
Avanafil
Avanafil 200mg lowest price
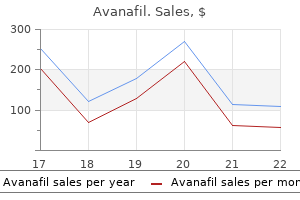
While satisfied workers may better tolerate longer work hours sleep in a 24 hour hours statistics of erectile dysfunction in india avanafil 200 mg for sale, it also is possible that some employees gradually habituate period (Belenky et al. For example, the National Highway Traffic Safety Administration estimates that drowsiness is the primary causal factor in more than 100, 000 police-reported motor More than one-third of U. Those real world amount of sleep, and one-half report fatigue-related events sometimes are highly publicized. The equipment requires individuals to respond to a small, bright red light by pressing a response button. This action stops the stimulus counter and displays the reaction time in milliseconds. The subject is instructed to respond as quickly as possible, but not to press the button too soon (which will cause a false start warning). The interval between stimuli varies randomly from 2 to 10 seconds, and the total test time is 10 minutes or a total of 90 reaction times. Fatigue relates to a complex interaction of physiological, cognitive and emotional factors. Fa tigue results in slowed reactions, poor judgment, reduced information processing and an inabil ity to continue performing a task or to carry it out at a high, sustained level of accuracy or safety. The pervasive problem of fatigue is due principally to one or more conditions including: lack of sleep, interrupted or poor quality sleep (which denies opportunities for protracted deep sleep ing periods), disrupted circadian work and rest cycles, and illnesses such as sleep apnea. Sitting inactive in a 0 1 2 3 public place, like a meeting or classroom Total number of points (The total [0 to 24] is the Epworth score, and a value of 10 or higher indicates excessive sleepiness. This manipulation can be useful when studying the assessment of interventions purporting to reduce sleepiness. The Epworth Sleepiness Scale lists eight specific real-life situations, and the subject is asked to rate the likelihood of falling asleep during any of these activities. The total score can vary between 0 and 24, and values of 10 or greater indicate excessive daytime sleepiness. Subjective fatigue differs from alertness and has many mental and physical dimensions, only one of which is the impact of sleep and circadian rhythm disruption. Only recently have survey instruments been developed that are easy to administer and have robust psychometric properties of construct reliability and discriminant validity (Winwood et al. The normal daily 24 hour rhythm results in alertness being greatest during the day, and conversely, the maximal drive for sleep is during biological night. Being awake for prolonged periods, such as when working more than a typical eight hour shift, also impairs performance (Jewett, 1997). Thus, a drowsy driver may be as dangerous as a drunk driver (Dawson & Reid, 1997; Falleti et al. Those findings led to federal regulations limiting the number of consecutive hours that truckers can drive (see Section 3); there is a greater than 15-fold increase in the risk of a fatigue-related fatal crash after more than 13 hours awake compared to the first hour (Department of Transportation, 2000). Other occupations demonstrate similar time dependent errors, and the on-the-job accident rate increases during the later hours of longer shifts (Tucker, Smith, Macdonald & Folkard, 2000), so that 10-hour shifts were found to increase accident risk more than 10 percent, and 12-hour shifts increased risk more than 25 percent. Repeated failure to obtain sufficient sleep has a cumulative detrimental effect on alertness and performance that increases linearly with sleep loss (van Dongen et al. Workers beginning a series of night shifts generally sleep poorly following each of their night shifts, and the cumulative effect of lack of restorative sleep may explain the higher accident rate observed with each successive night shift worked, so that by the fourth night the risk is increased 36 percent above the first night (Folkard, Lombardi & Tucker, 2005). Chronic sleep loss results in decreased ability to think clearly, handle complex mental tasks, form new memories and solve problems (Koslowsky & Babkoff, 1992; Durmer & Dinges, 2005; Stickgold, 2005; Rouch et al. In a study of more than 7000 Dutch employees from a variety of worksites, investigators found that occupational accidents were significantly more likely during shift work, especially during nights, and self-reported fatigue was a contributing factor (Swaen et al. Sleep has effects on brain receptors for serotonin and other neurotransmitters, which are related to mood and memory. In laboratory studies, only a few days of sleep restriction altered these receptor levels, and a week of restorative sleep was required to reverse the changes (Roman et al. The disorder can be treated with typical serotonin re-uptake inhibitor antidepressants or exposure to high intensity light, simulating longer, brighter days. According to the International Classification of Sleep Disorders, shift work sleep disorder is considered a specific diagnosis because of the frequency with which shift workers suffer from sleep disturbances and excessive sleepiness (Beer, 2000). Shift workers also are more likely to drive while fatigued, and they are almost twice as likely to fall asleep at the wheel. Shift work sleep disorder is charac Recently, employers have recognized that health is more terized by fatigue, functional impair than the absence of injury and illness, and that worker ment, difficulties initiating and main well being and presenteeism may have a greater taining sleep that are not readily rem economic impact than the more traditional indices of edied by behavioral measures and the health care costs (Mills, 2005). It may occur in 10 to 20 percent date, work hours and sleep deprivation have not been of night or rotating shift workers related to presenteeism or more global quality of life (Sherman & Strohl, 2004). They also can lead to a constant feeling of fatigue, irritability and a reduced sense of well being. A consistent relationship between increasing work hours and more health complaints was observed across studies. More recent data from approximately 20, 000 European workers from a broad range of occupations confirmed a clear direct correlation between the number of hours worked per week and health complaints (Raediker et al. Caruso and colleagues (2004) performed a critical review of studies linking work hours and health outcomes. In their analysis, they examined the effects of shift work and shift work also accompanied by longer total work hours (more than 40 hours a week). When those latter criteria were met, individuals consistently demonstrated lower perceived general well being and more health problems, along with an increased risk of occupational injuries. Eight hours of sleep per night is recommended for adults, because that number is the average preferred duration among healthy people who do not have other demands limiting sleep. Longitudinal studies comparing sleep duration and health outcomes seem to confirm that optimum duration. Mortality increases in men and women when they deviate from that average amount of sleep each night. In long term studies, even controlling for other factors influencing life expectancy, sleeping less than eight hours per night was associated with higher mortality rate (Heslop et al. Several lines of evidence indicate that long work hours (more than 50 to 60 hours each week) increase the incidence of, and risk factors for, heart disease and cardiovascular events. Most studies linking heart disease and long work hours have been among Japanese men. The stages of deep sleep are times when the heart rate and blood pressure are lowered, and important bodily repair functions occur. Daytime ambulatory blood pressure cuff measurements found that prolonged work hours were associated with an increase in blood pressure (Fialho et al.
Purchase discount avanafil on-line
The damaged annulus is fixed autologous pericardium and posterior annular reconstruc replaced with the pericardium and sutured to the healthy ven tion effective erectile dysfunction treatment buy genuine avanafil online. Tricuspid valve endocarditis can be managed by vegetec tricular endocardium and the anterior mitral leaflet. In conservative are obliterated with pericardium after debridement and irriga management, the tricuspid valve can be converted to a bicuspid tion. If the valve substitute selected is a homograft (allograft), valve with chordal replacement. The tricuspid valve involved the attached anterior leaflet tissue is useful for closure of sub with infective endocarditis can be replaced with a mitral allo valvular abscesses and closure of perforations at the base of the graft (46). Mitral and tricuspid valve sparing procedures with native anterior mitral leaflet. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee and anterior mitral leaflet of the allograft can be used in the on Management of Patients with Valvular Heart Disease). The options for allo acute streptococcal pharyngitis and prevention of rheumatic fever: A statement for health professionals: Committee on Rheumatic graft use are the scalloped, intra-aortic cylinder and allograft Fever, Endocarditis, and Kawasaki Disease of the Council on aortic root replacement. The infected annulus can be locally Cardiovascular Disease in the Young, the American Heart treated with phenol or iodine solution. Prevention of bacterial replacement for severe destructive native or prosthetic endocarditis. N Engl J Med of adults with infective endocarditis due to streptococci, 1995;332:38-44. Patient selection criteria and Prospective randomized comparison with parenteral therapy. Native valve infective choosing the optimal prophylaxis of bacterial endocarditis. A controlled evaluation of protective contraindication for urgent valve replacement in acute infective efficacy. Native valve infective endocarditis in elderly and treatment in native infective endocarditis. A seven-year younger adult patients: Comparison of clinical features and experience. Surgical treatment of Infective endocarditis: An analysis based on strict case definitions. Long-term survival infective endocarditis: Utilization of specific echocardiographic after aortic valve replacement for native active infective findings. Recommendations for prevention, and determinants of mortality after surgery for native and prosthetic diagnosis and treatment of infective endocarditis. Surgical treatment of active 36 Piper C, Hetzer R, Korfer R, Bergemann R, Horstkotte D. Pratali S, Nardi C, Di Gregorio O, Becherini F, Milano A, infective endocarditis: Reassessment of prognostic implications of Bortolotti U. Combined mitral and tricuspid valve repair in acute vegetation size determined by the transthoracic and the infective endocarditis. Mitral valve repair and transesophageal echocardiographic echocardiography as an adjunct to transthoracic echocardiography findings in a high-risk subgroup of patients with active, acute in evaluation of native and prosthetic valve endocarditis. Ann Thorac Surg complicated prosthetic aortic valve endocarditits with annular 1994;58:429-33. A stroke or permanent neurological event lasts more than three weeks or causes death. The definitions and recommendations that follow are Patients who do not awaken or who awaken after operation guidelines, not standards. These guidelines are designed to with a new stroke are excluded in tabulations of valve related facilitate comparisons between the experiences of different sur morbidity. Follow-up for 30-day mortality must be rial embolus is shown to be the cause of the infarction by oper complete. Hospital mortality is death within any time interval ation, autopsy or clinical investigation. Emboli proven to after operation if the patient is not discharged from the hospi consist of nonthrombotic material (eg, atherosclerosis, myxoma) tal. Embolic stroke complicated by bleeding is abnormality of the valve that causes stenosis or regurgitation. Whether patients were receiving a platelet calcification, leaflet tear, stent creep and suture line disruption inhibitory drug or not (eg, acetylsalicylic acid, dipyridamole) of components (eg, leaflets, chordae) of an operated valve. Nonstructural dysfunction: Nonstructural dysfunction is an Operated valvular endocarditis: Operated valvular endocardi abnormality resulting in stenosis or regurgitation at the operated this is any infection involving an operated valve. The diagnosis of operated valvular endocarditis is based on Nonstructural dysfunction refers to nonstructural problems customary clinical criteria including an appropriate combina that result in dysfunction of an operated valve exclusive of tion of positive blood cultures, clinical signs or histological thrombosis and infection diagnosed by reoperation, autopsy or confirmation of endocarditis at reoperation or autopsy. Examples of nonstructural dysfunction Morbidity associated with active infection such as valve include entrapment by pannus, tissue or suture; paravalvular thrombosis, thrombotic embolus, a bleeding event or par leak; inappropriate sizing or positioning; residual leak or avalvular leak, is included under this category and is not obstruction from valve implantation or repair; and clinically included in other categories of morbidity. Sudden or progressive operated valvular dysfunction or Consequences of morbid events deterioration may be structural, nonstructural or both, as Reoperation: Reoperation is any operation that repairs, alters determined by reoperation, autopsy or clinical investigation. Valve thrombosis: Valve thrombosis is any thrombus, in the the reasons for reoperation should be reported and may absence of infection, attached to or near an operated valve include reasons other than valve-related morbidity, such as that occludes part of the blood flow path, or that interferes recall, excessive noise, or incidental or prophylactic removal. Enzymatic or catheter-aided therapy of valve-related morbidity Valve thrombosis may be documented by operation, autopsy is not considered reoperation, but the morbid event that or clinical investigation. Embolism: Embolism is any embolic event that occurs in the Valve-related mortality: Valve-related mortality is death absence of infection after the immediate perioperative period caused by structural valvular deterioration, nonstructural dys (when anesthesia-induced unconsciousness is completely function, valve thrombosis, embolism, a bleeding event, oper reversed). Deaths caused by heart failure in patients with disease but without resulting limitation of physical activity. Objective evidence of minimal limitation: Patients with deaths and the relationship to an operated valve are unknown. Comfortable at rest; ordinary physical activity results gory of valve-related mortality if the cause cannot be deter in fatigue, palpitation, dyspnea or anginal pain. This category includes valve-related deaths with cardiac disease resulting in marked limitation of physical (including sudden unexplained deaths) and nonvalve-related activity. Comfortable at rest; less than ordinary physical cardiac deaths (eg, congestive heart failure, acute myocardial activity causes fatigue, palpitation, dyspnea or anginal pain. Symptoms of heart failure or the anginal impairment is any permanent neurological or other functional syndrome may be present even at rest. If any physical activity deficit caused by structural valvular deterioration, nonstruc is undertaken, discomfort is increased. Pain on moderate exertion: Ordinary physical activity, such posed longitudinal outcomes valvular surgery module can be as walking or climbing stairs does not cause angina. Pain with used for early mortality risk stratification and long term analy strenuous, rapid or prolonged exertion. Pain limitation of normal daily activities: Comfortable at rest, software for Canadian centres contracting with the organiza but ordinary physical activity, such as walking rapidly or tion. The participant-generated software has been developed climbing stairs, exercise after meals, in wind or cold weather and has received validation by the Duke Clinical Research causes anginal pain. This provides the opportunity for additional modules walking on the level or climbing one flight of stairs. Pre Operative Hemodynamics and Cath Number of Diseased Coronary Vessels: (None) (One) (Two) (Three) Left Main Disease > 50%: No Yes Ejection Fraction Done If yes, Gradient: Aortic Insufficiency: 0=None 1=Trivial 2=Mild 3= Moderate 4= Severe Mitral Stenosis: No Yes Mitral Insufficiency: 0=None 1=Trivial 2=Mild 3= Moderate 4= Severe Tricuspid Stenosis: No Yes Tricuspid Insufficiency: 0=None 1=Trivial 2=Mild 3= Moderate 4= Severe Pulmonic Stenosis: No Yes Pulmonic Insufficiency: 0=None 1=Trivial 2=Mild 3= Moderate 4= Severe J. Other Non Cardiac Procedures No Yes Aortic Aneurysm No Yes Carotid Endarterectomy No Yes Other Vascular No Yes Other Thoracic P. Post Operative Blood Products Used: No Yes Initial # of Hrs Ventilated Postop: Re-intubated During Hosp Stay: No Yes
Avanafil 50mg free shipping
The short course of treatment is a better option in these instances as 5 fluorouracil requires twenty-one days of application impotence tumblr purchase genuine avanafil on line. Craig Percy Developmental Editor: Richard Johnson Cover Designer: Steve Pisano Indexer: Joann Woy Compositor: Patricia Wallenburg Printer: Victor Graphics Visit our website at No part of it may be reproduced, stored in a retrieval sys tem, or transmitted in any form or by any means, electronic, mechanical, photocopying, recording, or otherwise, without the prior written permission of the publisher. Research and clinical experience are continually expanding our knowledge, in particular our knowledge of proper treatment and drug therapy. Nevertheless, this does not imply or express any guarantee or responsibility on the part of the authors, editors, or publisher with respect to any dosage instructions and forms of application stated in the book. Every reader should examine carefully the package inserts accompanying each drug and check with a his physician or specialist whether the dosage schedules mentioned therein or the contraindications stated by the manufacturer differ from the statements made in this book. The editors and publisher welcome any reader to report to the publisher any dis crepancies or inaccuracies noticed. Historically, on-the-job training, usually in a one-on-one setting, has been the stan dard by which most neophyte electroencephalographers acquire the exposure from those who are more senior in experience and knowl edge. Patterns of special significance underlie features that appear often during states of stupor or coma. Chapters on sleep and neurointensive and intraoperative monitoring add useful information to complete the handbook for clinicians that would ben efit from quick and easy pattern recognition. It is a graphic display of a differ ence in voltages from two sites of brain function recorded over time. Electrical signals are created when electrical charges move within the central nervous system. Neural function is normally maintained by ionic gradients established by neuronal membranes. Sufficient duration and length of small amounts (in microvolts) of electrical cur rents of cerebral activity are required to be amplified and displayed for interpretation. With depolariza tion, an influx of positive-charged (sodium) ions that exceeds the normal electrochemical resting state occurs. Channel opening within the lipid bilayer is via a voltage-dependent mechanism, and closure is time dependent. Conduction to adjacent portions of the nerve cell membranes results in an action potential when the depolarization threshold is exceeded. The brainstem and thalamus serve as subcortical generators to synchronize populations of neocortical neurons in both normal. All generators have both a positive and negative pole that function as a dipole (Figure 1. During routine use, electrical potentials are acquired indirectly from the scalp surface and incorpo rate waveform analyses of frequency, voltage, morphology, and topography. Furthermore, the waveforms that are recorded from the scalp represent pooled synchronous activ ity from large populations of neurons that create the cortical poten tials and may not represent small interictal or ictal sources. From the patient scalp, electrodes conduct electrical potentials to an electrode box (jackbox). These sites are then subdivided by intervals of 10% to 20% and to designate the site where an electrode will be placed. Subsequently, numbers combined following the letters for location reflect either the left (odd numbers) or right (even num bers) hemisphere of electrode placement. Special electrodes may also be added such as sphenoidal, true tempo ral, or frontotemporal electrodes. True temporal electrodes (desig nated T1 and T2) are placed to help distinguish anterior temporal or posterior inferior frontal location not delineated by the F7 or F8 posi tions. Subdermal electrodes are used when other recording techniques are not feasible such as in the operating room and intensive care unit. Electrode placements systems use either a 10-20 system (black circles) or modified combinatorial system with 10-10 electrode placement (black circles + white circles). Respiratory monitors may also be important if respiratory problems are identified. Bipolar montages may be arranged in many different spatial formats including longitudi nally, transverse fashion, or in a circumferential pattern. An anterior to posterior temporal and central connecting chain of electrodes arranged left alternating with right-sided placement is a typical array. Bipolar montages compare active electrodes sites adjacent to each other and signify absolute electrographic sites of maximal nega tivity (or positivity) by phase reversals (Figure 1. Recordings are usually performed with a visual display of 30 mm/sec (slower with sleep studies), amplifier sensitivities of 7 IV/mm, and fil ter settings of 1 to 70 Hz. Reducing the low filter settings promotes slower frequency representation, while reducing high filter settings decrease high frequency. Various generators of nonphysiological and physiological artifacts may deceive the interpreter to believe that the apparent sources are abnormal or epileptiform. In the example above, pulse artifact is seen that is usually seen in a sin gle channel as a periodic slow wave. Eye movement monitors demonstrating the in-phase cerebral ori gin of the diffusely slow background in this awake patient, and the out-of-phase movement of the eye blink artifacts during seconds 3 and 8. Normally, the eye functions as an electrical dipole with a relative positivity of the cornea compared to the retina. Artifact from three horizontal eye movements (looking left) followed by two vertical eye blinks. When the eyes move to the left yielding a pos itive phase reversal in F7 due to the cornea polarity, the homologous F8 electrode site demonstrates a negative phase reversal from the retina. Note the two lateral eye movements at the end of second 1 and during second 4 in Figure 1. The positive phase reversals noted at the F8 derivation is due to the proximity of the cornea. The homologous F7 electrode site is negative due to the conjugate effect from the retina. However, because vertical eye movements are often the source of confusion, bilateral infraorbital electrodes referred to the ipsilateral ear as a reference may better represent the eye as a dipole and demonstrate phase reversals that are out-of-phase with cerebral activity when due to eye movements (see above). Eye move ment monitors may be added during the recording if difficulty differ entiating cerebral function from extracerebral origin becomes desirable. The contractions are time locked to the photic stimulation and begin and cease commensurate with the flash, although there is often a brief delay between the flash and the myogenic potentials that appear. Spikes occur with rapid eye movements to the left, right, left, and right in the 4th to 6th second. Each rapid eye movement is associated with a positive potential represented by a phase reversal on eye deviation to the side of the lateral rectus contracting. Oz has continuous single electrode artifact, and a bifrontal burst of muscle artifact is seen in second 3 to 4.
Order avanafil 100 mg with visa
Multiple courses of pharmacological treatments It is used to treat overdose and treatment may be needed for the counter the effects of the drug addiction impotence after prostate surgery order avanafil on line, although its use for patient to make a full recovery. Often barbiturate and benzodiazepine abuse occurs in conjunction with the abuse of other drugs, such as alcohol or cocaine. In such cases of polydrug abuse, the treatment approach should address the multiple addictions. Treating addiction to prescription stimulants Treatment of addiction to prescription stimulants, such as Adderall and Concerta, is poor adherence and tolerability by can reduce cravings and is well based on behavioral therapies patients. It and benzodiazepine addiction (These vouchers can be exchanged has been used successfully for is sparse; however, addicted for items that promote healthy more than 40 years to treat heroin patients should undergo medically living. Their dilemma stems from the potential risks involved with long-term treatment, such as the development of drug tolerance (and the need for escalating doses), hyperalgesia (increased pain sensitivity), and addiction. Patients themselves may even be reluctant to take an opioid medication prescribed to them for fear of becoming addicted. This variability is the result of differences in treatment duration, insuffcient research on long-term outcomes, and disparate study populations and measures used to assess abuse or addiction. To mitigate addiction risk, physicians should screen patients for potential risk factors, including personal or family history of drug abuse or mental illness. Monitoring patients for signs of abuse is also crucial, and yet some indicators can signify multiple conditions, making accurate assessment challenging. Early or frequent requests for prescription pain medication reflls, for example, could represent illness progression, the development of drug tolerance, or the emergence of a drug problem. The development of effective, nonaddicting pain medications is a public health priority. A growing elderly population and an increasing number of injured military only add to the urgency of this issue. Researchers are exploring alternative medications that can alleviate pain but have less abuse potential. More research is needed to better understand effective chronic pain management, including identifying factors that predispose some patients to addiction and developing measures to prevent abuse. Antagonists prevent the natural (or abused) substance from activating its Polydrug Abuse: the abuse of two or more drugs at receptor. Respiratory Depression: Slowing of respiration Central Nervous System: the brain and spinal cord. Comorbidity: the occurrence of two disorders or Stimulants: A class of drugs that enhances the illnesses in the same person, also referred to as activity of monamines (such as dopamine) in the co-occurring conditions or dual diagnosis. Patients brain, increasing arousal, heart rate, blood pressure, with comorbid illnesses may experience a more and respiration, and decreasing appetite; includes severe illness course and require treatment for each some medications used to treat attention-defcit or all conditions. This is often the frst step in drug a drug are required to produce the same effect abuse treatment. Withdrawal: Symptoms that occur after chronic use Narcolepsy: A disorder characterized by of a drug is reduced abruptly or stopped. Norepinephrine: A neurotransmitter present in the brain and the peripheral (sympathetic) nervous system; and a hormone released by the adrenal glands. Norepinephrine is involved in attention, responses to stress, and it regulates smooth muscle contraction, heart rate, and blood pressure. Emergency department visits involving nonmedical use of selected prescription drugs McCabe, S. Medical use, Unintentional Drug Poisoning in the United illicit use, and diversion of abusable prescription States. The use of abusable prescription of results from the National Survey on Drug Use drugs: the role of gender. Monitoring the Future: National Survey of Ritalin: A comparison with amphetamines Results on Drug Use, Overview of Key Findings and cocaine. At birth, active sleep is approximately 50% of total sleep and declines over the first 2 years to approximately 20% to 25%. Slow-wave sleep (stages 3 and 4) decreases across adolescence by 40% from preteen years and continues a slower decline into old age, particularly in men and less so in women. In this chapter, the normal young adult sleep pattern is described as a working baseline pattern. Normative changes due to aging and other factors are described with that background in mind. Several major sleep disorders are highlighted by their differences from the normative pattern. Sleep Definitions According to a simple behavioral definition, sleep is a reversible behavioral state of perceptual disengagement from and unresponsiveness to the environment. It is also true that sleep is a complex amalgam of physiologic and behavioral processes. Sleep is typically (but not necessarily) accompanied by postural recumbence, behavioral quiescence, closed eyes, and all the other indicators one commonly associates with sleeping. These behaviors can include sleepwalking, sleeptalking, teeth grinding, and other physical activities. This manual recommends alterations to recording methodology and terminology that the Academy will demand of clinical laboratories in the future. Although specification of arousal, cardiac, movement, and respiratory rules appear to be value added to the assessment of sleep-related events, the new rules, terminology, and technical specifications for recording and scoring sleep are not without controversy. The current chapter uses the traditional terminology and definitions, upon which most descriptive and [17] experimental research has been based since the 1960s. Although these are somewhat trivial changes, changes in nomenclature can result in confusion when attempting to compare to previous literature and established data sets and are of concern for clinicians and investigators who communicate with other fields. The rationale for the change is that the frontal placements pick up more slow-wave activity during sleep. Within sleep, two separate states have been defined on the basis of a constellation of physiologic parameters. The four electroencephalogram tracings depicted here are from a 19-year-old female volunteer. Each tracing was recorded from a referential lead (C3/A2) recorded on a Grass Instruments Co. On the second tracing, the arrow indicates a K-complex and the underlining shows two sleep spindles. The distinction of tonic versus phasic is based on short-lived events such as eye movements that tend to occur in clusters separated by episodes of relative quiescence. This fundamental principle of normal human sleep reflects a highly reliable finding and is important in considering normal versus pathologic sleep. Definition of Sleep Onset the precise definition of the onset of sleep has been a topic of debate, primarily because there is no single measure that is 100% clear-cut 100% of the time. To begin a consideration of this issue, let us examine the three basic polysomnographic measures of sleep and how they change with sleep onset. Note that the electroencephalographic pattern changes from wake (rhythmic alpha) to stage 1 (relatively low-voltage, mixed-frequency) sleep twice during this attempt to fall asleep. Different functions, such as sensory awareness, memory, self-consciousness, continuity of logical thought, latency of response to a stimulus, and alterations in the pattern of brain potentials all go in parallel in a general way, but there are exceptions to every rule. One might not always be able to pinpoint this transition to the millisecond, but it is usually possible to determine the change reliably within several seconds.
Avanafil 50mg low cost
The aim of this study was to investigate the role of excision repair cross Petersburg population erectile dysfunction causes pdf avanafil 100mg low price. A variety of materials are used for filling and the bonding of restoration ma terials to the tooth cavity. Particularly, amalgam is known for its toxicity po tential as it releases mercury and shown to be genotoxic as well. The prevalence of po Cardiovascular diseases are the leading cause of premature death in the lymorphisms in these genes can vary considerably by ethnicity, so the im worldwide adults. Overall prevalence of hypertension in Morocco is there portance of specific polymorphisms may be very different in different eth about 33. The significant association of rs7216389 polymor morphisms of these genes and the level of blood pressure. The homozygous rs7216389 T/T genotype may be a risk factor for aldosterone system. Research Institute of Obstetrics and Gynecology, Saint-Petersburg, Russian Federation, In the literature, more than 200 different genodermatosis or hereditary 3The D. The goal of the study was to disclose rent systems of skin covers: skin, hair, nails, glands. We detect previously known mutation in A genome wide survey of copy number variations in population of 7 exon of the hHb6 gene. Department of Human and Medical Genetics, Faculty of Medicine, Vilnius University, Vilnius, Lithuania. Methods: A healthy Familial idiopathic steroid-resistant nephrotic syndrome is characterized by a cohort from population of Lithuanian (n=150) were genotyped using the nephrotic syndrome with often early onset. The nephrotic syndrome is defined by severe proteinuria 166 Mb and accounting for 5. The R138Q mutation has been reported as recurrent luable resources for studying human genome diversity and its association mutation in patients with steroid-resistant nephrotic syndrome, especiallly fa with disease. Determine the prevalence of this mutation in Moroccan patients with steroid Jakaitiene: None. Provide genetic counseling to families and allow early treatment of children, to J16. Ciullo; sporadic cases with consanguinity, Institute of Genetics and Biophysics A. Ait Ouamar: this segment faces the entire cardiac output volume coming from the left None. The weakening of the aortic wall and loss of elasticity could produce a dilatation and degenerate into a dissection and rupture, be coming a potentially life-threatening disease. Analysis of genetic distances between populations of the Volga-Ural Sri Ramachandra Medical college and Research Institute, Chennai, India. Kitsiou-Tzeli; 1Department of Medical Genetics, Medical School, University of Athens, Athens, Greece, R. As a primary investigation, ka situation makes it possible to study the relationship between pedigree-size ryotyping, fragile X testing and metabolic screening have been performed. Najmabadi: 1Fazeli-Sanati genetic laboratory, Tehran, Islamic Republic of Iran, 2Tehran university, None. Tehran, Islamic Republic of Iran, 3Fazeli-Sanati genetic laboratory, National institute for genetic engineering and biotechnology, Tehran, Islamic Republic of Iran. After 2 or 3 hours in total Unusual splicing mutations in patients with neurofibromatosis type 1 darkness, the normal color of the fundus returns. Carrier screening of the identified mutation in the family was also perfor In 9 cases (64, 3%) these mutations involved consensus splicing regulatory med with sequence analysis of exon 4 in all family members. Sequencing sequences, in remaining 5 patients (35, 7%) non-typical splicing pathogenic analysis showed a homozygote deletion C, in codon 96 (in exon 4). In one of them skipping of exon 29 or 29 and 30 of patients were heterozygote for mentioned deletion as well. Sahahzadeh-Fazeli: nucleotide substitutions affecting exons 7, 10b and 24 that would normally None. Department of Genetics, United Laboratories, Tartu University Hospital, Tallinn, Estonia. The ability to diagnose these disorders soon after birth is very important clinical issue with its different aspects re lating to diagnosis, treatment and sex of rearing. Zinchenko1; 1 karyotypes and genetic syndromes where ambiguous genitalia is one of the Research Centre for Medical Genetics, Russian Academy of Medical Sciences, Moscow, Russian Federation, 2Burdenko Neurosurgery Institute, Moscow, Russian Federation. During 2007-2012 four babies were consulted as newborns due to lar schwannomas), meningiomas, spinal tumors, peripheral nerve tumors, ambiguous genitalia in neonatal period. Mutation analysis was performed by direct sequencing using Identifying the underlying cause of is necessary for the individual prognosis 17 primers pairs covering the coding sequences and their intron-exon junc and genetic counselling of the family. Overall, we found 16 mutations in 15 pati ents (as in lymphocytes and in tumors): one large deletion (including exon E. Kovacs2; 12nd Department of Pediatrics, Comenius University Medical School and University T. Case report:A 10-years-old girl with acute exacerbation of chronic pancrea In this study, we analysed aneuploidy rates of 45 spontaneous miscarriage titis (2nd attack) was admitted to the hospital. For this reason, we suggest if the re Conclusion: We present a girl with two genetically determined disorders. All children have no other brothers or sisters; cystic fibrosis patients, aged between 6 and 12 years old. All the members of the family that have availability to spend a period of 4 weeks at the Romanian National Cystic the disease presented a precocious onset, with a progressive glomerulone Fibrosis Center, patients were divided in 2 groups. They have renal biopsy for a proper diagnosis in these days and we and nutritional counselling; and Control group (9 patients) who returned start a suitable genetic counseling for their family potential offspring. Patients were counseling started with genetic consult and psychological sessions, indivi evaluated, at baseline and at the end of the intervention period in regard dual and with all family members. The cor Results: At the end of the study we observed a significant increase of skeletal rect diagnose followed by a proper counseling is their chance to improve muscle mass (from 19. One month intervention did not influence significantly the patients in the Control group. Kuskucu1; tients belonging to two Tunisian unrelated families and manifesting severe 1Yeditepe University Medical School, Department of Medical Genetics, Istanbul, Turkey, phenotype. Homozygosity by descent analysis was carried out using two mi 2Yeditepe University Medical School, Department of Gynecology & Obstetrics, Istanbul, crosatellite markers: D6S1582 and D6S271. Bioinformatic tools revealed abolition of the Interventions for prenatal diagnostic purposes and spontaneous miscar donor splice site. Combined screening in the 1st and 2nd trimesters of pregnancy, compara tive analysis. Azaiez: 309 women 9-13 and 16-22 weeks of pregnancy are surveyed using nonin None. Therefore, based on the results of the analysis, the advantages of in factors involoved Additionally, we aim to find similarity and different views spection in early times of pregnancy were identified. Results were compared and scored and parents comments methods of prenatal diagnostics in the I trimester of pregnancy.
Purchase avanafil in united states online
In the characteristic schizo phrenic disturbance of thinking erectile dysfunction definition generic 100mg avanafil amex, peripheral and irrelevant features of a total concept, which are inhibited in normal directed mental activity, are brought to the fore and utilized in place of those that are relevant and appropriate to the situation. Thus thinking becomes vague, elliptical, and obscure, and its expression in speech sometimes incomprehensible. Breaks and interpolations in the train of thought are frequent, and thoughts may seem to be withdrawn by some outside agency. Ambivalence and disturbance of volition may appear as inertia, negativism, or stupor. The onset may be acute, with seriously disturbed behaviour, or insidious, with a gradual development of odd ideas and conduct. The course of the disorder shows equally great variation and is by no means inevitably chronic or deteriorating (the course is specified by five-character categories). In a proportion of cases, which may vary in different cultures and populations, the outcome is complete, or nearly complete, recovery. The sexes are approximately equally affected but the onset tends to be later in women. Diagnostic guidelines the normal requirement for a diagnosis of schizophrenia is that a minimum of one very clear symptom (and usually two or more if less clear-cut) belonging to any one of the groups listed as (a) to (d) above, or symptoms from at least two of the groups referred to as (e) to (h), should have been clearly present for most of the time during a period of 1 month or more. Conditions meeting such symptomatic requirements but of duration less than 1 month (whether treated or not) should be diagnosed in the first instance as acute schizophrenia-like psychotic disorder (F23. Symptom (i) in the above list applies only to the diagnosis of Simple Schizophrenia (F20. Viewed retrospectively, it may be clear that a prodromal phase in which symptoms and behaviour, such as loss of interest in work, social activities, and personal appearance and hygiene, together with generalized anxiety and mild degrees of depression and preoccupation, preceded the onset of psychotic symptoms by weeks or even months. Because of the difficulty in timing onset, the 1-month duration criterion applies only to the specific symptoms listed above and not to any prodromal nonpsychotic phase. The diagnosis of schizophrenia should not be made in the presence of extensive depressive or manic symptoms unless it is clear that schizophrenic symptoms antedated the affective disturbance. If both schizophrenic and affective symptoms develop together and are evenly balanced, the diagnosis of schizoaffective disorder (F25. Schizophrenia should not be diagnosed in the presence of overt brain disease or during states of drug intoxication or withdrawal. Similar disorders developing in the presence of epilepsy or other brain disease should be coded under F06. Pattern of course the course of schizophrenic disorders can be classified by using the following five-character codes: F20. The clinical picture is dominated by relatively stable, often paranoid, delusions, usually accompanied by hallucinations, particularly of the auditory variety, and perceptual disturbances. Disturbances of affect, volition, and speech, and catatonic symptoms, are not prominent. Examples of the most common paranoid symptoms are: (a)delusions of persecution, reference, exalted birth, special mission, bodily change, or jealousy; (b)hallucinatory voices that threaten the patient or give commands, or auditory hallucinations without verbal form, such as whistling, humming, or laughing; (c)hallucinations of smell or taste, or of sexual or other bodily sensations; visual hallucinations may occur but are rarely predominant. Thought disorder may be obvious in acute states, but if so it does not prevent the typical delusions or hallucinations from being described clearly. Affect is usually less blunted than in other varieties of schizophrenia, but a minor degree of incongruity is common, as are mood disturbances such as irritability, sudden anger, fearfulness, and suspicion. The course of paranoid schizophrenia may be episodic, with partial or complete remissions, or chronic. In chronic cases, the florid symptoms persist over years and it is difficult to distinguish discrete episodes. Diagnostic guidelines the general criteria for a diagnosis of schizophrenia (see introduction to F20 above) must be satisfied. In addition, hallucinations and/or delusions must be prominent, and disturbances of affect, volition and speech, and catatonic symptoms must be relatively inconspicuous. Delusions can be of almost any kind but delusions of control, influence, or passivity, and persecutory beliefs of various kinds are the most characteristic. It is important to exclude epileptic and drug-induced psychoses, and to remember that persecutory delusions might carry little diagnostic weight in people from certain countries or cultures. The mood is shallow and inappropriate and often accompanied by giggling or self-satisfied, self-absorbed smiling, or by a lofty manner, grimaces, mannerisms, pranks, hypochondriacal complaints, and reiterated phrases. There is a tendency to remain solitary, and behaviour seems empty of purpose and feeling. This form of schizophrenia usually starts between the ages of 15 and 25 years and tends to have a poor prognosis because of the rapid development of "negative" symptoms, particularly flattening of affect and loss of volition. Hebephrenia should normally be diagnosed for the first time only in adolescents or young adults. The premorbid personality is characteristically, but not necessarily, rather shy and solitary. For a confident diagnosis of hebephrenia, a period of 2 or 3 months of continuous observation is usually necessary, in order to ensure that the characteristic behaviours described above are sustained. For reasons that are poorly understood, catatonic schizophrenia is now rarely seen in industrial countries, though it remains common elsewhere. These catatonic phenomena may be combined with a dream-like (oneiroid) state with vivid scenic hallucinations. Transitory and isolated catatonic symptoms may occur in the context of any other subtype of schizophrenia, but for a diagnosis of catatonic schizophrenia one or more of the following behaviours should dominate the clinical picture: (a)stupor (marked decrease in reactivity to the environment and in spontaneous movements and activity) or mutism; (b)excitement (apparently purposeless motor activity, not influenced by external stimuli); (c)posturing (voluntary assumption and maintenance of inappropriate or bizarre postures); (d)negativism (an apparently motiveless resistance to all instructions or attempts to be moved, or movement in the opposite direction); (e)rigidity (maintenance of a rigid posture against efforts to be moved); (f)waxy flexibility (maintenance of limbs and body in externally imposed positions); and (g)other symptoms such as command automatism (automatic compliance with instructions), and perseveration of words and phrases. In uncommunicative patients with behavioural manifestations of catatonic disorder, the diagnosis of schizophrenia may have to be provisional until adequate evidence of the presence of other symptoms is obtained. It is also vital to appreciate that catatonic symptoms are not diagnostic of schizophrenia. A catatonic symptom or symptoms may also be provoked by brain disease, metabolic disturbances, or alcohol and drugs, and may also occur in mood disorders. Includes: catatonic stupor schizophrenic catalepsy schizophrenic catatonia schizophrenic flexibilitas cerea 81 F20. Diagnostic guidelines this category should be reserved for disorders that: (a)meet the general criteria for schizophrenia; (b)either without sufficient symptoms to meet the criteria for only one of the subtypes F20. Some schizophrenic symptoms must still be present but no longer dominate the clinical picture. These persisting schizophrenic symptoms may be "positive" or "negative", though the latter are more common. It is uncertain, and immaterial to the diagnosis, to what extent the depressive symptoms have merely been uncovered by the resolution of earlier psychotic symptoms (rather than being a new development) or are an intrinsic part of schizophrenia rather than a psychological reaction to it. They are rarely sufficiently severe or extensive to meet criteria for a severe depressive episode (F32. Diagnostic guidelines the diagnosis should be made only if: (a)the patient has had a schizophrenic illness meeting the general criteria for schizophrenia (see introduction to F20 above) within the past 12 months; (b)some schizophrenic symptoms are still present; and (c)the depressive symptoms are prominent and distressing, fulfilling at least the criteria for a depressive episode (F32. Diagnostic guidelines 82 For a confident diagnosis, the following requirements should be met: (a)prominent "negative" schizophrenic symptoms, i. Includes: chronic undifferentiated schizophrenia "Restzustand" schizophrenic residual state F20. Delusions and hallucinations are not evident, and the disorder is less obviously psychotic than the hebephrenic, paranoid, and catatonic subtypes of schizophrenia. With increasing social impoverishment, vagrancy may ensue and the individual may then become self-absorbed, idle, and aimless. Diagnostic guidelines Simple schizophrenia is a difficult diagnosis to make with any confidence because it depends on establishing the slowly progressive development of the characteristic "negative" symptoms of residual schizophrenia (see F20. There is no dominant or typical disturbance, but any of the following may be present: (a)inappropriate or constricted affect (the individual appears cold and aloof); (b)behaviour or appearance that is odd, eccentric, or peculiar; (c)poor rapport with others and a tendency to social withdrawal; (d)odd beliefs or magical thinking, influencing behaviour and inconsistent with subcultural norms; (e)suspiciousness or paranoid ideas; (f)obsessive ruminations without inner resistance, often with dysmorphophobic, sexual or aggressive contents; (g)unusual perceptual experiences including somatosensory (bodily) or other illusions, depersonalization or derealization; (h)vague, circumstantial, metaphorical, overelaborate, or stereotyped thinking, manifested by odd speech or in other ways, without gross incoherence; (i)occasional transient quasi-psychotic episodes with intense illusions, auditory or other hallucinations, and delusion-like ideas, usually occurring without external provocation. There is no definite onset and its evolution and course are usually those of a personality disorder. It is more common in individuals related to schizophrenics and is believed to be part of the genetic "spectrum" of schizophrenia. Diagnostic guidelines this diagnostic rubric is not recommended for general use because it is not clearly demarcated either from simple schizophrenia or from schizoid or paranoid personality disorders. If the term is used, three or four of the typical features listed above should have been present, continuously or episodically, for at least 2 years. A history of schizophrenia in a first-degree relative gives additional weight to the diagnosis but is not a prerequisite. They are probably heterogeneous, and have uncertain relationships to schizophrenia.
Discount avanafil line
To treat this ved erectile dysfunction treatment cheap 100mg avanafil otc, access was first achieved via the right common femoral artery, and the ipsilateral hypogastric artery was catheterized with a diagnostic catheter and 035 wire. Various contrast injec tions showed that an iliac-to-lumbar collateral was sup plying the endoleak. Three 2-mm X 4-cm soft Ruby Coils were deployed distally, fol lowed by a 3-mm X 15-cm soft Ruby Coil to completely occlude the smaller feeding collateral (Figure 1). Three 8-mm X 60-cm coils were collateral was successfully visualizing the aneurysm sac and deployed into the aneurysm sac, efficiently filling the embolized. Only four addi tional soft coils were required to densely occlude the entire lumbar collateral. A run was then performed and showed complete Angiography was then performed showing that the high occlusion (Figure 3). Jugular access was achieved, and a 6-F long sheath was delivered into the left gonadal vein. A contrast injection was performed showing mul automatically, without catheterizing the vessel (Figure 3). Distal coil are easily visualized when the catheter tip is buried within a coil mass. He subsequently devel ing, continued filling of the false lumen was observed oped a large 6-cm from the celiac trunk and L2 and L3 lumbar vessels with infrarenal abdomi aneurysmal expansion (Figure 1). Additionally, advanced through the true lumen of the aorta from an endograft was a femoral approach. Long, large-diameter Ruby system (Medtronic), completely occluding the false lumen Coils were deployed, embolizing the large false lumen proximally. To treat the aneurysm, we elected to embolize both inflow and outflow vessels and the aneu rysm sac. Upon accessing the proximal splenic artery, angiography was performed and showed a high-flow tor tuous vessel (Figure 1). Each year, approximately 6 million people in the United States are treated with the oral anticoagulant Figure 1. Soft coils pack more densely, creating cross-sectional this medical therapy is severe internal bleeding. However, Despite resuscitative measures and efforts to reverse anti many conventional fibered coils rely on the coil fibers to coagulation, the patient remained hemodynamically unsta promote in vivo thrombus formation, and patients might ble, necessitating emergent angiography and embolization. Selective catheterization of the superior mesenteric Reversal of anticoagulation may be contraindicated in artery demonstrated active extravasation from a terminal some cases, such as in patients with newly placed coronary, branch arising from the right colic artery (Figure 2). Management of antithrombotic therapy in patients undergoing invasive mass, and complete vessel obliteration can be achieved with procedures. Distal bleed visualized in the packing immediately stopped flow within cessation of bleeding. Disclaimer: the opinions and clinical experiences presented herein are for informational purposes only. Individual results may vary depending on a variety of patient specific attributes. Where To Obtain Additional Information For additional information on the Emergency Severity Index, Version 4, please visit The Author owns the copyright, which is on file with the United States Copyright Office. The Author hereby assures physicians and nurses that use of the Algorithm as explained in these two works by health care professionals or physicians and nurses in their practices is permitted. Each professional user of these two works is granted a royalty-free, non-exclusive, non-transferable license to use the Algorithm in their own clinical practices in accordance with the guidance in these two works provided that the Algorithm is not changed in any way. The Algorithm has been rigorously tested and found to be both reliable and valid, as described in the research references included in these two works. However, the Author and the Agency for Healthcare Research and Quality require that the implementation and use of the Algorithm be conducted and completed in accordance with the contents of these two works using the professional judgment of authorized physicians or nurses and staff directed and supervised by them. The Author and the Agency for Healthcare Research and Quality disclaim any and all liability for adverse consequences or for damages that may arise out of or be related to the professional use of the Algorithm by others, including, but not limited to , indirect, special, incidental, exemplary, or consequential damages, as further set forth below. Note: the Authors and the Agency for Healthcare Research and Quality have made a good faith effort to take all reasonable measures to make these two works accurate, up-to-date, and free of material errors in accord with clinical standards accepted at the time of publication. Users of these two works are encouraged to use the contents for improvement of the delivery of emergency health care. Any practice described in these two works should be applied by health care practitioners in accordance with professional judgment and standards of care used in regard to the unique circumstances that may apply in each situation they encounter. The Authors and the Agency for Healthcare Research and Quality cannot be responsible for any adverse consequences arising from the independent application by individual professionals of the materials in these two works to particular circumstances encountered in their practices. We hope that you find this tool useful in your ongoing efforts to improve the quality of care provided by your emergency department. The group agreed that this was crucial to preserving the reliability and validity of the tool. Pediatric validation research led to the addition of a new pediatrics chapter to this edition. Successful implementation of this system is accomplished by committing significant resources during training and implementation. Triage nurses also need education in institution-specific triage policies and protocols. For example, hospitals may develop policies regarding which types of patients can be triaged to fast-track. Triage protocols may also be developed, such as giving acetaminophen for fever, or ordering ankle films for patients who meet specified criteria. Since in the United States 2000, there has been a trend toward standardization the purpose of triage in the emergency department of triage acuity scales that have five levels. The triage) leaves the patient at risk for deterioration task force published a second paper in 2005 and while waiting. Clear definitions believed that a principal role for an emergency of time to physician evaluation are an integral part department triage instrument is to facilitate the of both algorithms. Introduction to the Emergency Severity Index: A Research-Based Triage Tool of these constructs. Inter-rater reliability is a after implementation of the system into triage measure of reproducibility: will two different nurses practice at seven hospitals in the Northeast and rate the same patient with the same triage acuity Southeast. The study the accuracy of the rating system and assesses how results indicated substantial inter-rater reliability well the system measures what it is intended to with kappa statistics ranging from 0. If many high acuity patients were discharged home, the Researchers have also compared inter-rater reliability triage system is most likely not valid. Inter-rater facilitate meaningful comparisons of case mix reliability between the research nurse and the between hospitals. Results using kappa statistics a survey of nursing staff at the two original can range from 0 (no agreement) to 1 (perfect university teaching hospitals, responses to the agreement). Inter to discriminate patient acuity and hospitalization rater reliability for written case scenarios was 0. Overall inter-rater reliability Center conducted a survey of 935 persons who was excellent (weighted kappa=. Good inter 2 patients can be taken directly to the treatment area and intra-rater reliability (weighted kappas of. Introduction to the Emergency Severity Index: A Research-Based Triage Tool headache treatment.
Cheap avanafil 100 mg otc
Dr Neelam Dhingra Coordinator Blood Transfusion Safety 4 Policy recommendations 1 Each country should establish a national system for blood donor selection for the donation of blood or blood components impotence of organic origin 60784 purchase 200mg avanafil mastercard. It should build and maintain a pool of safe, voluntary non-remunerated blood donors and take all necessary steps to ensure that the products derived from donated blood are effcacious for the recipient, with a minimal risk of any infection that could be transmitted through transfusion. All prospective blood donors should therefore be assessed for their suitability to donate blood, on each occasion of donation. The purpose of blood donor selection is to: Protect donor health and safety by collecting blood only from healthy individuals Ensure patient safety by collecting blood only from donors whose donations, when transfused, will be safe for the recipients Identify any factors that might make an individual unsuitable as a donor, either temporarily or permanently Reduce the unnecessary deferral of safe and healthy donors Ensure the quality of blood products derived from whole blood and apheresis donations Minimize the wastage of resources resulting from the collection of unsuitable donations. In addition, at least 13 million prospective donors are deferred from donating blood due to anaemia, existing medical conditions or the risk of infections that could be transmitted through transfusion (9). The scale of these discards and deferrals highlights the need for effective blood donor selection to minimize the unnecessary deferral of suitable donors, and the donation of blood by unsuitable donors that subsequently has to be discarded; this will reduce the wastage of resources, including donor and staff time, consumables and screening tests, and also avoid needless discomfort to donors. Signifcant variations have been observed between countries in the extent to which national donor selection criteria are defned, prospective donors are assessed and the quality and effectiveness of the donor selection process are monitored. In some countries, national systems of blood donor selection are not well-developed and donor selection criteria are not clearly defned or applied uniformly. This may result in blood being collected from donors who have not been properly assessed for their suitability to donate; this may affect their health and pose a higher risk of transmission of infections through transfusion. In many countries, donor selection criteria are still based on tradition and customary practice rather than on evidence (10, 11) and criteria from one country are often adopted in other countries without due consideration of the profles 16 of the general and potential donor populations, the prevailing epidemiology of infections and diseases, local culture and available resources. Some countries take a highly precautionary approach to the selection of donors for the safety of blood products, donors and patients. Policies for donor selection should take into account the need for a balance between the safety and suffciency of the blood supply and available resources (11, 12, 13). However, there are relatively few internationally-recognized guidelines on blood donor selection (Annex 1) and all of these have been developed to address the needs of specifc regions or countries. There is therefore a need for global guidance on the development of systems and criteria for blood donor selection that could then be adapted at national level. Objectives these guidelines are intended for use in countries which have not yet established national systems for blood donor selection or which are in the process of developing or revising donor selection guidelines and criteria. The specifc objectives are to: 1 Provide guidance on the measures needed to develop and implement effective systems for assessing the suitability of individuals to donate blood. The donor selection criteria recommended in these guidelines apply to donors of whole blood, red cells, platelets, plasma and other blood components, donated as whole blood or through apheresis, including plasma for fractionation. These include a) criteria that have worldwide applicability and should be applied uniformly, and b) criteria that require local adaptation in the light of epidemiological data, demography, the health of the population, the screening and confrmatory tests performed and the available technology. Whilst these guidelines are designed to promote best practice in blood transfusion services to ensure the collection of donations from the lowest risk donors possible, consideration should always be given to the issue of suffciency, balancing any risk of infection against the risk of blood shortages resulting from the development of too stringent national guidelines. Infectious risks are not the same in all countries, or even within individual countries, and it is crucial that selection guidelines are developed according to the circumstances and needs of each country. It identifed three key questions to be addressed: 1 What are the components of an effective national system for assessing the suitability of prospective donors to donate blood As these guidelines have been developed particularly for use in countries that have not yet established national systems for blood donor selection, the literature search strategy was specially designed to collect literature from low and middle income countries. A preliminary screen by review of titles was carried out by the searcher to eliminate obviously irrelevant and duplicate citations. This formed the basis for the formulation of recommendations on criteria for the acceptance and deferral of prospective blood donors. It is recognized that there is a paucity of high quality evidence on which to base decisions on blood donor selection. Many long-established donor selection criteria are based on medical knowledge of the disease process and human physiology, the haemodynamic effect of blood donation and the potential for harm to either the donor or the recipient. In general, acceptance criteria specify conditions in which there is no or minimal risk to donor or recipient, based either on published evidence of safety from observational studies or on general medical principles. Deferral criteria are based almost entirely on general principles aimed at minimizing any risk to the donor or recipient. Evidence is rarely available because observational studies of blood donation in many such conditions would be unethical. Given the paucity of the evidence on donor selection criteria, formal assessment of the quality of evidence to support the recommendations was undertaken only for three topics, because of their controversial nature, discrepancies between international guidelines or the potential impact of a change of practice on the blood donor base, i. Summaries of evidence tables were made to assist in the development of recommendations on these topics. Where published evidence is lacking, recommendations on donor selection criteria are based on international best practice and the medical knowledge and expertise of members of the guideline development group and external review group. In conditions where emerging evidence suggests that deferral criteria may be relaxed, a precautionary approach is recommended until good evidence of safety becomes available. Part 1 (Sections 2 and 3) addresses the requirements for an effective national system for blood donor selection; policy recommendations are provided on pp. Review and updating of the guidelines It is anticipated that the guidelines will remain valid until 2017. National health authorities and blood transfusion services are responsible for ensuring that a national system is in place for the selection of all blood donors through an assessment of their suitability to donate blood. The national system for blood donor selection should include: National policy and legislative framework National guidelines and criteria on blood donor selection Public information and donor education Suitable infrastructure and facilities Adequate fnancial and human resources Quality system, including standard operating procedures, documentation and records Donor haemovigilance Monitoring and evaluation. The national blood policy should be supported and enforced by a legislative and regulatory framework and implemented through national guidelines. The legislative framework should defne the fundamental principles and ethics of blood donation and donor selection. Blood donors have a responsibility to self-defer if they are aware of having been exposed to any risk of an infection or a known health condition or treatment that could infuence their suitability to donate blood. Blood donors also have the right to withdraw at any stage of the donation process. Patients have a right to be protected from avoidable adverse effects of transfusion. Thus, while anyone may offer to become a blood donor, no one has the right to donate blood (20, 21). The formulation and implementation of donor selection criteria will protect the health of blood donors and the recipients of transfusion. It will also help to maintain and raise standards of donor management and care and minimize unnecessary donor deferrals. Guidelines on blood donor selection should be comprehensive, relevant to the local situation and simple to apply in practice. In developing national guidelines, a review of existing international guidelines, relevant literature and best practices would help to identify the medical and scientifc principles underlying donor selection criteria. National guidelines should be based on evidence and risk assessment, taking into account national data on the epidemiology of medical conditions and transfusion-transmissible infections, and risk behaviours (22). It is also important to consider the nutritional and health status of the population and cultural practices. National guidelines and criteria on blood donor selection should comply with national legislative and regulatory requirements and should be reviewed regularly and updated in response to changes in epidemiology, advances in technology, the latest medical and scientifc information and new evidence. Emerging infections and other situations that may infuence donor and patient safety should be monitored and may necessitate the revision and modifcation of donor selection criteria. Donor acceptance and deferral criteria and blood screening procedures have to be balanced to provide optimal safety for both donors and recipients while at the same time ensuring an adequate supply of blood and blood products (23, 24). National health authorities should assess whether, and to what extent, any criteria for donor selection could be relaxed in order to maintain adequate blood supplies in an emergency situation, such as pandemic infuenza. However, any deviation from national guidelines and criteria on blood donor selection should be limited to a defned period in managing the emergency situation (25). Donor questionnaire A donor questionnaire is the key tool in donor selection for assessing donor health and safety and for reducing the risk of transmission of infection, in particular for infections for which no suitable screening tests are available. A standardized donor questionnaire incorporating selection criteria is now widely accepted as being necessary for uniformity and consistency in approach and for ease of implementation in assessing donor suitability. It ensures that the same information is collected systematically about each donor on each occasion of donation and forms the basis for a one-to-one confdential interview with a trained member of staff. By presenting all relevant information in a standard format, a donor questionnaire facilitates decisions on the acceptance or deferral of the donor.