
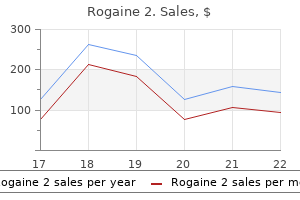
Rogaine 2
Rogaine 2 60ml online
They can be programmed so that an alarm goes off at a particular Depending on the patients abilities and inclinations prostate cancer essential oils cheap rogaine 2, he or she may use a variety time, when the screen displays a message about of memory aids: diaries, notebooks, alarms, calendars, or hand-held electronic persome action the patient should take. If a patient has not previously used such memory aids, however, he or she must be taught how to use them, which can create a paradox: Even after learning how to use a memory aid, the patient must later remember how to use it and then remember to use it in the appropriate situation. Depending on the specic nature of the memory problems, though, many patients can learn new strategies and use them. To ensure that a patient has learned a technique or strategy, the clinician should do the following (Wilson, 2004): Table 15. Once she has mastered this step, she can proceed to learn how to add information to the grocery list. Patients are more likely to remember their own actions than the corrections of errors they make. Thus, mental health professionals may use errorless learning techniques to teach patients new information (Kessels & de Haan, 2003): Patients are explicitly guided in learning a new skill rather than being allowed to gure it out through trial and error. If she didnt know Techniques by which patients are explicitly what to do at a given step, the clinician would show her or provide help ranging from guided in learning a new skill rather than very specic guidance (Now press the green button) to hints or prompts (What do being allowed to gure it out through trial you do rst to add an item To facilitate such generalization, the clinician may teach family members or others how to use the strategies and devices and how to help the patient use them in his or her home environment. Targeting Social Factors: Organizing the Environment One way to reduce the cognitive load of someone with amnestic disorder is to enlist others to structure the patients environment so that memory is less important. For instance, family members can place labels on the outside of cupboard doors and room doors at home or at a residential facility; each label identies what is on the other side of the door (for examthis man has signicant memory problems. In some rehabilitation centers, the notes on his dresser drawers label the type the doors to bathrooms are painted a distinctive color, and arrows on the walls or of items in each drawer. Such modications to his environment can reduce the impact of his oors show the direction to a bathroom, so patients dont need to rely as much on memory problems, and make his experience memory to get around the facility (Wilson, 2004). A paand they may not be able to report their history accurately during tients environment can be structured in order to minimize the a clinical interview. During neuropsychological testing, the principal areas of difficulty on [certain] tests were in mental control, as evidenced by tangential and repetitive speech; psychomotor slowing [in this case, slow movements based on mental processes, not reexes]; and reduced exibility in thought and action (LaRue & Watson, p. In this section we focus on dementia: what it is, what neurological factors give rise to it, and what treatments are available for it. A set of cognitive disorders characterized Dementia is the general term for a set of cognitive disorders that is characterized by decits in learning new information or by decits in learning new information or recalling information already learned recalling information already learned plus at plus at least one of the following types of impaired cognition (American Psychiatric least one other type of cognitive impairment. In dementia, aphasia often appears as overuse of the words thing and it because of difficulty remembering the correct specic words. Problems with executing motor tasks (even though there isnt anything wrong with the appropriate muscles, limbs, or nerves) can lead to problems dressing and eating, at which point self-care becomes impossible. People with dementia may not recognize friends, family members, or even the face in the mirror. These problems lead to difficulties in planning, initiating, organizing, abstracting, and sequencing or even in recognizing that one has memory problems. We discussed aphasia, apraxia, and agnosia earlier, in the context of effects of brain damage on cognition. Unlike the effects of a stroke or a head injury, however, dementia is not caused by an isolated incident. Rather, it arises over a period of time, as brain functioning degrades; symptoms of dementia often change over time, typically becoming worse, but sometimes remaining static or even reversing course. To be diagnosed as having dementia, a person must have cognitive decits severe enough to impair daily functioning, and these decits must contrast with a prior, more adaptive level of functioning. Mild symptoms of dementia may go unnoticed in people whose cognitive functioning started out at a very high level. Early onset, particularly before age 50, is rare and is usually hereditary (Ikeuchi et al. The cognitive decits signicantly impair social or occupational functioning and reect a signicant decline from a previous level of higher functioning. The cognitive decits cannot be better attributed to another Axis I disorder, such as depression [Chapter 6] or schizophrenia [Chapter 12]. Impaired cognitive functioning can lead many patients to feel easily overwhelmed or confused and become agitated. The most common cause of dementia is Alzheimers disease (also called dementia of the Alzheimers type, or simply Alzheimers), in which the affiicted individual initially has problems with both memory and executive function (such as difficulty with abstract thinking and impaired judgment). As the disease advances, memory problems worsen, and attention and language problems emerge, and spatial abilities may deteriorate; the patient may even develop psychotic symptoms, such as hallucinations and delusions (particularly delusions of persecution). Family memA medical condition in which the affiicted bers thus may wait longer before seeking medical assistance for an older person with dementia individual initially has problems with both (Cox, 2007). She got lost on the way home because no landmarks looked familiar; she was unable to remember her address or to recognize her cousin. After neuropsychological and neuroimaging tests, she was diagnosed with early-onset Alzheimers disease (because the disorder emerged before age 65). In her memoir about the progressive nature of this disease, Living in the Labyrinth (1993), McGowin describes sharing with her neurologist some of the symptoms she was having: I showed him the burns on my wrists and arms sustained because I forgot to protect myself when inserting or removing food from the oven. I told him of becoming lost in the neighborhood grocery store where I had shopped for over twenty years. I showed him my scribbled notes and sketched maps of how to travel to the bank, the post office, the grocery, and work. Memories of childhood and long ago events were quite clear, yet I could not remember if I ate that day. On more than one occasion when my grandchildren were visiting, I forgot they were present and left them to their own devices. Moreover, on occasions when I had picked them up to come play at my house, the small children had to direct me home. Childhood nostalgia is so keen I can actually smell the aroma of the small town library where I spent so many childhood hours. Somewhere there is that ever-present reminder list of what I am supposed to do today. However, mental retardation does not primarily involve memory problems; moreover, mental retardation is diagnosed in young people. Such people may technically meet the criteria for dementia in older adulthood (Heaton, Grant, & Matthews, 1991). Although both dementia and schizophrenia often involve hallucinations and delusions, schizophrenia is usually diagnosed earlier in adulthood.
Best purchase for rogaine 2
Numerous studies nd perfectionism to be higher in people with eating disorders than in people who do not have these disorders (Forbush prostate cancer quizlet discount rogaine 2 60ml, Heatherton, & Keel, 2007). High scores on measures of perfectionism persist after people recover, which suggests that this personality trait may exist before an eating disorder arises and may increase the risk for developing such a disorder (Franco-Paredes et al. Thus, bingeing may provide an escape from the emotional distress associated with perfectionism (Blackburn et al. Being aware of imperfections (referred to as aversive self-awareness) causes emotional distress. People high in perfectionism try to decrease the ensuing emotional distress by focusing on immediate aspects of the environment (referred to as cognitive narrowing), which they attain through bingeing (Blackburn et al. For instance, they are likely to be organized planners rather than carefree and spontaneous, which minimizes their exposure to potential danger. Another aspect of personality associated wtih eating disorders is neuroticism (see Chapter 2), which is characterized by a propensity toward anxiety and emotional reactivity (Eggert, Levendosky, & Klump, 2007; Miller et al. Those who had high levels of neuroticism were more likely to develop an eating disorder 18 months later (Cervera et al. People high in neuroticism may be N more sensitive to criticism in general, and when this trait is combined with other P S risk factors (such as an overvaluation of weight and appearance), they may take to heart criticisms or comments related to their weight and appearance more than other people do (Davis, Claridge, & Fox, 2000). Finally, people who have low self-esteem may try to raise their self-esteem by controlling their food intake, weight, and shape, believing that such changes will increase their self-worth (Geller et al. For instance, they may think, If I restrict my calories, thatll prove that Im in control of myself and worthy of respect. If youve ever been on some type of diet, you know that continuing to adhere to such restrictions can be challenging. In fact, it is common for dieters, and people with eating disorders, to alternate restrictive eating with disinhibited eating (Fairburn et al. In addition to dieting, researchers have identied other stimuli that may trigger disinhibited eating. One stimulus is eating more calories than intended or desired, which can trigger the abstinence violation effect. Seemingly paradoxically, disinhibited eating can also be triggered by an upcoming diet. This phenomenon is known as the last supper effect (Eldredge, Agras, & Arnow, 1994) and is sometimes referred to as diet tomorrow, feast today because it leads people to increase their food intake before starting a diet. To study the last supper effect, researchers examined whether anticipation of a week-long diet would lead a group of restrained Figure 10. Unrestrained eaters ate comparable 20 diet for a week or to a group that would amounts, regardless of whether those have no change in food intake. Restrained eaters can also become insensitive to internal cues of hunger and fullness. In order to maintain restricted eating, they may stop eating before they get a normal feeling of fullness and so end up trying to tune out sensations of hunger. They therefore need to rely on external guides, such as portion size or elapsed time since their last meal, to control their food intake (Polivy & Herman, 1993). In fact, the results of one study showed that restrained Restrained eating eaters ate more when they were asked to inhibit their emotional responses to a Restricting intake of specic foods or overall video clip (which required them to increase their cognitive effort) than when they number of calories. A longitudiFemales 30 nal study of 726 adolescents found that having a depressive disorMales der during early adolescence was associated with a higher risk for 25 later dietary restriction, purging, recurrent weight uctuations, and the emergence of an eating disorder. This was the case even when 20 researchers statistically controlled for other disorders or eating problems before adulthood (Johnson, Cohen, Kotler, et al. One social fac5 tor is the role played by family and friends, who have the potential to minimize or amplify an individuals attention to food, weight, and 0 body, and who can help shape individuals thoughts, feelings, and No disorder 1 disorder 2 disorders 3+ disorders behaviors related to food, weight, and body. Another social factor Number of psychological disorders is culture, which can contribute to eating disorders by promoting an during early adolescence ideal body shape; the media, in turn, propagate the cultural ideal. However, researchers have not found it easy to disentangle the inuences of genes from those of the family itself for two main reasons: 1. Family members provide a model for eating, body image, and appearance concerns through their own behaviors (Stein, Woolley, Cooper, et al. For example, parents who spend a lot of time on their appearance before leaving the house model that behavior for their children. Family members affect a childs concerns through their responses toward the childs body shape, weight, and food intake (Stein, Woolley, Senior, et al. For example, if a parent inquires daily about how much food his or her child ate at Children often pay attention to and imitate how lunch or weighs the child daily, the child learns to pay close attention to caloric their family members behave; when parents are intake and daily uctuations in weight. Shed eat normally for a while, then go on a diet, pick at her food, push it away, stare at her butt in the mirror. Friends also play a role, especially if they tease or criticize an individual concerning her weight, appearance, or food intake; such comments can have a lasting inuence on her (dis)satisfaction with her body, her willingness to diet, and her self-esteem. Such inuences can make a person more vulnerable to developing an eating disorder (Cash, 1995; Crowther et al. Hornbacher was aware of this social facet of eating disorders and its underlying drawback: Women use their obsession with weight and food as a point of connection with one another, a commonality even between strangers. Instead of talking about why we use food and weight control as a means of handling emotional stress, we talk ad nauseum about the fact that we dont like our bodies. Hornbacher associated the increased prevalence have a lasting inuence on how she feels about with a cultural fad: her body, her willingness to diet, and her self-esteem. Starving is the feminine thing to do these days, the way swooning was in Victorian times. In the 1920s, women smoked with long cigarette holders and ashed their toothpick legs. A meta-analysis of the incidence of eating disorders across cultures over the 20th century found only a small increase in the number of cases of anorexia. However, Hornbacher seems to have been on the right track about the fad aspect of bulimia. N Three elements come together to create the engine driving the culturally induced increase in eating disorders (Becker et al. In order to examine the cultural ideal of thinness, David Garner and colleagues (1980) undertook an innovative study: They tracked the measurements of Miss America contestants and Playboy centerfold playmates over time and found that their waists and hips gradually became smaller. Other studies have found similar results (Andersen & DiDomenico, 1992; Field et al. During the same period studied by Garner and colleagues, the prevalence of eating disorders increased in the United U. Similarly, men who have a heightened awareness of appearance (Ousley, Cordero, & White, 2008), such as some in the gay community, are also more likely to develop an eating disorder (Carlat, 10. Immigration to a Western country and internalization of Western norms inN crease the risk of developing symptoms of an eating disorder, as occurs among those P S immigrating from China and Egypt to Western countries (Bilukha & Utermohlen, 2002; Lee & Lee, 1996; Perez et al.
| Comparative prices of Rogaine 2 | ||
| # | Retailer | Average price |
| 1 | YUM! Brands | 935 |
| 2 | OfficeMax | 147 |
| 3 | Rite Aid | 575 |
| 4 | A&P | 856 |
| 5 | Delhaize America | 257 |
| 6 | Bed Bath & Beyond | 983 |
| 7 | OSI Restaurant Partners | 790 |
| 8 | Ingles Markets | 152 |
| 9 | Sears Holdings | 413 |
| 10 | Kohl's | 341 |
Buy rogaine 2 60ml with visa
Body Lancashire and south cumbria in north west England and an 8 year expeweight gain and deep brain stimulation mens health 747 workout buy rogaine 2 online. Age at [134] Cereda E, Cassani E, Barichella M, Spadafranca A, Caccialanza R, Bertoli S, onset inuences on wide-ranged clinical features of sporadic amyotrophic et al. Low cardiometabolic risk in Parkinsons disease is independent of lateral sclerosis. Neuro[135] Barichella M, Pinelli G, Iorio L, Cassani E, Valentino A, Pusani C, et al. J Neurol Neurosurg Psychiatry 2004 habits and neurological features of Parkinsons disease patients: implications Apr;75(4):645e7. Outcome of [139] Suzuki M, Yoshioka M, Hashimoto M, Murakami M, Noya M, Takahashi D, percutaneous endoscopic gastrostomy insertion in patients with amyoet al. Randomized, double-blind, placebo-controlled trial of vitamin D suptrophic lateral sclerosis in relation to respiratory dysfunction. Am J Clin Nutr 2013 May 1;97(5): Lateral Scler Front Degener 2013 Dec 25;14(7e8):528e32. Elevated homocysteine levels in gastrostomy in patients with amyotrophic lateral sclerosis. The controversy Amyotrophic lateral sclerosis: enteral nutrition provisiondendoscopic or concerning plasma homocysteine in parkinson disease patients treated with radiologic gastrostomy Plasma homocysteine levels in Parkinsons disease: role of antiAmyotroph Lateral Scler Front Degener 2013 May 4;14(4):308e14. Hyperhomocysteinemia in l-dopa treated Parkinsons disease patients: effect [119] Abdelnour-Mallet M, Verschueren A, Guy N, Soriani M-H, Chalbi M, of cobalamin and folate administration. Vitamins and entacapone in levodopa-induced hyperScler 2011 May 15;12(3):178e84. Major nutritional issues in the manageVitamin A and carotenoids and the risk of Parkinsons disease: a systematic ment of Parkinsons disease. Coenzyme Q10 deciency in patients with of community-dwelling people with Parkinsons disease. Prognostic signicance of weight changes in Pardisability in early Parkinsons disease. A systematic review of the risk and gastrointestinal dysautonomia symptoms in Parkinsons disease prevalence of oropharyngeal dysphagia in stroke, Parkinsons disease, Alzoutpatients hospitalised onascheduled basis. Neurogastroenterol Motil 2012 Swallowing disturbances in Parkinsons disease: a multivariate analysis of Jul;24(7):e277e84. Swallowing abnorVoiceand swallow-related quality of life in idiopathic Parkinsons disease. Asymptomatic normalities as a sign of dysphagia: validation against acoustic and videoswallowing disorders in elderly patients with Parkinsons disease: a uoroscopic data. Med Swallowing impairment and pulmonary dysfunction in Parkinsons disease: Biol Eng Comput 2012 Dec 13;50(12):1261e8. Electrophysiologic patterns of oral-pharyngeal swallowing in parkinsonian [171] Potulska A, Friedman A, Krolicki L, Spychala A. Does levodopa improve swallowing dysfunction in in normal subjects and in patients with swallowing disorders. A pilot study of problems in Parkinson disease: frequency and clinical correlates. J Neurol respiration and swallowing integration in Parkinsons disease: On and Neurosurg Psychiatry 2009 Sep 1;80(9):1047e9. Ann Indian Acad Neurol 2014 Jan;17(1): parkinsonian swallowing dysfunction to dopaminergic stimulation. Park Relat Disord Autonomic symptoms and dopaminergic treatment in de novo Parkinsons 2008;14(8):646e8. Clin Neurol Neurosurg 2008 Feb;110(2): nosis and pharmacological management of Parkinsons disease: summary of 117e9. Park Relat Disord 2014 Practice parameter: treatment of parkinson disease with motor uctuations Sep;20(9):1033e4. J Am Diet Assoc in Parkinson patients versus healthy controls: reliability of measurements in 1995 Sep;95(9):979e83. The prevalence and patterns of oesophageal Does l-dopa treatment contribute to reduction in body weight in elderly dysmotility in patients with Parkinsons disease. J Neurogastroenterol Motil 2015 associated with decreased body weight in patients with Parkinsons disease Mar 30;21(2):283e7. Reproducibility and agreement of pharyngeal automated impedance uences of levodopa on adipose tissue and skeletal muscle metabolism in manometry with videouoroscopy. A method to objectively assess swallow function in adults with suspatients treated long-term with levodopa. Effects of impedance-manometry based method for non-radiological detection of subthalamic nucleus deep brain stimulation and levodopa on energy R. Effect of [244] Bender A, Koch W, Elstner M, Schombacher Y, Bender J, Moeschl M, et al. Management of constipation in Parkin[219] Siniscalchi A, Mancuso F, Gallelli L, Ferreri Ibbadu G, Biagio Mercuri N, De sons disease. Gastroenterology 2013 Jan;144(1): [220] Zoccolella S, Iliceto G, deMari M, Livrea P, Lamberti P. Clin Chem Lab Med 2007 Jan disease: objective assessment and response to psyllium. Effects of therapy for dysphagia in parkinsons dis[250] Barichella M, Pacchetti C, Bolliri C, Cassani E, Iorio L, Pusani C, et al. Nutritional assessment and malnutrition in multiple Park Relat Disord 2014 Aug;20(8):800e7. Rehabilitation or compensation: time for a [252] Poorjavad M, Derakhshandeh F, Etemadifar M, Soleymani B, Minagar A, fresh perspective on speech and language therapy for dysphagia and ParMaghzi A-H. N Engl J Med Comparison of 2 interventions for liquid aspiration on pneumonia incidence: 1952 May 8;246(19):722e8. Nutr Res Rev 2005 Jun expiratory muscle strength training on voluntary cough and swallow func10;18(01):113. Immediate effects of thermal-tactile stimufying nutricals for multiple sclerosis. Pharmacol Ther 2015 Apr;148: lation on timing of swallow in idiopathic parkinsons disease. Low maternal exposure to ultraviolet radiaand oropharyngeal dysphagia: effects on quality of life. Dysphagia 2012 Sep tion in pregnancy, month of birth, and risk of multiple sclerosis in offspring: 13;27(3):336e45. A randomised placebo [238] Barichella M, Marczewska A, De Notaris R, Vairo A, Baldo C, Mauri A, et al. Gluten antibodies in patients with multiple [241] Baroni L, Bonetto C, Tessan F, Goldin D, Cenci L, Magnanini P, et al. J Clin Endocrinol Metab 2004 Mar;89(3): Motor, psychiatric and fatigue features associated with nutritional status and 1196e9. Lancet mortality and survival in multiple sclerosis: ndings from British Columbia. Available a prospective population-based cohort in Bizkaia, Basque Country, Spain. Effects of adjunct Dysphagia in multiple sclerosis: from pathogenesis to diagnosis. Neurol Sci low-dose vitamin d on relapsing-remitting multiple sclerosis progression: 2008 Dec 16;29(S4):360e3. Mult Scler Int [310] Abraham Suzanne, Scheinberg LabeC, Smith Charles R, LaRocca Nicholas G. The Oropharyngeal dysphagia in patients with multiple sclerosis: do the disease effect of vitamin D-related interventions on multiple sclerosis relapses: a classication scales reect dysphagia severity Nat Clin Pract Neurol 2009 Swallowing abnormalities in multiple sclerosis: correlation between videoFeb;5(2):82e92. Linoleic acidandmultiple sclerosis: [319] Terre-Boliart R, Orient-Lopez F, Guevara-Espinosa D, Ramon-Rona S, Bera reanalysis of three double-blind trials. Cochrane dataphysiological evaluation of dysphagia in the mild or moderate patients with base of systematic reviews.
Generic rogaine 2 60ml with visa
These and advocate prostate 5k greensboro generic rogaine 2 60 ml, in addition to becoming a opportunities were more proftable than counseling practitioner. On counselor takes on the role of manager in the other hand, the idea that one is trained a mental health setting. It is easy to feel to provide therapy sometimes discourages unprepared for the bumps and bruises that the individual from considering other take place while learning to lead others. July 2013 Counseling Today 59 What follows are some of the areas I delivered and measured. With the push have found particularly challenging as a for integrated health care and evidencemanager working in mental health. It has source, and when they are introduced to leadership role, he or she been one of my biggest challenges. The manager of these counselors Sometimes we assume that simply having must become familiar needs to understand quality assurance a supervisory title or being called the and improvement, performance boss will speak for itself. In addition, to as legitimate power in the leadership the manager must coach employees in all culture and learn to literature. Many counselor-managers also Specialized programs with grant operate within that assume that because of their employees funding require the counselor-manager backgrounds as clinicians, these belief system. This often to understand all laws and rules relating employees automatically will be to the funding source as well as internal cooperative, be willing to express requires signifcant organizational procedures. This can be concerns and contribute ideas to improve overwhelming for a frst-time leader who is adjustment and change. While paying Managers often face concerns in my mistakes in the work setting through attention to licensure standards, managers mental health organizations regarding purposeful refection and mentoring from must also interpret organizational rules as who is being served, who is in charge my superiors. For example, some for diversity of all kinds in leadership, Organizational culture mental health organizations encourage mental health administration and According to Edgar Schein, each clinical managers to take an authoritarian research. With a rapidly diversifying organization has its own culture that approach to leadership and not take includes artifacts, values and tacit population, the United States is facing excuses from clinicians who are unable assumptions. On the surface, symbols numerous challenges associated with a to reach quotas for billable hours. In that represent the organization are visible lack of ethnically and otherwise diverse another mental health organization, and recognized by members of the leadership. If diversity is absent in mental however, the clinical manager facing this organization, while at the deepest level, health management and leadership, issue may be encouraged to conduct a assumptions and beliefs exist that drive the beliefs and perspectives of those focus group with his or her clinicians to what is considered appropriate or taboo. This often requires for mental health services that support management role in mental health that signifcant adjustment and change. Sometimes and that I was expected to understand it is not always easy to implement in the your inner clinician knows a certain and develop the talents of my employees. But that I need to continually learn from my Managed care, grant directives from higher-ups, organizational employees. They are the front-line service funding and budgeting loyalty, staff concerns or any number providers and possess valuable insights Funding sources often dictate the of other things can interfere with your that can improve what we do as a cohesive groups of clients the organization can programmatic goals for the clients. I have also learned to learn from serve and how treatment is planned, inner clinician aspires to be reasonable 60 ct. But the inner leader knows that the organization expects you to Syllabus Clearinghouse deliver a write-up and a warning about termination to the employee. Future directions It would be benefcial if graduate Need Help Planning counseling programs offered mental health leadership courses to inform students about the full array of careers Your Fall Syllabi Graduate students should be given Ive used it a couple of times for reference; not just for the opportunity to seek electives or additional training in the areas of tests, but also for assignment ideas, course policies, readmanagement/ leadership, organizational ing load (if included), course descriptions, and so on. Here are a few examples of what you will fnd: Learning opportunities that increase understanding of the management, n Thomas Blum, Oakland University business and legal aspects of mental Introduction to Family and Couple Counseling health leadership would help prepare the newest generation of counselor-leaders, n Kathryn MacCluskie, Cleveland State University who are very much in demand in the Laboratory in Counseling Skills world of mental health today. In n Harriet Bachner, Pittsburg State University addition to being a manager Techniques of counseling and psychotherapy with the Center for Health Care Services Head Start Mental Theories and techniques of family therapy Health Program, she has a small Visit and/or contribute today. You can fnd the clearingprivate practice and is a doctoral candidate in education at the house under the Knowledge Center at counseling. The goal of the of Counseling and Related Educational change, according to its announcement Programs)-only language in hiring, in the December 2011 Federal Register, credentialing and reimbursement was to increase access to mental health policies could impact your practice. As care by eliminating the physician-referral/ practicing mental health counselors and supervision requirement. Our practices and states that all of ones post-masters livelihoods are under serious threat, and the supervision hours must have been obtained public faces greatly reduced access to care, under a licensed professional counselor. It is imperative that professional enforcement is not a solution to an overly counselors everywhere understand these restrictive rule. Future initiatives Girls and Womens Wellness: Contemporary Counseling Issues and Interventions Laura Hensley Choate This is an exciting resource for addressing girls and womens issues from a strength-based, holistic perspective that highlights resilience and coping. It will help women discover and actualize their inherent potential for positive change. Myers, PhD the University of North Carolina at Greensboro In this empowering resource, mental health counselors, counselor educators, and school counselors will find an abundance of practical strategies that can be used immediately in their daily practice. Each chapter includes assessment and intervention strategies, client handouts, workshop outlines, self-exploration activities, case studies with discussion questions, and recommended resources. Topics addressed include womens development and mental health, self-esteem, body image, relational aggression in girls, sexual assault and intimate partner violence, college womens experiences, life-work balance, spirituality, and the concerns of mid-life and older women. For more was cohosted with the Association For registration and more information information, visit the conference website for Counselors and Educators in on this exciting online training, visit at collegecounseling. We have had information is shared and how you every step of the way as you make an amazing response to the call for many discussions and idea exchanges your mark in society for those facing programs, so I am confdent of the now take place through these sites, lifes challenges. I look forward to the high-quality programming we will be so we are dedicating a number of amazing year our association will have, featuring. And that is on top of the resources this year to enhance and and I thank you for being part of our networking and career development improve our involvement. We are still publishing counselors and counselor educators to your comments, questions and 11 professional journals and 10 new gather under one roof. Feel free to call me at During 2013-2014, our foray Counseling Today) that can be read 800. You can also Facebook, Twitter, LinkedIn and the need is great in our society follow me on Twitter: @RichYep. De-triangulated rationale/cognitiveInsight gained throughprocesses leading to Behavioral disorders aregenerational transmissionthe result of a multiBeginning:member. Looks for suppressedFamily possesses all are conceptualized asresulting from failure toDysfunctional behaviors Beginning:establish goals. Family structure, subsystems, boundaries/degree of Active director of Behavioral change is based Individual symptomology Beginning:End:Provide closure. Active, take-charge on alleviating currentFocus of therapy issymptoms through altering communication isFocus on howused to increase ones Beginning:interaction stage, goal setting. Narrative Therapy(Post-Modern): and is based on the idea that problemsare manufactured in social, cultural andFocus on the stories of peoples lives families and groups. Individuals, couples, the lines, reauthoring the whole story, reinforcing the newstory, de-constructing dominant cultural discourses. Life stories, externalizing, who is in charge, reading between investigator reporter. Strong interest inCollaborative listener/ when a persons story helpshim to regain his life from aChange and insight occur multiple interpretationsThere is no one objectivetruth and there are Beginning:questions/encourages clients to ask questions. Most contemporary models ofacculturaton emphasize that it is an ongoing process, involving both adoptng thein the Behavioral SciencesAssociation for Advanced Training these aspects of acculturaton are not necessarily correlated, however; i. When counseling a minority group client, the counselorshould determine the clients degree of acculturaton into the majority culture.
Buy rogaine 2 60ml low cost
The reporting mandate includes androgen hormone zyklus buy generic rogaine 2, but is not limited to , any form of child abuse, neglect, or exploitation as required by the Child Abuse and Neglect Reporting Act, Penal Code sections 11164-11174. Page 3 of 10 November 19, 2018 (d) the Evaluation Procedures section shall include record review, clinical interview, mental status examination, and risk instruments utilized or risk factors considered. A prior juvenile adjudication of a sexually violent offense may constitute a prior qualifying conviction if: a. A conviction that resulted in a finding that the person was a mentally disordered sex offender constitutes a prior qualifying conviction. If facts of the qualifying offense or conviction are not available, the Evaluator shall make a reasonable attempt to obtain relevant information. Without other relevant facts, as to the qualifying offense or conviction, the Evaluator may rely solely on the Individuals recollection. The Evaluator shall discuss the validity and any limitation of the information relied upon and offered. Force means to compel a person by physical means to overcome the will of that person. In determining whether force is present in the facts, consider all evidence as to whether the physical or mental state of the victim, including but, not limited to unconsciousness or intoxication, affected the ability of the victim to exert his or her will. Violence means the application of physical force greater than what is necessary to accomplish the act. Duress means the use of direct or implied threat of force, violence, danger, hardship, or retribution sufficient to cause a person to perform an act or submit to an act to which he or she would not otherwise submit. In determining whether duress is present in the facts, consider the totality of the circumstances, including but not limited to the age, mental state, physical stature, maturity of the victim; the victimperpetrator relationship; and specific characteristics of the perpetrator. Menace means any threat, statement, or act which shows intent to inflict injury upon another person. Fear means the apprehension of the victim of physical harm, dread, or awareness of danger. When determining whether fear is present in the facts, consider whether the victim is actually afraid, reasonably or unreasonably, and whether the Individual is aware of and exploits the fear of the victim. Threats to retaliate in the future by means of inflicting future harm against the victim or any other person. In determining whether a threat to retaliate is in the facts, consider whether the victim or the other person has a belief that the Individual will execute the threat. The future criminal sexual acts to which the Evaluator determines the Individual is predisposed need not be violent in nature. The Evaluator shall reference consensus-based diagnostic tools from the professions of psychiatry or psychology, including but not limited to the Diagnostic and Statistical Manual of Mental Disorders or the International Classification of Diseases. The Evaluator may also consider additional evidence in the clinical or empirical literature that is relevant to the Evaluators assessment of psychiatric diagnoses. Emotional capacity is defined as an understanding or appreciation of consequences. Impaired emotional capacity is a defective understanding or appreciation of consequences which may occur as the result of an intellectual or emotional impairment. Impaired volitional capacity is serious difficulty controlling behavior as demonstrated by an Individuals propensity to act impulsively or an Individuals failure to conform his or her behavior to the law despite the risk of criminal punishment. To make that determination, the Evaluator shall review the Individuals background, including but not limited to the Individuals mental health history, medical history, and criminal history. The Evaluator may also consider the Individuals self-report and available records. The Individuals developmental history, including but not limited to: early development, childhood and family dynamics, educational history, exposure to domestic or community violence, past trauma, and any history of emotional, physical, or sexual abuse or neglect; 2. The Individuals employment history, including but not limited to: legal employment, illegal means of earning income, work disciplinary issues, and military history; Page 6 of 10 November 19, 2018 3. The Individuals relationship history, including but not limited to: intimate relationships, current family relationships, and community supports; 4. The Individuals sexual history, including but not limited to: the sexual development, sexual relationship history, current and past sexual functioning or dysfunction, the nature of sexual fantasies and interests including atypical sexual interests or a paraphilia or paraphilic disorder, and if available, the results of sexual interest testing which may include, but is not limited to , penile plethysmograph, polygraph, or visual reaction time measures; 5. The Individuals psychiatric history, including but not limited to: current and past psychiatric diagnoses or symptoms, current and past history of psychiatric treatment, current and past history of sex offender treatment, and current and past history of substance abuse treatment; 6. The Individuals substance use history, including but not limited to: the age of onset; duration of use; severity or frequency of use; effects of use on functioning, including but not limited to sexual functioning, cognitive process, affective regulation, propensity for violence, and impulse control; and other substance use criteria cited in professional consensus diagnostic manuals; 8. The Individuals juvenile and adult criminal history which may be based upon both the Individuals self-report and any available criminal history records that corroborate the Individuals self-report, including but, not limited to allegations; arrests; charges; convictions; violations of rules in institutions such as group home, jail, juvenile or adult correctional facility, or psychiatric hospital; and parole or probation violations. The Evaluator shall also note any limitations of the forensic evidence relied upon; and 9. The Evaluator may supplement his or her mental status examination with a structured mental status instrument. The mental status examination shall include but, is not limited to consideration of the Individuals physical appearance, level of alertness, awareness of their surroundings, attentional capacities, cooperation, thought organization, mood and affect, behavior, memory functioning, ability to communicate, and approach to the interview or specific interview. For the Evaluator to find that an Individual is a menace to the health and safety of others, a recent overt act while the Individual is in custody is not required. The Evaluator shall address Criterion C regardless of the Evaluators conclusion of Criterion B. To assess the Individuals likelihood, the Evaluator may review all available forensic evidence, and relevant clinical information and use empirically-derived risk estimation tools or factors. There is no specific timeframe in considering the Individuals likelihood of engaging in sexually violent criminal behavior. In determining whether sexual crimes are likely to be predatory, the Evaluator may also consider the Individuals prior sexual crimes that were not predatory. The Evaluator shall address whether the Individual can be safely treated in the community and consider the following factors to determine whether a proposed voluntary plan, if any, provides sufficient reduction of risk to reoffend: 1. The intended and collateral effects of such treatment and the influence of those effects on a reasonable expectation that one would voluntarily pursue it; 4. The Individuals progress, if any, in any mandated sex offender treatment program in which the Individual has already participated; and 5. The Individuals expressed intent, if any, to seek out and submit to any necessary treatment, whatever its effects, and any other facts bearing on the credibility and sincerity of such an expression of intent. Certain neurodegenerative conditions may the dominant hand is involved include micrographia also exhibit parkinsonian features; these are labeled (abnormally small, cramped handwriting) and imparkinson-plus or atypical parkinsonian syndromes, pairment in other fine tasks, such as fastening butand include progressive supranuclear palsy. More commonly distal, involving the hands May be observed as patients rest hands in lap; often pill-rolling in nature Nonmotor Features. Most do not respond to , and Must distinguish from spasticity, which only has increased flexor tone may be exacerbated by, dopamine replacement therapy. Both motor and nonmogoals of management are to preserve functionality tor symptoms worsen over time. Of enormous stress, fatigue, anxiety, and ultimately this total burden, almost 70% was related to indidepression; social activities of the caregiver are rect costs in terms of productivity loss and provision impaired and a financial burden often occurs. Prescription drug costs were care is needed for physical limitations of the patient responsible for about 4%. Exclusion of Other Causes of Parkintherapy increase significantly with clinical progressonism. Some questions and reimplicated in the development of parkinsonism are sponses lack clarity; nonmotor symptoms are not haloperidol, risperidone, metoclopramide, and adequately addressed (especially neuropsychiatric); prochlorperazine. In particular, recognition of the imporgressive supranuclear palsy; multiple system atrophy, tant contribution of nonmotor symptoms to disabilsuch as Shy-Drager syndrome; corticobasal gangliity is not reflected in the questions. Several contains more questions than the original scale, supportive criteria can increase the positive predicbut time to complete is similar. However, neuroimaging may be useful in assessing nonmotor symptoms, a nonmotor scale patients presenting with atypical features to help focusing only on this symptom complex would be a rule out other causes of parkinsonism. It has proved effective for currently available to assess nonmotor (and motor) patient management and clinical research. Ten frequently asked is sensitive to changes that matter to the patient but questions about Parkinsons disease. Protein aggregation in the considered the tool of choice,6 some clinicians have pathogenesis of familial and sporadic Parkinsons disease.
Syndromes
- Pyrazinamide
- Difficulty starting or stopping voluntary movements
- National Kidney and Urologic Diseases Information Clearinghouse - http://kidney.niddk.nih.gov
- Excessive sleepiness (lethargy)
- Symptoms reappear
- Breathing support, including a breathing tube
- Sesame seeds

Buy 60ml rogaine 2 visa
Other hepatic tures and other amplification conditions were optimized lesions included bile duct epithelial hyperplasia prostate cancer trials cheap 60 ml rogaine 2 free shipping, periporfor each primer pair. Mycobacterial growth was unpasteurized milk, wild rodents or contact with conassessed by colony formation on solid media or positaminated material [3, 14]. It would be speculative to adtive growth signal by the VersaTrek system and condress the source of the infection in the present case. Germany) and immunochromatographic-based card bovis infection due to small rodent predation [14]. We do not have any knowledge about the sis drugs was performed with the VersaTrek automated feeding of the cat except for house leftovers given. However, no Our isolate was susceptible to isoniazid, ethambutol, riviral immunosupression could be detected in the present fampicin and streptomycin, which are all first-line antireport. Cats are not generally considered to be an importReferences ant host in the epidemiology of tuberculosis; however, 1. Bovine ever, when treatment is pursued in small animals, it tuberculosis in domestic cats. Tuberculosis in should consist of a triple combination of rifampicin, domestic animal species res. Sputum digestion and this is the first reported case in Turkey of a cat infected decontamination with N-acetyl-L-cysteine-sodium hydroxide for culture of with M. Trends of Mycobacterium bovis isolation and first-line anti-tuberculosis drug munosuppression by feline viruses that might make the susceptibility profile: a fifteen-year laboratory-based surveillance. Detection of feline herpes virus 1 via polymerase chain reaction and Funding immunohistochemistry in cats with ulcerative facial dermatitis, eosinophilic the author(s) disclosed receipt of no financial support for the research, granuloma complex reaction patterns and mosquito bite hypersensitivity. Availability of data and materials Molecular characteristics of malignant lymphomas in cats naturally infected All data generated or analysed during this study are included in this with feline immunodeficiency virus. Buonavoglia C, Martella V, Pratelli A, Tempesta M, Cavalli A, Buonavoglia D, et al. Use of computed tomography imaging during long-term follow-up of nine feline tuberculosis Ethics approval and consent to participate cases. PublishersNote Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations. Author details 1Department of Pathology, Faculty of Veterinary Medicine, Firat University, 23 200 Elazig, Turkey. Identify typical signs and symptoms of viral diseases spread by airborne transmission 3. Identify typical signs and symptoms of common foodborne and waterborne viral diseases 3. We will pay covered veterinary expenses that you incur during the policy term for diagnosis or treatment of your pets condition. Benefit payments are subject to all exclusions, limitations, and conditions of this insurance policy. Any veterinary terms or phrases not defined in this policy will be interpreted as defined in the most recent edition of Blood D. Chemotherapy means treatment through chemicals primarily designed to stop the progression of cancer. Chronic condition means a condition that can be treated or managed, but not cured. Congenital anomaly or disorder means a condition that is present from birth, whether inherited or caused by the environment, which may cause or otherwise contribute to illness or disease. Covered veterinary expenses means expenses for reasonable and necessary veterinary services that are eligible for payment under the Major Medical Plan. Cured means eliminated and having no effect on the pet so that the pet is fully restored to normal health without any treatment or management. Developmental defect means an abnormality of a body structure or function that is a result of faulty development, whether apparent or not, that can cause illness or disease. Drug or drugs means medication or other substance undergoing clinical trials for or approved by the U. Hereditary disorder means an abnormality that is genetically transmitted from parent to offspring and may cause illness or disease. All clinical signs or symptoms of an illness constitute one illness, regardless of the number of affected areas of your pets body. Injury means physical damage to part of a pets body caused by an unforeseen physical action or force outside the pets body. Pet means the animal identified on the Declarations Page or Renewal Certificate of your policy. Pet insurance means an individual or group insurance policy that provides coverage for veterinary expenses. Preexisting condition means any condition for which a veterinarian provided medical advice, the pet received treatment for, or the pet displayed signs or symptoms consistent with the stated condition prior to the effective date of a pet insurance policy or during any waiting period. Prescribed means: (1) directly provided by or (2) authorized by written instruction of a veterinarian. Procedure means a veterinary medical or surgical treatment method or course of action. Surgical means healing or therapy that requires cutting or entering a part of the body to repair or remove body tissue. Veterinarian means an individual who holds a valid license to practice veterinary medicine from the Veterinary Medical Board pursuant to Chapter 11 (commencing with Section 4800) of Division 2 of the Business and Professions Code or other appropriate licensing entity in the jurisdiction in which he or she practices. Veterinary expenses means the costs associated with medical advice, diagnosis, care or treatment provided by a veterinarian, including, but not limited to , the cost of drugs prescribed by a veterinarian. Veterinary services means medical advice, diagnosis, care or treatment provided by a veterinarian who has physically examined your pet, including drugs prescribed by the veterinarian. Void means to declare during the policy term that this policy is no longer in force or effect. Waiting or affiliation period means the period of time specified in a pet insurance policy that is required to transpire before some or all of the coverage in the policy can begin. Wild mammal means a mammal that has never been domesticated and generally lives in the state of nature unless captured and confined. You or your means the pet owner listed on the Declarations Page or Renewal Certificate of this policy. Your policy only applies to covered veterinary expenses that you incur during the policy term due to your pets condition that occurs while your policy is in effect. We will pay covered veterinary expenses that you incur during the policy term for the diagnosis or treatment of your pets condition, up to the limits of this policy. To be eligible for payment, your pets condition or procedure to treat this condition must be listed in the Major Medical Plan Benefit Schedule. We will apply your deductible to covered veterinary expenses that you incur during the policy term. We will pay covered veterinary expenses that exceed your deductible, up to the limit of one Column A Primary Diagnosis Allowance and any Column B Secondary Diagnosis Allowance that applies to your pets condition. These Diagnosis Allowances are the most that we will pay during the policy term for any condition covered by this policy, regardless of the number of incidents or treatments during the policy term. Covered veterinary expenses from each incident are eligible for payment under only one Column A Primary Diagnosis Allowance and any applicable Column B Secondary Diagnosis Allowance. In each incident, we will apply the Column A Primary Diagnosis Allowance of the predominant condition for which your pet received veterinary services. We will not pay both a Column A Primary Diagnosis Allowance and a Column B Secondary Diagnosis Allowance under any Diagnosis Code that applies to the same condition. All payments under any Diagnosis Allowance reduce the amount payable under that Diagnosis Allowance for any other covered veterinary expenses incurred during the policy term. Covered veterinary expenses that are paid under one Diagnosis Allowance are not payable under any other Diagnosis Allowance. We will only pay veterinary expenses for diagnostic testing resulting in the diagnosis of a condition that is covered by this policy. We will pay for Specialized Diagnostic Tests conducted by your veterinarian, up to the limits of the Specialized Diagnostic Test amounts listed in the Major Medical Plan Benefit Schedule.
60 ml rogaine 2 visa
Matthew felt trapped and forced to choose between his mother and his girlfriend prostate and bone cancer cheap rogaine 2 60 ml with amex, and because blood is thicker than water, he had decided not to go against his mothers wishes. Matthew is afraid of disagreeing with his mother for fear that she will not be supportive of him and he will then have to fend for himself. He criticizes himself for being weak, but also admires his mother and respects her judgment. Matthew works at a job several grades below what his education and talent would permit. On several occasions he has turned down promotions because he didnt want the responsibility of having to supervise other people or make independent decisions. He has lunch with one of them every single workday and feels lost if his friend is sick and misses a day. He has lived at home his whole life except for 1 year of college, from which he returned because of homesickness. However, with avoidant personality disorder, these characteristics focus on feeling socially inept, whereas with dependent personality disorder, they focus on feeling incapable of taking care of oneself (Skodol, 2005), as Matthew in Case 13. Personality Disorders 617 When considering the diagnosis of dependent personality disorder, clinicians Obsessive-compulsive personality disorder need to keep in mind that cultures have different norms about appropriate deA personality disorder characterized pendent behaviors; moreover, these norms may vary for men and women and for by preoccupations with perfectionism, orderliness, and self-control as well as low people of different ages. For instance, some Asian cultures may promote more deflevels of exibility and efficiency. These behaviors, normal within those cultures, should be distinguished from symptoms of dependent personality disorder (Paniagua, 2001). Obsessive-Compulsive Personality Disorder Obsessive-compulsive personality disorder is characterized by preoccupations with perfectionism, orderliness, and self-control as well as low levels of exibility and efficiency (American Psychiatric Association, 2000). It is the personality disorder associated with the least disability (Skodol, Gunderson, et al. Rachel Reiland describes her father as having some elements of obsessive-compulsive personality disorder: He was strict, coveted control, and became enraged when events werent to his liking. Reiland herself had some elements of this disorder: Once upon a time perfectionism was my noble aspiration. I also aspired to be the perfect mother, lover, and friend, always appropriate in all my emotional expressions (2004, p. People with obsessive-compulsive personality disorder can get so bogged down in details that they leave the most important elements to the last minute (see Table 13. For instance, when preparing a presentation, people with this disorder might spend hours creating a single PowerPoint slide, trying to get it perfect, and end up running out of time for organizing their talk. And, like Reilands father, when they are unable to control a situation, Table 13. They a project because his or her own overly strict standards are not met) may hold others to these same unrealistically strin(3) is excessively devoted to work and productivity to the exclusion of leisure activities gent standards. Typically, people with obsessive-compulsive (7) adopts a miserly spending style toward both self and others; money is viewed as personality disorder feel uncomfortable with othsomething to be hoarded for future catastrophes ers who express emotions easily and openly. People (8) shows rigidity and stubbornness with this disorder are not likely to express tender feelings or pay compliments. Other people often Source: Reprinted with permission from the Diagnostic and Statistical Manual of Mental Disorders, Text Revision, Fourth Edition, (Copyright 2000) American Psychiatric Association. Source: Unless otherwise noted, citations should be American Psychiatric Association, 2000. His presenting complaint was difficulty with completing work effectively, particularly writing tasks, due to excessive anxiety and obsessionality. When he came for treatment, he was struggling to make progress on his masters thesis. V socialized quite a bit, he reported that intimate relationships often felt wooden. A central theme throughout treatment was his tendency to be self-denigrating, loathing himself as a person deserving of punishment in Some workaholics have obsessive-compulsive some way yet being extremely provocative. He also held very strong political beliefs, sure personality disorder: They are perfectionistic and that his way of viewing things was superior to others. Research studies addressing this question have reported mixed ndings (Albert et al. Personality Disorders 619 Understanding Fearful/Anxious Personality Disorders Virtually nothing is known about the neurological bases of fearful/anxious personality disorders, but the apparent similarity between these disorders and anxiety disorders might indicate that the amygdala is involved. In contrast, psychological factors associated with these disorders have been identied. In fact, many of the factors related to social phobia are also involved in avoidant personality disorder, which makes sense, given the overlap in the symptoms of the two disorders. For instance, people with social phobia are also high in the dimension of harm avoidance (Marteinsdottir et al. Moreover, people with both disorders have similar negative beliefs about themselves in relation to other people and avoid social situations for fear of embarrassing themselves (Meyer, 2002; Morey et al. Cognitive and behavioral factors are thought to contribute to all three fearful/ anxious personality disorders, as outlined in Table 13. For all three, patients avoid situations that lead to discomfort and anxiety: With avoidant personality disorder, patients avoid social situations; with dependent personality disorder, they avoid making decisions and having responsibility; and with obsessive-compulsive personality disorder, they avoid making mistakes and experiencing strong emotions. The avoidance perpetuates the cognitive distortions because the patients fears go unchallenged (Beck, Freeman, & Davis, 2004; Farmer & Nelson-Gray, 2005). These factors include anxious or avoidant attachment style, which may have arisen in childhood as a result of particular interaction patterns with parents (Gude et al. Treating Fearful/Anxious Personality Disorders As for most other personality disorders, there is little research on the treatment of fearful/anxious personality disorders, and what research there is has focused primarily on avoidant personality disorder. Although similar to sohis symptoms meet the criteria for avoidant personality disorcial phobia, avoidant personality disorder has criteria that are der. If more pervasive and involve a more general reluctance to take you would like more information to determine his diagnosis, risks. Specically, list which criteria apply and which do and by low levels of exibility and efficiency. Follow-up on Rachel Reiland We can say with certainty that Rachel Reiland suffered from borderline personality disorder. In addition, she displayed signicant elements of two other personality disorders: histrionic personality disorder (her dramatic behaviors may have been motivated by excessive emotional reactivity and a desire for attention) and obsessive-compulsive personality disorder (her rigid thoughts and behaviors may have been motivated by perfectionism). However, it is difficult to determine whether these aspects of her personality met the criteria for the diagnosis of a comorbid personality disorder. Her symptoms of borderline personality disorder were so pronounced that they might have masked additional personality disorders. If a clinician interviewing Reiland had sought to assess the presence of possible comorbid personality disorders, he or she might have spoken with Reilands husband for his perspective, asked Reiland specic questions related to the other personality disorders under consideration, or asked her to complete a personality inventory or questionnaire (described in Chapter 3).
Purchase 60ml rogaine 2 otc
The second non-sexual offence is part of the index because the behaviour occurred prior to detection for the index offence man health 4 all purchase rogaine 2 canada. To count this as a post-index offence, the behaviour would have had to occur after the sentencing date for the index offence. The second non-sexual offence is part of the index because the behaviour occurred prior to the sentencing date for the index sex offence even though the detection and conviction didnt occur until after the detection/conviction for the index sex offence. The second non-sexual offence is considered post-index because the behaviour occurred both after the behaviour and detection/conviction for the index sex offence. Most studies have found that older sex offenders are lower risk to reoffend than younger sex offenders (Barbaree & Blanchard, 2008; Hanson, 2002; Helmus, Thornton, et al. Research has found that the original Static-99 did not fully account for age at release and that a new age weighting improved the predictive accuracy (Helmus, Thornton, et al. With the new age weighting (used in this item), age at release from the index sex offence no longer significantly contributed to the prediction of sexual recidivism after controlling for Static-99R scores (in other words, the new age item fully accounted for age at release). Information Required to Score this Item: To complete this item the evaluator has to confirm the offenders birth date (from the official records if possible) or have other knowledge of the offenders age through collateral report or offender self-report. The evaluator would benefit from access to an official criminal record as compiled by police, court, or correctional authorities that identifies the date of release from the index sex offence. The Basic Rule: Score 1 to 3 points depending on the age of the offender when they are released from their index sex offence referencing the table below: Aged 18 to 34. Under certain conditions, such as anticipated release from custody or presentence reports, the evaluator may be interested in an estimate of the offenders risk at some specific time in the future. Static-99R may be scored months or years before the offenders release to the community and the offender may advance an age scoring category by the time he is released. For assessing risk in the future, consider what his age will be on the date of release from the index sex offence. Sometimes the release date may be uncertain, for example, if he is eligible for parole but may not qualify for release due to an inadequate release plan. In these cases it may be appropriate to use some form of conditional wording indicating how his risk assessment would change with a delayed release date. In any situation where the offender has not yet been released from the index sex offence and their first possible release date is uncertain. Whichever option is chosen should be clearly explained in the risk assessment report. Note that in some cases, the index sex offence identified for Static-99R scoring purposes may not be the same as the offenders current offence. For example, sometimes an offender is serving a sentence for a non-sexual offence but they are assessed as a sex offender due to a prior sex offence. Because this item is scored using age at release from the index sex offence rather than age of release from the current offence, the offender may now be significantly older than when they were released from their index sex offence. For example, an offender may be released from custody on their index sex offence at age 35 and they may be released at age 55 from a current prison term after committing a non-sexual offence. In these cases where an offender has committed subsequent non-sexual offences and is now much older, the effect of aging on sexual recidivism (as well as their continued criminality after the index sex offence) will need to be considered outside Static-99R. For Static-99R assessment purposes, however, the scale will describe the offenders risk when he was released at age 35. For offenders who are released from their index sex offence and are placed on conditional release for several years, they may incur one or more conditional release revocations. The age used would be the age at release after the index sex offence and not the age at release from the revocation. For offenders with an index cluster consisting of multiple release dates, this item should be scored based on the initial release date from the latest sex offence in the cluster. There are limited circumstances where it is possible to make a judgement call that although an offender was released from the index sex offence, they were returned to custody for a technical violation so quickly that the case is more comparable to someone who has been continually incarcerated with no release at all, and you could score their age based on their current anticipated age of re-release. This type of decision is a deviation from the general coding rules and should only be made in extreme circumstances. Specifically, to consider making this judgement, all of the following conditions must apply: the offender was in the community for a short period of time after the initial release from the index offence (no more than 6 months), he was returned to custody for a technical violation (not any behaviour that would be considered a new offence, sexual or non-sexual), and since the revocation, the offender has been in custody for 10 or more years without any kind of release. These situations are most applicable to offenders who are released to the community but are quickly revoked for technical violations and civilly committed. If this decision is made, the evaluator should clearly explain why they did not count the initial release. For purposes of offenders subject to civil commitment in the United States, an offender may be found to meet the criteria as a Sexually Violent Person/Sexually Dangerous Person and not released to the community when their prison term expires. This is because the offender has still not been released to the community since their index sex offence. If the last prison term was for a non-sexual offence then the evaluator should use age at release from the index sex offence. For offenders who are released from their index sex offence and remain in the community for more than two years without a new sex offence please refer to the section on Time Offence Free in the Community after Release from Index Sex Offence (page 13). It may refer to release from court, jail, prison, psychiatric hospital, or the like. Offenders are considered in the community if they are on parole, probation, or other types of community supervision. If they do not receive a custodial sentence for their index offence, the release date would be the date of conviction. If the index sex offence was a charge that did not result in a conviction, date of release is the day the charges were dropped/dismissed. Information Required to Score this Item: To complete this item it is highly desirable that the evaluator confirm the offenders relationship history through collateral sources or official records. The Basic Rule: If the offender has never had an intimate adult relationship of two years duration you score the offender a 1 on this item. If the offender has had an intimate adult relationship of two years duration you score the offender a 0 on this item. This is scored based on relationship history prior to release from the index offence. Live-in relationships lasting longer than two years occurring after the offender is released from the index offence should not be used to score this item; rather, they should be considered outside of Static-99R. The intent of this item is to reflect whether the offender has the personality/psychological resources as an adult to establish a relatively stable marriage-like relationship with another person. It does not matter whether the intimate relationship was/is homosexual or heterosexual or polyamorous. The gender identification/expression of both partners is also not considered in this item. To complete this item the evaluator should make an attempt to confirm the offenders relationship history through collateral sources and official records. In the absence of these sources self-report information may be utilized assuming, of course, that the self-report seems credible and reasonable to the evaluator. There may be certain cases (immigrants, refugees from third world countries) where it is not possible to access collaterals or official records. Where the evaluator, based upon the Balance of Probabilities (see page 19 for definition), is convinced this person has lived with an intimate partner for two years the evaluator may score this item a 0. It is greatly preferred that you confirm the existence of this relationship through collateral contacts or official records. This should certainly be done if the assessment is being carried out in an adversarial context where the offender would have a real motive to pretend to a non-existent relationship. Considerations in Scoring In cases where confirmation of relationship history is not possible or feasible the evaluator may choose to score this item both ways and report the difference in results in their final report. If a person has been incarcerated most of their life, is not allowed to establish an intimate relationship. The first being, this was the way this item was scored in the original samples and to change this definition now would distance the resulting norms and recidivism estimates from those validated on Static-99R.
Purchase genuine rogaine 2 line
The tendency to access and incorporate a wide variety of resources into ones teaching prostate juice recipe discount rogaine 2 60ml. Admission to the Program: Course Sequence the standards and course sequence are carefully crafted to provide program candidates a rich 142 professional experience. It is highly recommended that students plan carefully in order to take advantage of the professional development plan designed to prepare program candidates for the profession of teaching. Upon acceptance after the interview, a student will be formally entered into the Teacher Education Program minor. In addition, program candidates must have appropriate evaluations in each of their feld-based internships. The Teacher Education Faculty reviews and evaluates each program candidates progress at the end of each semester to determine continued eligibility based on the established criteria above, as well as any other reports submitted concerning ethical behaviors. Students who are not in compliance will be blocked from taking additional classes and removed from the Teacher Education Program. The appeal process includes: (1) a written request delivered within one week following the receipt of the letter regarding the decision related to registration for student teaching. It should state the reason(s) an exception should be made; (2) in person explanation to the Teacher Education Committee scheduled within three weeks after the receipt of the written petition of appeal; (3) a decision will be given in writing to the petitioner within one week following the in-person appeal. Chemistry Chemistry Computer Information Systems Career & Technical Education-Computer Sci. In order to apply for licensure, students must: Complete the application for licensure available online at. There is a fee for an offcial transcript **This non-refundable application fee made payable to the Treasurer of Virginia must accompany the application packet. The Registrar will submit the entire application packet to the Virginia Department of Education. Valuation and income determination, internal control systems and basic fnancial statement preparation. Also included are fnancial analysis and concepts of cost, including the effects of cost on revenues, profts, asset values, and capital budgeting decisions. Projects may include audit services, tax services, managerial accounting services, accounting systems development or support services, or fnancial accounting services. Each course will include a minimum of 8 hours of classroom instruction, 12 hours of feld experience, and a summary paper. Emphasis on preparation, interpretation, and analysis of accounting and fnancial data for planning and control, including performance evaluation. A student cannot earn a grade of C or higher in this course unless he or she earns a C or better on the 148 writing assignments required by the course. Emphasis on preparation, interpretation, and analysis of fnancial data prepared for internal users. Items taught include variance analysis, segment reporting, capital budgeting decisions, product pricing and fnancial statement analysis. The course consists of three primary sections: 1) general ledger accounting and accompanying modules; 2) tax software for corporate and personal income taxes; 3) auditing software for the independent audit of business entities. This course integrates computer-applications skills, ability to interpret accounting statements, and investment analysis. Emphasis is on synthesizing the skills and knowledge gained in previous accounting, business, economics, and other courses to obtain new perspectives on contemporary topics. Internships are normally spent in a 400-hour situation or voluntary service activity. They are carefully supervised and designed to provide practical experience in professional accounting environments. The course requires several feld trips to nearby farms including a trip to the Eastern Shore of Virginia. Also includes a section on artifcial insemination, embryo transfer, cloning, and newer technologies. The primary emphasis of the course will be the organization and use of the farm for maximum proft. It includes reviewing college mathematics, an introduction to research methods as relates to real world situations, interpreting formal and media-based studies by drawing inferences, and projects applying these research methods. Several practical issues related to quality management will be considered, including teamwork, leadership, management, decision making and the role of information technology in the support of quality initiatives. Topics include historic and contemporary view of quality (including 6 Sigma, lean, and value-based purchasing), statistical quality improvement tools and methods, and process fow and design. Students will be asked to apply the nutritional concepts they learn to a variety of potential situations they might encounter post-graduation. Students will be asked to apply the concepts they learn to a variety of potential situations they might encounter post-graduation. Topics covered will include physiological processes of reproduction in domestic animals, gonadal functions, endocrine relationships, fertility and factors affecting reproductive effciency. The language of art, art media, and methods are introduced with an emphasis is on understanding, appreciating and discussing art in its cultural and historical context. Students view projected examples, view movies and discuss imagery and artistic techniques in a lecture/discussion format. This will fulfll a fne art requirement and can be used as an elective for Art majors. Problems/projects are organizational, conceptual and thought provoking to challenge and introduce the basic elements and principles of art. It is the intent of this studio experience to establish a disciplined, effcient and practical use of art tools and materials. In this course students will explore formal, functional and conceptual issues that govern three-dimensional work by creating a variety of artworks as assigned. It is the intent of this studio experience to establish a disciplined, effcient, practical and safe use of art tools and materials. Students learn by gaining experience with the physical act of drawing in an attempt to resolve problems of representation and description in fundamental ways. This course is open to all curious students and does not rely upon representational drawing skills. Emphasis is placed upon individual interpretation of class assignments and developing drawings that exhibits versatility and profciency in drawing. It is a beginning studio addressing hand-building techniques including pinch, coil and slab and introduces traditional wheel throwing to expand sensitivity to ceramics material, history, and techniques. This studio experience also introduces glazing and kiln fring applicable to contemporary and sculptural concepts. They will work from a variety of sources including stock images, scans, personal images and their own unique in system compositions. Students will be introduced to the techniques of creating, editing and processing images in the Photoshop environment and organizational skills within Adobe Bridge. Connections to analogue studio techniques will be introduced, including visits to the chemical process photography lab. This is not a photography course and students are not required to purchase a camera. Attention to technical aspects including exposure settings, cameras types, storage media, as well as digital and analogue darkroom techniques. Included are introductions to computer illustration, graphic design, commercial art, image manipulation and related topics. Students will be introduced to a variety of historical and contemporary sculptors and traditions as well as issues and theories about sculpture. The goal of the course is to allow students to develop their aesthetic and technical skills with projects that challenge their level of ability. There will be specifc attention given toward painting materials and the application of techniques to create form in deliberate and creative compositions. Emphasis is placed on the creative use of Internet, Intranet, and World Wide Web systems. Students develop a more advanced commitment to clay and contemporary practitioners and artists while refecting upon the history and techniques of the medium. Students expand their sensitivity to ceramics material, history, and glazing techniques. Students develop conceptual approaches to image-making, cultivate an understanding of the relationship of photography to culture and learn to speak critically of their own and others work.

Buy 60ml rogaine 2
Integrating care for people with cooccurring alcohol and other drug prostate support generic rogaine 2 60 ml on line, medical, and mental health conditions. Chemical dependency and psychiatric services for adolescents in private managed care: Implications for outcomes. Commentary: Dual diagnosis: the status of treating co-occurring disorders in the U. Three-year recovery outcomes for long-term patients with co-occurring schizophrenic and substance use disorders. Prevalence estimates of psychiatric disorders in Intellectual Disability range from 30 percent to 70 percent Virtually all categories of psychiatric disorders have been reported. Often, particularly in those with more severe intellectual disability, specific psychiatric diagnoses cannot be made yet, behavioral symptoms significantly compromise optimal daily functioning by interfering with adaptive, communication, social, learning, recreational and/or motor activities. The childs behavior/attention/interactions may be inappropriate for his/her chronological age but entirely appropriate for his/her developmental age. The psychiatric diagnoses in people with intellectual disabilities tend to accumulate and travel with them for years, so help them sort through which diagnoses are active, and which ones are not. In this case, systematic but empiric approaches to target symptom management are necessary. Attention to possible conditions such as gastresophageal reflux, dental pain, infections, medication side-effect, seizures, constipation and other disorders is important. A basic strategy of "Start low, go slow" is warranted (lower starting doses, increase more slowly. Studies are predominately open trials, case reports or controlled trials with small samples. Diagnostic approaches are modified, depending on the childs cognitive level and communication skills. The poorer the communication skills, the more one has to depend on information provided by caregivers familiar with the child and on direct behavioral observations. Interview (where appropriate) and Observation of Child/Adolescent Ample time should be allotted for the child interview. If there is concern for underlying metabolic disorder, a pediatric genetics and/or child neurology consultation should be obtained. If there is concern about seizure disorder, structural brain abnormality or progressive neurological disorder, a child neurology consultation should be obtained. Psychological Testing Intellectual Disability must be assessed using standardized, full scale measures of intelligence. Frequently used measures of adaptive behavior include nd Adaptive Behavior Assessment System, 2 Ed. Psychological tests can provide additional support for the diagnosis of a psychiatric disorder. Most instruments include guidelines for use with various populations and reading levels. Helping the individual, family, and caregivers deal with or eliminate stressors may sometimes be the primary target of treatment and often facilitates other treatment interventions. They are brought by family or caregivers who are usually concerned about particular behaviors. Consider whether the target symptoms are due to developmental delay, symptoms consistent with a specific developmental disorder, symptoms of a medical condition or signs of psychopathology requiring a psychiatric diagnosis. If the treatment does not work to resolve the presenting problem, consider that the diagnosis may not be correct and that additional information not present at the outset may lead to a new diagnosis. The clinician may need to focus on one or more behavioral symptoms as the target(s) of treatment in the absence of a firm diagnosis. Patient and Caregiver Interview the child or adolescent may present with limited communication skills or may be shy to disclose relevant history. Information from parents and caregivers should always be sought in order to develop a more complete assessment, especially in those instances where the child or adolescent lacks adequate communication skills. Attempts should be made to collect both anecdotal subjective information and more objective data, such as adaptive functioning, daily record keeping, or graphical data. Specialized treatments are also provided if necessary for children and adolescents with additional severe visual and auditory impairment or motor disabilities. Some parents and older children are not fully aware of their rights to obtain services. The clinician has an important role in such instances to educate and, if 2 needed, to refer to a "patient advocate" or "educational advocate. Psychotropic medication should be integrated as part of a comprehensive treatment plan that includes, appropriate behavior planning, behavior monitoring, and communication between the prescribing physician, therapists, and others providing supports, habilitative services, and medical treatment. There should be an effort, over time, to adjust medication doses to document ongoing need or the minimum dose at which a medication remains effective. The prescribing clinician may want to collaborate with a Board Certified Behavior Analyst regarding behavior analysis and treatment. Psychotropic medication decisions need to be made with due consideration for potential problems of polypharmacy, and otherwise for negative impact on the individuals functioning and overall quality of life. Every effort should be made to avoid unnecessary compromise of cognitive, communicative, social, adaptive or motor function. Behavioral Emergencies Individuals will be evaluated for any contraindication for restraint or emergency medication. Techniques typically utilized with persons with mental disorders can be considered potential interventions for persons who are dually diagnosed, with adaptations made as necessary, based on the needs and strengths of the individual. The approach to therapy may need to be more concrete, repetitive, and/or directive, and may need to incorporate visual and auditory aids. Role play can be effective, and behavioral techniques, such as positive reinforcement are very important. Treatment should be appropriate for the individuals cognitive and communicative skills. Generally, the lower the cognitive and adaptive functioning of the child, the more extensive the needed modifications in technique. It considers antecedents (environmental factors that appear to trigger unwanted behavior), the behaviors themselves, and consequences that either increase or decrease future occurrences of that behavior. A treatment program using a behavioral technique known as operant conditioning is then carried out to address the specific challenging behavior, such as self-injurious behavior. Residential Treatment Programs Treatment of children and adolescents with Intellectual Disability should always be in the least restrictive environment possible. Treatment goals as well as target symptoms must be established by the clinicians, family caregivers and where appropriate, the child. Follow-up includes repeated recipient interview/observation and obtaining comprehensive interim information. If the child or adolescent is not experiencing improvement, the accuracy and completeness of the diagnosis should be reviewed, as well as the consistency of implementation of treatment by the caregivers. Treatment of behavior disorders in mental retardation: report on transitioning to atypical antipsychotics, with an emphasis on risperidone. Practitioner Review: Psychopharmacology in children and adolescents with mental retardation. Pharmacotherapy of disruptive behavior in mentally retarded subjects: A review of the current literature. Psychopathology in persons with mental retardation: Clinical guidelines for assessment and treatment. Practice parameters for the assessment and treatment of children, adolescents, and adults with mental retardation and comorbid mental disorders. Journal of the American Academy of Child & Adolescent Psychiatry, 38(12 Suppl), 5S-31S. Healing trauma: the power of group treatment for people with intellectual disabilities. Nationally, increasingly younger children are coming to the attention of schools, courts, and social service agencies for sexual behavior problems. While Tennessee law, state policy and mental health practice originally geared for adult offenders have been modified in part for minors who commit sexual offenses, they do not differentiate between the behavior of older minors and children 12 and under that are experiencing sexual behavioral problems. However, research has shown that the assessment and treatment needs of children ages 12 and under who have sexual behavior problems are different from the assessment and treatment needs of adolescents who offend sexually.