of Morton’s Neuroma – September 23, 2010, October 13, 2011, October 11, 2012 13. Ultrasound-Guided Corticosteroid Injection: Efficacy of Treatment in Patients With Moderate to Severe Plantar Fasciitis Who Have 41 Failed Conservative Therapies. Platelet-Rich Plasma and Hyperosmolar Dextrose (Prolotherapy) for Lateral Epicondylosis: Power Doppler Sonographic Assessment of Tendon Neovascularity as a Measure of the Healing Response. Ultrasound-Guided Microwave Ablation in the Management of Inguinal Neuralgia: A Preliminary Study with 1-Year Follow-up. Supersonic Shear Imaging identifies potential evidence of localized changes in Achilles tendon compliance in middle-aged adults. Platelet-Rich Plasma Injection for Patellar Tendinopathy: Imaging and Clinical Outcomes in Athletes at 1-Year Follow Up. The Importance of the Sonographer in the Investigation of Chronic Cerebrospinal Venous Insufficiency. Cost effectiveness of ultrasound-versus computed tomography-guided soft tissue biopsy (a pilot study and sensitivity analysis). Acoustoelastographic mapping of the stiffness gradient distribution in the rotator cuff for pathologic identification. Ultrasound changes seen in the common extensor tendon during hyperosmolar dextrose (Prolotherapy) treatment for chronic lateral epicondylosis. Hands-On Session: Musculoskeletal Ultrasound Hands-On Workshop Shoulder, Hand, and Wrist. Scapulothoracic: concave (subscapular fossa) Acromioclavicular: 90° abduction on convex (posterior ribs) Sternoclavicular: full elevation Normal end feel Active range of motion (shoulder) Flexion: elastic, frm capsular Flexion. Infraspinatus 12 13 Anterior view of right shoulder Biceps long head tendon Transverse humeral ligament Scapula Glenoid labrum Articular capsule Subscapular bursa Humerus Vizniak Pectoralis major Scapulocostal musculature Tight Weak Erector spinae Abdominal muscles Weak Tight Glut. With longer standing pain, the Other opposite shoulder is favored and gradually loss of. Arthroscopy gold standard investigation, allowing motion and weakness may develop a direct inspection and repair of torn structures in. Loss of strength, possible crepitus with motion the shoulder joint 130 | Orthopedic Conditions Conservative or surgical treatment for subacromial tendon complex lesions of the shoulder. Evaluation of intravenous analgesic for reduction of acute anterior shoulder clinical tests for subacromial impingement syndrome: a propofol and remifentanil for intravenous sedation for reducing dislocations. Shoulder impingement biceps brachii tendon: evaluation with dynamic sonography 75. Limited sensitivity of syndrome: relationships between clinical, functional, during maximal external shoulder rotation. Arthroscopic subacromial decompression: acromioplasty labral detachment lesions of the shoulder.
Terminalia arjuna (Terminalia). Toradol.
- What is Terminalia?
- Treating congestive heart failure (CHF), when used with conventional medications.
- Treating chest pain (angina) after a heart attack, when used with conventional medications.
- How does Terminalia work?
- Dosing considerations for Terminalia.
- Earaches, HIV infection, lung conditions, severe diarrhea, urinary problems, water retention, and other conditions.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96788
Order toradol 10mg without a prescription
The line marks the duodenum; the interrupted line marks the narrowed lumen a b Neoplasms Gastric carcinoma Gastric cancers are echo poor alternative pain treatment center tacoma toradol 10 mg without a prescription, the echo pattern being similar to that of the normal mucosa. Small carcinomas limited to the mucosal and submucosal layer (early gastric carcinomas, stage 1 tumours) can be visualized only if a high resolution transducer and the water-contrast method are used or by endoscopic ultrasound (see also Fig. In cross-section, a ring-like fgure consisting of the echo-poor thickened wall and the stenotic lumen, marked by strong echoes, is seen and is termed a ‘cockade’, ‘pseudokidney sign’ or ‘target-like lesion’ (Fig. Difuse growing carcinomas cause thickeningof theentire gastric wallby up to 10–15 mm. Enlarged, round, echo-poor lymph nodes are highly indicative of metastases but can also be caused by an infammatory reaction. Normal cardia, transverse scan distal to the hiatus (arrow) (vc, vena cava; ao, aorta) 233 Fig. Advanced carcinoma of the antrum (19 mm) causing distal stenosis of the stomach Fig. Cross-section (a) and longitudinal scan (b) show that the entire stomach wall is homogeneously thickened (12 mm). Advanced lymphomas destroy the layers and cause echo-poor thickening of the whole gastric wall. The success of treatment is demonstrated as soon as thethickness decreases and thediferentlayers become visible again (Fig. Transverse and longitudinal scans show thickened dorsal wall (10 mm) with an irregular pattern a b Fig. From thelumen,such tumoursarecovered withtwoor three layers (interface plus mucosal and, mostly, submucosal layer), the so-called ‘bridging sign’ (Fig. Usually, they are found accidentally but sometimes as a source of bleeding if ulceration of the mucosa has developed. The origin of a submucosal tumour found during ultrasonic examination of the abdomen may frst remain unclear but can be revealed by useof thewater-contrasttechnique. To diferentiate between a submucosal tumour and an impression by a process outside the stomach, ultrasound is the best method. Three layers (arrow) are seen between the water-filled lumen and the tumour (T), which clearly indicates its origin in the fourth layer (‘bridging sign’) 237 Differential diagnosis A thickened gastric wall without discernible layers is strongly indicative of malignancy, advanced cancer or malignant lymphoma. A thickened wall with the typical layers still visible is a more ambiguous fnding. Malignancy cannot be excluded, as the layers are ofen discernible in carcinomas of the difuse type (linitis plastica); however, all difuse infammatory and other disorders are possible, as listed with some diferential aspects in Table 11. A normal (not thickened) muscle layer is considered to be a sign of a benign disorder, but a low-grade malignant lymphoma may involve the mucosa exclusively in the earlier stages. An ulcer might also be diagnosed diferentially, especially if the lesion is small and located in the distal part of the stomach. The transition of a tumour to the normal wall is abrupt, whereas the reactive thickened wall in benign ulcers shows a graduated transition to the normal wall. Although ultrasound can be used for some diferential diagnoses, mentioned above, it is not usually suitable for distinguishing between benign and malignant ulcers. They therefore difer clearly from the ‘pseudokidney sign’ of typical gastric carcinomas. The ultrasonic fnding of bright echoes in the centre of gastric carcinomas (marking the narrowed lumen) also distinguishgastrictumoursfromsolidtumoursoftheneighbouringorgans. Diferentiation of larger submucosal tumours from solid tumours of the surrounding structures is, however, ofen possible only with the water-contrast method. Other epithelial tumours of the stomach, such as carcinoid tumours, are seen as smallpolypsbygastroscopy. Distension of the stomach without signs of a distal tumour may be due to an ulcer in the pylorus channel but may also be seen in an advanced stage of vegetative (diabetic) neuropathy. Small and large bowel Indications The indications for ultrasonography of the small and large bowel are: bowel obstruction abdominal pain suspected appendicitis diarrhoea lasting longer than a few days (complications? Generally, ultrasound is not suitable for diagnosing carcinomasof thelargebowel, as only advanced tumours can be visualized. It may, however, be useful for fnding (advanced) tumours, especially lymphomas, in the small bowel, which is not easily accessible by endoscopy. Imaging modalities such as ultrasound are not needed to diagnose or manage acute infective enterocolitis but are useful in looking for complications or other 238 disorders in cases with an uncommon (long) course. As discussed for examination of thestomach, thewater-contrast technique gives a good contrast between the lumen and the wall. Hydrocolonosonography is, therefore, recommended by some authors for delineation of the inner surface of the wall and to visualize small lesions. For this technique, the colon must be cleaned by laxative intestinal lavage, as for colonoscopy. Intravenous application of 20 mg scopolamine N-butyl bromide (Buscopan) is useful to stop peristalsis and for better distension of the colon. If examination of the small bowel is indicated, it may be useful for the patient to drink up to 500 ml of water or another suitable fuid. When the water-contrast method is used, the patient may also be turned in an oblique position. Scanning technique It is useful to start with a longitudinal scan of the right liver lobe to check that the instrument has the correct setting. Ten, longitudinal scans of the whole abdomen are carried out, with the liver, kidneys and aorta as landmarks. Gas in the bowel can be displaced by applying slight pressure with the transducer. For examination of the appendix, the landmarks are the caecum, the terminal ileum and the iliac vessels. The examination is carried out by application of slight pressure in longitudinal and oblique scans. Examination of a patient with acute appendicitis should always include the neighbouring organs, especially the terminal ileum, the lymph nodes and the organs of the small pelvis. Normal findings The duodenum is relatively fxed and can be visualized around thehead of thepancreas and in its further course to the ligament of Treitz. It is identifable mainly on the basis of its content, disturbing gas or echo-poor fuid. The 14–16 loops of the bowel are situated in the middle part of the abdomen, surrounded by the colon. The wall is less than 3 mm thick and consists of an outer, echo-poor layer, corresponding to themuscle layer, and aninner, echo-rich layer due to thesubmucosa and theinterface echoes between thefolds of themucosa and thelumen (Fig. When there is water inside the lumen, ultrasound can reveal the complex inner surface of the mucosa, with the longer villi of the jejunum and the shorter villi 239 of the ileum (Fig. The last loop of the ileum is not difcult to identify; it is located in the lef lower quadrant, with a course from caudal, medial and dorsal to the caecum, which is situated more laterally, cranially and ventrally. The complex structure of the ileocaecal valve can be seen with high-quality ultrasound (Fig. The peristaltic movement of the bowel can be visualized, especially if the loops are flled with fuid. Note the fine pattern of the Kerckring folds (jejunum) The colon is identifed by its largerdiameter, thehaustra coli and its typical course. The anatomically fxed ascending colon is seen on the right side, with the right fexure close to the gall-bladder. The transverse part has a more variable course, whereas the course of the descending colon is fxed on the lef side in front of the iliopsoas muscle. The sigmoid shows no haustra and turns to the midline and backward to the dorsal wall of the bladder. The distal and upper parts of the sigmoid can be demonstrated by using the full bladder as an acoustic window (Fig. The shadow originating at the front of intestinal gas covers the dorsal wall and the structures behind the colon a b 241 The appendix (Fig. With ultrasound, it is sometimes possible to demonstrate the normal appendix, but this cannot be done routinely, as it is a tubular structure about 8 cm long with a diameter of 3–6 mm. It difers from the ileum in that it has a blind end and does not show peristaltic movement. Pathological findings Inflammatory bowel disease Enterocolitis When the bowel is infected with certain microorganisms, the mucosa and submucosa swell and there is augmented secretion of fuid and hyperperistalsis.
Buy toradol cheap online
Deposits ofen occur in the acute phase of the disease and ofen may also be found when the disease is apparently in remission pain treatment center of greater washington generic 10 mg toradol overnight delivery. Benign intratesticular tumours and masses Tese include testicular cysts, ectasia of the rete testis, epidermoid cysts, sarcoidosis, stromal tumours, haematomas, focal orchitis and infarcts. Some have a characteristic appearance on ultrasound scans, others are difcult to distinguish from malignant tumours. These are typical of lymphoma, although in a young man the diferential diagnosis could be multifocal seminoma. Ultrasound appearance The cysts are thin-walled with anechoic contents, acoustic enhancement posteri orly and no solid elements. In contrast, cystic teratomas always have solid elements and thick walls or thick septae (Fig. A typical tunical cyst, situated at the periphery of the testis and bulging into the testis. Although the lesion is predominantly cystic, there are marked solid elements which confrm the diagnosis Cystic ectasia of the rete testis The rete testis is the area at the hilum of the testis where the tubules leave to enter the epididymis. The tubules are of variable size and are ofen just visible on the ultrasound image as multiple thin-walled tubes converging at the hilum. Varying degrees of dilatation or ectasia can occur, assumed to be due to obstruction of the sperm transport mechanism (epididymis or vas deferens). In older men the condition is not important but, in younger men, bilateral ectasia suggests infertility. Dilatation of the rete has sometimes been misdiagnosed as cystic teratoma, particularly if scanned with low-resolution equipment. Carcinoma of the rete testis also produces tubular dilatation in its early stages, but there are coexisting solid elements. A history of haematospermia should raise the suspicion of the diagnosis and in the absence of the symptom it can be discounted. The tumour usually presents at a later stage as a large solid mass, indistinguishable on ultrasound from a germ cell tumour. Ultrasound appearance Mild-to-moderate ectasia appears as multiple tubular structures at the testicular hilum. Epidermoid cyst Testicular epidermoid cysts are benign cystic lesions that, unlike simple cysts, are full of keratin rather than fuid. It is important to recognize them because, if a frm ultrasound diagnosis can be made, they can be excised, and the testis conserved. Granuloma of the tunica albuginea this benign granuloma may be caused by infection or trauma, but is more ofen idiopathic. Small granulomas characteristically feel like a small hard grain of rice on the surface of the testis. Small intratesticular tumours With high-resolution ultrasound systems, very small tumours down to a few millimetres in size can be detected. Small hypoechoic lesions are more of a problem, and may cause a diagnostic dilemma (Fig. However, most lesions of less than 5-mm diameter prove to be benign stromal tumours or cell rests. Intratesticular haematomas Intratesticular haematomas can be caused by severe trauma. While a history of trauma would seem to point to the diagnosis, it is common for patients to present with a testicular tumour afer trauma. This may be because the trauma causes a bleed into the tumour, or because the trauma prompts the patient to examine his scrotum. As with any intratesticular mass, estimation of serum tumour markers and follow-up are mandatory. The tumour was a benign Leydig cell rest a b 376 Ultrasound appearance See section on Trauma in this chapter. Focal orchitis and infarcts Focal orchitis and infarcts may both appear to be tumours. Ultrasound appearances See sections on Epididymo-orchitis and Focal testicular infarcts in this chapter. Testicular atrophy The atrophic testis, whatever the cause, becomes small and heterogeneous with hypoechoic and hyperechoic areas, some due to scarring, others due to Leydig cell rests. In older men with ischaemic atrophy and in younger men with a history of atrophy following mumps infection, these changes may be assumed to be due to atrophy alone. Conversely in men with atrophy due to previously undescended testes, congenital atrophy or hypotrophy, the testes are also likely to be dysplastic. Abnormal areas within these testes must therefore be treated cautiously, with careful follow-up. The testis is typically less than 3 cm in length and inhomogeneous with a prominent hypoechoic area. Epididymal cysts and spermatoceles It is ofen not possible to distinguish between these two benign cystic lesions. Ultrasound appearance Both cysts and spermatoceles are thin-walled, spherical or ovoid structures. These are thin walled with anechoic contents a b Differential diagnosis Large cysts that are indented by the testis may look like hydroceles. Sperm granulomas A granuloma, or scar tissue, may develop in response to sperm that has exuded from the tubules. They are more common following vasectomy, but ofen occur in patients who have not had a vasectomy. They typically cause a dull ache for a few months and thereafer are asymptomatic apart from a palpable mass. Placing a fnger of one hand against the palpable lesion while scanning with the other hand will ofen make the lesion easier to demonstrate. This granuloma is signifcantly hypoechoic and is thus easy to see (transverse view of the epididymis; the testis is out of plane) Adenomatoid tumours Tese are benign tumours of the epididymis that typically occur in middle-aged men. As with sperm granulomas, palpating the lesion while scanning may be necessary to visualize it. Inflammatory and post-inflammatory epididymal masses Epididymitis causes swelling of the epididymis, which is sometimes focal. Focal swellings may persist for a considerable 379 time afer the clinical symptoms have cleared and may be permanent. Tuberculous epididymo-orchitis usually results in a permanent irregular craggy mass. There is a well circumscribed, signifcantly hypoechoic tumour within the epididymis. This persisted after an episode of epididymitis Tubular ectasia of the epididymis Tubular ectasia of the epididymis is a condition that occurs in older men, ofen, though not exclusively, in men who have had a vasectomy. Occasionally one part of the epididymis is more afected and presents as a palpable mass. The dilated tubules making up the lesion are easily seen a b c Varicocele A varicocele is a pathological dilatation of the intrascrotal veins (the pampiniform plexus). A small minority may be due to obstruction by a pelvic tumour or, on the lef side only, a renal tumour invading the renal vein. Rarely, they can be caused by an arteriovenous communication (high-fow varicocele). However, on coughing or with the Valsalva manoeuvre, refux fow occurs, causing the veins to fll with colour (Fig. High-fow varicoceles have high spontaneous fow (without cough or Valsalva manoeuvre). The refux blood fow into the dilated veins is shown a b Inguinal hernia An inguinal hernia may present as a scrotal mass. Ultrasound appearance The echo pattern of a hernia is highly variable, depending on whether it contains omentum or bowel. Ultrasound appearance A large, loculated, cystic structure flls the extratesticular space.
Order toradol with a visa
In old people lower back pain treatment exercise discount toradol on line, the lungs become voluminous areas of fibrosis and atelectasis and involves upper part of due to loss of elastic tissue, thinning and atrophy of the lungs more severely than the lower. Grossly, the destruction of the septal walls and, therefore, preferable subpleural portion of the lung shows air-filled cysts, 0. The involvement is tree such as by a tumour or a foreign body causes irregular as regards the portion of acinus involved as well as overinflation of the region supplied by obstructed bronchus. During life, irregular emphysema Infantile lobar emphysema is a variant of obstructive is often asymptomatic and may be only an incidental autopsy overinflation occurring in infants in the first few days of life who develop respiratory distress or who have congenital finding. Quite often, the lungs during inspiration but cannot leave on expiration the same lung may show more than one type of emphysema. Thus, the lungs of an elderly smoker at autopsy one lung or one of its lobes or segments of a lobe are may show continuation of centriacinar emphysema in the radiolucent. The condition occurs in adults and there is upper lobes, panacinar in the lower lobes, and paraseptal generally a history of serious pulmonary infection in emphysema in the subpleural region. However, a severe and unremitting form of the 483 alveoli and there is histologic evidence of preceding disease termed status asthmaticus may prove fatal. Bronchial asthma is common and prevalent worldwide; in the United States about 4% of population is reported to 5. The entry of air into the connective tissue framework of cases develop it before the age of 10 years. The sexes are affected equally but in children there is 2:1 male usual sources of entry of air into stroma of the lung are female ratio. Hyper of alveoli, the leaked air enters the fibrous connective tissue sensitivity to various extrinsic antigenic substances or of the alveolar walls from where it extends into the fibrous ‘allergens’ is usually present in these cases. Most of these septa of the lung, into the mediastinum, the pleura, and even allergens cause ill-effects by inhalation. Collection of small quantities of stimulated by fumes, gases and organic and chemical dusts air is generally harmless and is resorbed. There are increased levels of accumulation of air in surgical emphysema may produce IgE in the serum and positive skin test with the specific impaired blood flow in the lungs. Pneumo-mediastinum may offending inhaled antigen representing an IgE-mediated type produce symptoms resembling myocardial infarction. I hypersensitivity reaction which includes an ‘acute immediate response’ and a ‘late phase reaction’: Histologically, the alveoli are distended but septal walls Acute immediate response is initiated by IgE-sensitised mast are not damaged; therefore it is not true emphysema. These result in further release of mediators oedema and inflammatory infiltrate consisting of which accentuate the above-mentioned effects. In addition, lymphocytes and plasma cells with prominence of eosino inflammatory injury is caused by neutrophils and by major phils. Changes of bronchitis and emphysema may super of asthma develops later in adult life with negative personal vene, especially in intrinsic asthma. Asthmatic patients suffer from symptom-complex after an upper respiratory tract infection episodes of acute exacerbations interspersed with symptom by viruses. Most attacks typically but about 10% of patients become hypersensitive to drugs, last for a few minutes to hours. When attacks occur most notably to small doses of aspirin (aspirin-sensitive continuously it may result in more serious condition called asthma). The clinical diagnosis is supported by demonstration of circulation eosinophilia and sputum 3. Many patients do not clearly fit into either demonstration of Curschmann’s spirals and Charcot-Leyden of the above two categories and have mixed features of both. The pathologic changes in diameter) developing secondary to inflammatory are similar in both major types of asthma. The most characteristic material examined is generally autopsy of lungs in clinical manifestation of bronchiectasis is persistent cough patients dying of status asthmaticus but the changes are with expectoration of copious amounts of foul-smelling, expected to be similar in non-fatal cases. Post-infectious cases commonly develop Grossly, the lungs are overdistended due to over-inflation. The origin of inflammatory destruc bronchi and bronchioles by viscid mucus plugs. The mucus plugs contain normal or degenerated Endobronchial obstruction by foreign body, neoplastic respiratory epithelium forming twisted strips called growth or enlarged lymph nodes causes resorption of air Curschmann’s spirals. The bronchial wall shows thickened basement growth, or infection may be a primary event i. These 2 mechanisms—endobronchial obstruction and infection, are seen in a number of clinical settings as under: 1. Several hereditary and congenital factors may result secondarily in diffuse bronchiectasis: i) Congenital bronchiectasis caused by developmental defect of the bronchial system. The disease charac teristically affects distal bronchi and bronchioles beyond the segmental bronchi. More vertical air passages of left lower lobe are more often involved than the right. The dilated airways, depending upon their gross or bronchographic appearance, have been subclassified into the following different types (Fig. Cut surface of the affected lobes, generally the lower zones, shows characteristic honey-combed appearance. The bronchi are extensively dilated nearly to the pleura, their walls are thickened and the lumina are filled with mucus or Figure 17. The chronic inflammatory cells and destruction of normal causes of endobronchial obstruction include foreign bodies, muscle and elastic tissue with replacement by fibrosis. Necrotising pneumonias such bands of fibrous tissue between the bronchus and the as in staphylococcal suppurative pneumonia and tuberculosis pleura. Sectioned surface shows honey-combed appearance of the lung in the lower lobe where many thick walled dilated cavities with cartilaginous wall are seen (arrow). The bronchial wall is thickened and infiltrated by acute and chronic inflammatory cells. The mucosa is sloughed off at places with exudate of muco-pus in the lumen (arrow). Sinusitis is a common accompaniment of diffuse expansion of lungs due to alterations in chest wall, pleura bronchiectasis. Late complications occurring in cases and neuromuscular apparatus, but are primarily not lung uncontrolled for years include development of clubbing of parenchymal diseases. Airways Obstructed at any level from Reduced expansion of lung parenchyma trachea to respiratory bronchiole 2. Pulmonary Increased pulmonary resistance and Decreased total lung capacity function test obstruction of maximal expiratory airflow 3. X-ray chest Variable appearance depending Typically bilateral infiltrates giving ground-glass upon the cause shadows 4. The major common clinical manifestations of restrictive 487 lung diseases are exertional dyspnoea, non-persistent I. Connective tissue diseases by inhalation of dust, mostly at work (pneumo = lung; conis = 8. Sarcoidosis (Chapter 6) the type of lung disease varies according to the nature 2. Pulmonary Langerhans cell histiocytosis (eosinophilic 5 μm reach the terminal airways where they are ingested by granuloma of the lung) and morbidity. Eventually, there is widespread destruction of alveolar capillary walls resulting in end-stage lung or ‘honeycomb lung’. Coal dust Simple coal-workers’ the respiratory bronchioles and into the draining lymph pneumoconiosis nodes but does not produce any respiratory difficulty or Progressive massive radiologic changes. Pathogenetically, it appears that anthracosis, simple coal-workers’ pneumoconiosis and 2. Silica Silicosis progressive massive fibrosis are different stages in the evolu Caplan’s syndrome tion of fully-developed coal-workers’ pneumoconiosis. Asbestos Asbestosis However, progressive massive fibrosis develops in a small Pleural diseases proportion of cases (2-8%) of simple coal-workers’ pneumo Tumours coniosis. Beryllium Acute berylliosis implicated in this transformation as follows: Chronic berylliosis 1. Cotton, flax, hemp dust Byssinosis significant role in the pathogenesis of progressive massive 4. Bird droppings Bird-breeders’ (bird fibrosis by release of various mediators (Fig. Mouldy maple bark Maple-bark disease tissues by these inflammatory cells which on activation cause 8.
Buy generic toradol 10mg line
During closed-chain upper extremity exercise pain treatment algorithm purchase toradol 10mg with amex, how much weight is transmitted through the radiocapitellar and ulnohumeral joints? Approximately 60% of the force is transferred through the radiocapitellar joint and 40% through the ulnohumeral joint. Minimal adduction may occur with flexion and minimal abduction with extension, although the magnitude of these movements is debated. If pronation and supination are normal with good motion of the wrist and shoulder, functional mobility may occur with as little as 75 to 120 degrees of motion. The axis of flexion of the elbow is a line through the center of the capitellum and the center of curvature of the trochlear groove, colinear with the distal anterior humeral cortex. Motion resembles a “loose hinge,” with 3 to 5 degrees of rotation and varus/valgus motion during the flexion arc. During pronation and supination, the radius rotates along an axis passing through the center of the radial head and the distal ulnar fovea. The brachialis muscle is the primary flexor of the elbow, inserting approximately 1 cm distal to the coronoid onto both the ulna and the capsule. The pronator quadratus is the primary pronator of the forearm, regardless of elbow position. What is the effect of changing forearm position on muscle testing of elbow flexion strength? Resisting elbow flexion with the forearm in neutral position places maximal stress on the brachioradialis muscle. Pronation strength is 15% to 20% less than supination strength in the normal elbow. Describe the innervation of the various muscles controlling movement at the elbow. Action Muscles Nerve Root Nerve Flexion Brachialis C5, C6 Musculocutaneous Biceps brachii — Brachioradialis Radial Extension Triceps C7 Radial Anconeus Pronation Pronator teres C6, C7 Median Pronator quadratus Supination Biceps C5, C6 Musculocutaneous Supinator C5, C6, C7 Deep branch of radial 22. The medial arcade is formed by the superior and inferior ulnar collateral arteries and the posterior ulnar recurrent artery. The posterior arcade is formed by the medial and lateral arcades and the middle collateral artery. The lateral arcade is formed from the radial and middle collateral, radial recurrent, and interosseous recurrent arteries. What is the order (and approximate age) of ossification of structures around the elbow? The ligament of Osborne is present in all elbows, and two thirds of elbows will also display a discrete arcade of ligament of Struthers. An average of one capsular branch diverges from the ulnar nerve 7 mm proximal to the medial epicondyle. The medial antebrachial cutaneous nerve is subject to painful neuromas if disrupted during surgery. The radial recurrent artery supplies the tendon through branches on its medial and lateral borders. Important contributions are given from the posterior branch of the radial collateral artery and more minor contributions from the interosseous recurrent artery. These arteries form a superficial network with the deep portion of the tendon being nearly avascular. Supination draws the nerve proximal with an average distance of 33 mm from the capitellum. Diliberti T, Botte M, Abrams R: Anatomical considerations regarding the posterior interosseous nerve during posterolateral approaches to the proximal part of the radius, J Bone Joint Surg 82A:809-813, 2000. Yamaguchi K et al: the extraosseous and intraosseous arterial anatomy of the adult elbow, J Bone Joint Surg 79A:1653-1662, 1997. All three joints of the elbow complex are affected because they have a common joint capsule. The joint swelling is most evident in the triangular space between the radial head, tip of the olecranon, and lateral epicondyle. The elbow is held in the loose packed position of about 70 degrees of flexion, because in this position the joints have maximal volume. Little league elbow is a generic term referring to several overuse injuries in young throwers. Examples include osteochondritis dissecans of the capitellum with or without loose bodies, injury and premature closure of the proximal radial epiphysis, overgrowth of the radial head, and medially stressed valgus overuse. The repetitive valgus stress of throwing results in microtrauma of the medial anterior oblique ligament and compression of the radiocapitellar joint. Repeated traction on the olecranon at the site of the triceps brachii insertion may produce olecranon apophysitis or an olecranon stress fracture. Excessive repeated traction through the medial elbow may result in enlargement of the medial humeral epicondyle as well as inflammation of the medial humeral apophysis. Osteochondrosis dissecans of the radial head and/or capitellum or osteochondrosis of the capitellum (Panner’s disease) may result from compressive forces through the lateral elbow during the throwing motion. These same forces can result in injury to the proximal radial epiphysis and early closure of its growth center. In general, little league elbow is treated with relative rest and absolutely no throwing for up to 1 year. If significant fragmentation or separation of the medial humeral apophysis is seen on plain radiographs, surgery may be indicated. One of the main causes of elbow injury in adolescent athletes is throwing pitches that they are not physically prepared to perform. Baseball’s Medical and Safety Advisory Committee has recommended when various pitches should be introduced. The first pitch introduced is the fast ball at 8 years, followed by the change-up at 10 years, the curve ball at 14 years, the knuckle ball at 15 years, and the slider and fork ball at 16 years. Flexing and extending the elbow with maintenance of valgus stress should elicit elbow pain. Loss of passive elbow extension may result from early flexion contracture, which is common in professional pitchers and may represent serious damage in children or adolescents. The term “tendonitis” has been used to describe a hypothetical chronic inflammatory process in the overused tendon. However, histologic examinations of excised pathologic tendons have consistently failed to display the presence of inflammatory cells. Instead, the tissue is characterized by the presence of dense populations of fibroblasts, vascular hyperplasia, and disorganized collagen, termed by Nirschl as angiofibroblastic hyperplasia. Angiofibroblastic hyperplasia appears to be the result of a failed healing response to microtears, combined with vascular deprivation in the tendon’s origin, preventing healing to occur. Which structure is most commonly involved in lateral epicondylitis (tennis elbow)? Tendon fibers attaching to the periosteum are relatively avascular and tend to heal very slowly. Are forearm support bands (counterforce braces) an effective orthosis for lateral epicondylitis? Counterforce braces consist of a flexible band that fits around the proximal forearm and applies pressure to the underlying tissues during activity. While one study showed that they increase the rate of fatigue in unimpaired people, other studies have shown decreased pain threshold with no changes in isokinetic strength. Lateral epicondylitis most commonly occurs in patients between 35 and 50 years of age. In studies performed at industrial health clinics, epicondylitis was most commonly associated with work-related activities (35% to 64% of all reported cases). Tennis players also are at high risk; 10% to 50% will have symptoms at some time in their career. Risk increases with poor stroke mechanics, striking the ball off center, improper grip size, and harder court surfaces. Amateurs tend to have lateral epicondylitis secondary to the backhand whereas professionals usually have medial epicondylitis because of forceful serving. Corticosteroid injections have shown short-term improvement (6 weeks) with this condition; however, the few long-term follow-up studies for this intervention show success rates at 60% or lower. There has been one study that has compared both corticosteroid injection and physical 392 the Elbow and Forearm therapy. Hart found that at 6 weeks, 92% of patients receiving corticosteroid injection reported improvement in symptoms compared to 47% of patients receiving physical therapy. However, at 52 weeks only 69% of patients receiving corticosteroid injections had positive outcome measure ments (self-reported and blinded assessments) compared to 91% for the physical therapy interventions.