
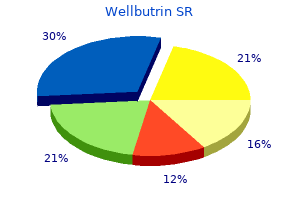
Wellbutrin SR
Order wellbutrin sr with a mastercard
How erative treatment for lumbar disk herniation: the Spine Patient ever anxiety vs depression discount 150 mg wellbutrin sr fast delivery, the results are difcult to interpret. Porchet et al reported results of a retrospective comparative Nov 22 2006;296(20):2451-2459. Spine L1-2, 9 patients at L2-3, 48 patients at L3-4, 86 patients at L4-5 (Phila Pa 1976). The authors concluded that Surgery versus prolonged conservative treatment for sciatica. A 10-year Wenger et al11 described a retrospective case series report follow-up of the outcome of lumbar microdiscec to my. Success rates, including excel year outcome of surgery for lumbar disc herniation: radiograph lent, good, and fair results, were 92. The authors concluded that sequestrec to my alone is a up of patients surgically treated by the far-lateral approach for safe operative modality and should be used whenever possible. Long-term outcome results are as favorable as or better than results afer standard of 104 patients afer lumbar sequestrec to my according to Williams. Lumbar Decompres Future Directions for Research sion Using a Traditional Midline Approach Versus a Tubular Re The work group identifed the following suggestions for future trac to r System Comparison of Patient-Based Clinical Outcomes. Archivos de Neurocien Follow-up of patients included in the studies describing medi cias. Recovery of Future long-term studies of the efects of surgical interventions impaired muscle function in severe sciatica. Recovery of sensory nerve intervertebral lumbar disk prolapse: mid-term results of 22 pa fbres afer surgical decompression in lumbar radiculopathy: tients and literature review. Jan bar discec to my for sciatica: the efects of fragment type and anular 1998;64(1):120-123. Lumbar herniated disc pre function in adjacent nerve roots afer surgery for lumbar disc senting with cauda equina syndrome. Long-term follow-up of herniation: use of quantitative sensory testing in the explora four cases. Outcome analysis in 654 radiculopathy beneft more from microdiscec to my than advice surgically treated lumbar disc herniations. Jun in the short term, although there is no diference in the long 1992;30(6):862-866. The outcome of surgery disc herniation treated either by microdiscec to my, or by intradis for lumbar disc herniation. Magnetic resonance imaging Surgery versus prolonged conservative treatment for sciatica. Interpreting the Spine Patient Outcomes Microdiscec to my for lumbosacral disc herniation and frequency Research Trial. Recurrent disc herniation cutaneous lumbar laser disc decompression: a systematic review and long-term back pain afer primary lumbar discec to my: review of current evidence. Recurrent lumbar resonance imaging afer primary lumbar discec to my: fac to rs disc herniation afer discec to my: Clinical result of repeated associated with recurrent disc herniation and disc height loss. Is there a difference in outcome or complications between different sites of service for the surgical management of a lumbar disc herniation with radiculopathyfi Future Directions for Research Recommendation #2: The work group identifed the following suggestions for future Assuming that the surgical procedure performed is the same, ad studies, which would generate meaningful evidence to assist in ministrative data could be examined to assess complication and further defning the outcomes or complications between difer readmission rates. Comparison of Surgical Outcomes/Complications by Site-of-Service Bibliography Recommendation #1: 1. Ambula to ry surgery Participation in surgical registries would allow for comparison is safe and efective in radicular disc disease. Value of Spine Care What is the cost-effectiveness of surgical treatment options in the management of lumbar disc herniation with radiculopathyfi They were able to track all health niation has been evaluated by several authors using diferent care costs for the study duration and used a standard human methodologies and from diferent perspectives (patient, payer, capital approach to estimate indirect costs. This difculty was a result of a combination of fac to rs in concerning lumbar disc surgery from several studies looking at cluding the relative immaturity of the rating methodology, the microdiscec to my as well as chemonucleolysis and calculated relative inexperience of the committee members in evaluating costs based on hospital reimbursements (a payer perspective cost efectiveness studies, and the diferent methodologies em analysis). This group found that even when indirect costs of per ployed by the authors of the primary studies. Future Directions for Research Ongoing costs were assessed using surveys at follow-up visits Participation in long-term outcome registries could provide regarding medication use, physical therapy, injections, and other meaningful data regarding the cost efectiveness of treatment op interventions. Indirect costs were estimated using a standard tion for patients with radiculopathy from lumbar disc herniation. Cost-Effectiveness of Surgical Treatments References While this analysis captured expenses from the payer and from 1. Socioeconomic predic to rs of Hansson et al2 performed a similar analysis using a prospec baseline disability status among patients with lumbar radicu lopathy. Ninety-two of these workers were treated is safe and efective in radicular disc disease. Spine (Phila Pa with surgery for sciatica due to lumbar disc herniation and the 1976). Increases in lumbosacral injections cohort based on demographic as well as pain diagram and pain in the Medicare population: 1994 to 2001. Sep 1999;52(3):217 of intervertebral disc tissue specimens afer routine cervical and 223; discussion 223-215. Sep 1 sociated injuries Modeling of the 1991 injury cohort from a 2008;33(19):2108-2115. Long-term back pain afer a single-level discec to my for radicu lopathy: incidence and health care cost analysis. Does the surgical approach for lumbar disc herniation with radiculopathy have an effect on the value of treatmentfi Future Directions for Research Participation in long-term outcome registries could provide meaningful data regarding the efect of surgical approach on the value of treatment. Does the site-of-service chosen for surgical management of lumbar disc herniation with radiculopathy affect the value of treatmentfi Future Directions for Research Participation in long-term outcome registries could provide meaningful data regarding the efect of site-of-service on the value of surgical treatment. A complete assessment of quality of individual studies requires critical appraisal of all aspects of the study design. Patients treated one way (eg, cemented hip arthroplasty) compared with a group of patients treated in another way (eg, unce mented hip arthroplasty) at the same institution. Patients treated one way with no comparison group of patients treated in another way. Grades of Recommendation for Summaries or Reviews of Studies A: Good evidence (Level I Studies with consistent fnding) for or against recommending intervention. Additional data care or use of new technologies is the comprehensive literature bases may be searched depending upon the to pic. Torough assessment of the literature is the basis for the review of existing evidence, which will be instrumental to these 2. The medical librarian typi employ a solid search strategy, regardless of the source of the re cally responds to requests and completes the searches within quest. The following parameters are to be provided to research staf to facilitate this search. Spine ated lumbar disc: the outcome afer chemonucleolysis, surgi (Phila Pa 1976). Myelographic versus clinical diagnostics in nonsurgical management of sciatica secondary to a lumbar disc lumbar disc disease. Spine (Phila Pa outcomes of surgical and nonsurgical management of sciatica 1976). Apr 15 taneous endoscopic lumbar discec to my for upper lumbar disc 2005;30(8):927-935.
Buy cheap wellbutrin sr 150 mg on-line
There is a need to think more critically about the relative contribution to mental wellbeing of individual psychological skills the Power Threat Meaning Framework 271 and attributes depression test for social security buy cheap wellbutrin sr online. At the same time, these progressive ideas are, if these documents are taken as typical, undermined by unquestioned assumptions of medicalisation. More mental health services are promised, but the appropriateness of the diagnostic model on which they are based is not open to question or dispute. When compared with physical healthcare, the aim is to have equal access to the most effective and safest care and treatment; equal efforts to improve the quality of care; the allocation of time, effort and resources on a basis commensurate with need; equal status within healthcare education and practice; equally high aspirations for service users; and equal status in the measurement of health outcomes. The mind and body are intrinsically linked on a physiological level (p 12) the silo approach to public health, in which physical health is considered independently of mental health, no longer makes sense (Faculty of Public Health, 2016, p. One of the suggested solutions is the commissioning of liaison psychiatry teams across acute, secure, primary care and community settings, for all ages. It is undoubtedly true that mental health services are seriously under-resourced and underfunded. Breaking down artifcial service barriers between mental and physical health settings and social care is highly desirable. Thus, while the need for parity of esteem in the form of resources in all these areas can be endorsed, it should not be confated with justifying the expansion of the medicalisation of distress, given the striking lack of an evidence-base or achievement of good overall outcomes (Drury, 2014). These developments are particularly unwarranted given, although possibly related to , increasing challenges to medicalisation within mental health services themselves. As we have emphasised throughout this document, psychological and emotional distress is not the same kind of problem as medical illness even if they co-exist, have synergistic effects, and share some common roots arising out of adversities. This is not to deny that useful work happens within these new liaison and consultancy teams, as within any mental health team. It couples the call to integrate mental and physical health with a more emphasis on coercive interventions and less on peer support and trauma-informed care. Independent, voluntary, self-help and survivor-led services While it is beyond the remit of this document to offer an overview of non-statu to ry, voluntary, self-help and survivor-led services and organisations, it is important to note that many of them offer extremely valuable support, which may be based on non-medical and non-diagnostic approaches. Stigma describes negative social attitudes to wards these people, which are often internalised in to a sense of shame and difference. Both are a major barrier to recovery (Corrigan & Kosyluk, 2013; Pyle & Morrison, 2014), and some people describe stigma and discrimination as more disabling than their original diffculties (Schulze & Angermeyer, 2003). However, this approach has consistently been shown to increase, rather than decrease, prejudice, fear and pessimism about recovery (Angermeyer et al. Stigmatising attitudes are less common in low and middle income countries, which may partially account for higher recovery rates there. Service users who espouse biological causal beliefs are less 274 the British Psychological Society, January 2018 optimistic about recovery, make less effort to recover, and/or are more likely to use alcohol to cope (Birchwood et al. Mental health professionals who hold bio-genetic causal beliefs may be less empathic to wards their clients (Lebowitz & Ahn, 2014). This to o, however, has been shown to lead overall to more negative attitudes (Angermeyer et al. Conversely, experimental studies that put forward psychosocial causal explanations have been consistently shown to improve attitudes (Kvaale et al. Some service users have expressed doubts about the messages of anti-stigma campaigns. Its equally signifcant limitations can be traced back to a failure to question, and thus offer genuine alternatives to , the medicalisation of emotional distress with all its consequences. When a human services program takes the step to become trauma-informed, its entire organization, management, and service delivery system is assessed and potentially modifed to include a basic understanding of how trauma affects the life of an individual seeking services. Similar guidelines and practice examples have been developed in British Columbia (Arthur et al. Not everyone in mental health and related services has experienced specifc identifable traumatic events, and conversely, not everyone who has done so will experience lasting damage or need professional support. However, we are all, in some aspects of our lives, subject to the negative impacts of power.
Buy wellbutrin sr 150mg amex
Medical specialist in Internal Medicine anxiety group generic wellbutrin sr 150mg line, Systemic Au to immune Diseases Unit, Hospital Clinico San Cecilio, Granada. Medical Specialist in Rheuma to logy, Hospital Clinico San Borja Arriaran, Universidad de Chile. Medical specialist in Internal Medicine, Hospital Universitario Son Espases, Palma de Mallorca. Assessment and Planning Service of the Canary Health Service, El Rosario, Tenerife. Medical specialist in Family and Community Medicine, Canary Health Service, La Palma. Specialised Care Service, Direc to rate General for Healthcare Services, Canary Health Service, Tenerife. Declaration of interest: All members of the Development Group, as well as those who partici pated in the expert collaboration and external review, made the declaration of interest appearing in Appendix 1. Do early detection and early treatment improve the prognosis and survival of people with systemic lupus erythema to susfi What are the main symp to ms and signs that should make us suspect systemic lupus erythema to susfi What is the validity of labora to ry tests to confrm the diagnosis of systemic lupus erythema to susfi After confrming the diagnosis, what test should be carried out to make an initial evaluation of any patient with systemic lupus erythema to susfi What is the most recommendable clinical moni to ring pro to col for people with systemic lupus erythema to susfi What complementary tests should be carried out on people with systemic lupus erythema to sus, and how often, in moni to ring and control consultationsfi Which are the most effective and cost-effective disease activity biomarkers for moni to r ing systemic lupus erythema to susfi Are the available standardised to ols effective to assess the disease in clinical practicefi What are the analytical or biological markers that can predict a lupus fare or which fac to rs have been associated with an increase in activity of systemic lupus erythema to susfi What non-biological immunosuppressive treatments are effective in extrarenal lupusfi Is the use of anti-malarial drugs indicated in all people with systemic lupus er ythema to susfi What is the effectiveness, cost-effectiveness and safety of these drugs in preventing faresfi Have they got other additional benefcial effects that may justify their generalised usefi What is the recommended dose of glucocorticoids to keep the disease controlled with an assumable risk of adverse effectsfi Which biological therapies are effective and safe in people with systemic lupus erythema to susfi What is the effectiveness and safety of immunoglobulins in treating systemic lupus erythema to susfi What are the complications and adverse effects of the most usual biological and immunosuppressive treatments of systemic lupus erythema to susfi What is the effectiveness and safety of therapeutic apheresis in treating systemic lupus erythema to susfi Which measures are effective to prevent the reactivation of systemic lupus ery thema to susfi Which therapeutic options are effective to help people with asthenia associated with systemic lupus erythema to susfi Which lifestyle-related measures should be advised for people with systemic lu pus erythema to susfi Are structured nursing-based educational programmes addressed to people with systemic lupus erythema to sus effectivefi Which circumstances defne a therapeutic guideline as ineffective/refrac to ry to treatmentfi Under what conditions would induction treatment with mycophenolate afford ad vantages over other drugsfi What induction treatment in lupus nephritis with renal insuffciency should be administeredfi What is the immunosuppressive maintenance treatment of proliferative lupus ne phritisfi What should be the immunosuppressive therapeutic strategy of frst choice for type V lupus nephritisfi What is the usefulness of certain types of au to antibodies for diagnosing neu ropsychiatric complicationsfi Which are the imaging techniques of choice in the diagnostic process of neu ropsychiatric complications of systemic lupus erythema to susfi Should neuropsychological tests be performed in all patients with suspected neu ropsychiatric systemic lupus erythema to susfi When are high-intensity immunosuppressive drugs indicated in people with neu ropsychiatric lupusfi What is the effectiveness, safety and cost-effectiveness of to pical therapies in treating systemic lupus erythema to sus with cutaneous manifestationsfi What types and combinations of antiphospholipid antibodies increase the risk of thrombosis in people with systemic lupus erythema to susfi What preventive and treatment measures should be taken for thrombotic compli cations in people with systemic lupus erythema to sus and antiphospholipid anti bodiesfi How would pregnancy be planned in women with systemic lupus erythema to sus in order to maximise success possibilitiesfi What specifc moni to ring should be carried out and how often in pregnant pa tients with systemic lupus erythema to susfi What preventive measures should be taken for obstetric complications in people with antiphospholipid antibodies Fertility and contraception 50. Are assisted reproduction procedures safe and effcient in systemic lupus erythe ma to susfi Should the cardiovascular risk be evaluated in people with systemic lupus erythema to susfi Is there evidence about specifc cholesterol fgure targets, or can we only transfer those recommended for other high cardiovascular risk pathologies such as diabetesfi In which people with systemic lupus erythema to sus is the use of aspirin indi catedfi Is there evidence that favours the use of certain high blood pressure drugs such as angiotensin blockers, in people with systemic lupus erythema to susfi What is the safety and effcacy of a pneumococcal vaccine in people with sys temic lupus erythema to susfi What are the most frequent types of cancer in people with systemic lupus erythe ma to susfi Should a bone densi to metry be carried out on all people with systemic lupus ery thema to susfi Which measures should be taken to prevent steroid-induced osteoporosis in peo ple with systemic lupus erythema to susfi Well-conducted studies of case control or cohort studies with a very low risk of confounding or bias and a high probability that the relationship is causal. B A volume of scientifc evidence comprised of studies classifed as 2++, directly applicable to the target population of the guideline and that show great consistency between them; or scientifc evidence extrapolated from studies classifed as 1++ or 1+. C A volume of scientifc evidence comprised of studies classifed as 2+, directly applicable to the target population of the guideline and that show great consistency between them; or scientifc evidence extrapolated from studies classifed as 2 ++. D Scientifc evidence of level 3 or 3; or scientifc evidence extrapolated from studies classifed as 2+. The studies classifed as 1 and 2 must not be used in the recommendations preparation process due to their high bias possibility.
150 mg wellbutrin sr
The polymorphic maculopapular rash is generalized and typically includes the palms and soles anxiety stomach problems order wellbutrin sr 150 mg mastercard. This stage also resolves spontaneously without treatment in approximately 3 to 12 weeks, leaving the infected person completely asymp to matic. A variable latent period follows but sometimes is interrupted during the frst few years by recurrences of symp to ms of secondary syphilis. Latent syphilis is defned as the period after infection when patients are seroreactive but demonstrate no clinical manifestations of disease. The tertiary stage of infection occurs 15 to 30 years after the initial infection and can include gumma formation, cardiovascular involvement, or neurosyphilis. The incidence of acquired and congenital syphilis increased dramatically in the United States during the late 1980s and early 1990s but decreased subsequently, and in 2000, the incidence was the lowest since reporting began in 1941. Since 2001, however, the rate of primary and secondary syphilis has increased, primarily among men who have sex with men. Among women, the rate of primary and secondary syphilis has increased since 2005, with a concomitant increase in cases of congenital syphilis. Rates of infection remain disproportionately high in large urban areas and in the southern United States. Primary and secondary rates of syphilis are highest in black, non-Hispanic people and in males compared with females. Congenital syphilis is contracted from an infected mother via transplacental trans mission of T pallidum at any time during pregnancy or possibly at birth from contact with maternal lesions. Among women with untreated early syphilis, as many as 40% of pregnancies result in spontaneous abortion, stillbirth, or perinatal death. The rate of transmission is 60% to 100% during primary and secondary syphilis and slowly decreases with later stages of maternal infection (approximately 40% with early latent infection and 8% with late latent infection). The World Health Organization estimates that 1 million pregnancies are affected by syphilis worldwide. Of these, 460 000 will result in stillbirth, hydrops fetalis, abortion, or perinatal death; 270 000 will result in an infant born preterm or with low birth weight; and 270 000 will result in an infant with stigmata of congenital syphilis. Acquired syphilis almost always is contracted through direct sexual contact with ulcer ative lesions of the skin or mucous membranes of infected people. Relapses of secondary syphilis with infectious mucocutaneous lesions can occur up to 4 years after primary infection. In most cases, identi fcation of acquired syphilis in children must be reported to state child protective services agencies. The incubation period for acquired primary syphilis typically is 3 weeks but ranges from 10 to 90 days. Specimens should be scraped from moist mucocutaneous lesions or aspirated from a regional lymph node. Although such testing can provide defnitive diagnosis, in most instances, serologic testing is necessary. Polymerase chain reaction tests and immunoglob ulin (Ig) M immunoblotting have been developed but are not yet available commercially. Presumptive diagnosis is possible using nontreponemal and treponemal serologic tests. Use of only 1 type of test is insuffcient for diagnosis, because false-positive nontrepone mal test results occur with various medical conditions, and treponemal test results remain positive long after syphilis has been treated adequately and can be falsely positive with other spirochetal diseases. These tests mea sure antibody directed against lipoidal antigen from T pallidum, antibody interaction with host tissues, or both. These tests are inexpensive and performed rapidly and provide semiquantitative results. Occasionally, a nontreponemal test performed on serum sam ples containing high concentrations of antibody against T pallidum will be weakly reactive or falsely negative, a reaction termed the prozone phenomenon. A reactive nontreponemal test result from a patient with typical lesions indicates a presumptive diagnosis of syphilis and the need for treatment. However, any reactive nontreponemal test result must be confrmed by one of the specifc treponemal tests to exclude a false-positive test result. False-positive results can be caused by certain viral infections (eg, Epstein Barr virus infection, hepatitis, varicella, and measles), lymphoma, tuberculosis, malaria, endocarditis, connective tissue disease, pregnancy, abuse of injec tion drugs, labora to ry or technical error, or Whar to n jelly contamination when umbili cal cord blood specimens are used. Treatment should not be delayed while awaiting the results of the treponemal test results if the patient is symp to matic or at high risk of infec tion. A sustained fourfold decrease in titer, equivalent to a change of 2 dilutions (eg, from 1:32 to 1:8), of the nontreponemal test result after treatment usually demonstrates adequate therapy, whereas a sustained fourfold increase in titer from 1:8 to 1:32 after treatment suggests reinfection or relapse. The nontreponemal test titer usually decreases fourfold within 6 to 12 months after therapy for primary or secondary syphilis and usu ally becomes nonreactive within 1 year after successful therapy if the infection (primary or secondary syphilis) was treated early. Some people will continue to have low stable nontreponemal antibody titers despite effective therapy. This serofast state is more common in patients treated for latent or tertiary syphilis. People who have reactive treponemal test results usually remain reactive for life, even after success ful therapy. However, 15% to 25% of patients treated during the primary stage revert to being serologically nonreactive after 2 to 3 years. Treponemal test antibody titers correlate poorly with disease activity and should not be used to assess response to therapy. Treponemal tests also are not 100% specifc for syphilis; positive reactions occur vari ably in patients with other spirochetal diseases, such as yaws, pinta, lep to spirosis, rat-bite fever, relapsing fever, and Lyme disease. The traditional algorithm performs well in identifying people with active infection 1 who require further evaluation and treatment while minimizing false-positive results in low prevalence populations. Quantitative nontreponemal antibody tests are useful in assess ing the adequacy of therapy and in detecting reinfection. In areas of high prevalence of syphilis and in patients considered at high risk 1 of syphilis, a nontreponemal serum test at the beginning of the third trimester (28 weeks of gestation) and at delivery is indicated. For women treated during pregnancy, follow-up serologic testing is necessary to assess the effcacy of therapy. Low-titer false-positive non treponemal antibody test results occasionally occur in pregnancy. When a pregnant woman has a reactive non treponemal test result and a persistently negative treponemal test result, a false-positive test result is confrmed. All infants born to seropositive mothers require a careful exam ination and a nontreponemal syphilis test. The test performed on the infant should be the same as that performed on the mother to enable comparison of titer results. The diagnostic and therapeutic approach to infants being evaluated for congenital syphilis is summarized in Fig 3. Children who are identifed as having reactive serologic tests for syphilis after the neonatal period (ie, 1 month of age and older) should have maternal serologic test results and records reviewed to assess whether they have congenital or acquired syphilis. Algorithm for evaluation and treatment of infants born to mothers with reactive serologic tests for syphilis. For example, a titer of 1:64 is fourfold greater than a titer of 1:16, and a titer of 1:4 is fourfold lower than a titer of 1:16. If a single dose of benzathine penicillin G is used, then the infant must be fully evaluated, full evaluation must be normal, and follow-up must be certain. Treatment Options: (1) Aqueous penicillin G, 50 000 U/kg, intravenously, every 12 hours (1 week of age or younger) or every 8 hours (older than 1 week); or procaine penicillin G, 50 000 U/kg, intramuscularly, as a single daily dose for 10 days. Other causes of elevated values should be considered when an infant is being evaluated for congenital syphilis. Recommendations for penicillin G use and duration of therapy vary, depending on the stage of disease and clinical manifestations. Such patients always should be treated with penicillin, even if desensitization for penicil lin allergy is necessary.
150 mg wellbutrin sr otc
Since the effect of the document is of the adult patient making health care decisions while they had capacity anxiety symptoms in children buy wellbutrin sr 150 mg without a prescription, they are entitled to refuse any medical treatment. However it should be noted that objections to certain forms of treatment can be 3 Note that there are some exceptional situations where medical officers can choose not to follow the directions in an Advance Health Directive. End-of-life care: Guidelines for decision-making about withholding and withdrawing January 2018 29 life-sustaining measures from adult patients made at a previous time, and must also be taken in to consideration in the decision-making process. Health care professionals must first determine if the person still has capacity to accept or refuse treatment at the relevant time. If they have capacity, they can refuse treatment at this point, or they can change their decision and accept treatment. The health professional will therefore need some other form of authority to determine treatment, for example, by obtaining consent from the substitute 66 decision-maker to provide or withhold treatment. The concept of informed consent has been greatly influenced by medical case law and ethical debate in this area. Informed consent involves the medical information patients need to know so they can make decisions, sometimes in advance, about heath matters. Decision-making responsibility is also a key feature of discussions about informed consent. This includes the right to accept or to decline the offer of certain healthcare and to change that decision. Informed consent means that a patient has received the information relevant to them to make an informed decision and they have given permission for the health care service to be provided. In an ethical sense, the agreement by a patient to receive public sec to r health services reflects the end point of a process of engagement in which one or more health practitioners have supported the patient to come to an informed decision to agree to the health care offered. End-of-life care: Guidelines for decision-making about withholding and withdrawing January 2018 31 life-sustaining measures from adult patients clearly understand the information because it is provided in a language or by other means the patient can understand as far as possible, the patient is advised in simple terms of: the diagnosis recommended health care, including the expected benefits, common side effects and alternative health care options the material risks including complications associated with: the recommended health care alternative health care options a decision not to receive the health care offered any significant long term physical, emotional, mental, social, sexual or other expected outcomes the anticipated recovery implications fi the patient has sufficient time to consider and clarify information in order to make an informed decision, taking in to account the context of the clinical situation fi the information provided and the consent given relate to the specific health care provided. There are tensions between what constitutes informed consent for providing medical treatment versus the refusal of medical treatment. Some patients may be competent to consent to minor procedures like vaccinations but not competent to consent to major surgery or the prospect of life-sustaining measures being withheld or withdrawn. Such dilemmas not only create doubt in the process of assessing capacity, it adds to the pressure on doc to rs making assessments to ensure the patient (and his or her substitute decision-maker) has sufficient information to make an informed decision. A patient needs to know what options are available, what the expected outcomes are for each option, and what the success rates and incidence of side-effects are for each option. The treating doc to r and attending healthcare team need to know that the patient understands the implications of their decision. To add to the complexity of issues in applying informed consent principles in this area, some consent can be verbal or implied, and consent need not be in writing to be enforceable. It should be pointed out that the signature on a consent form is not considered to be enough to show the consent is valid and informed. This is connected to the fundamental right of an adult with decisional capacity to refuse medical treatment even if this results in their death or would cause it to happen sooner. End-of-life care: Guidelines for decision-making about withholding and withdrawing January 2018 32 life-sustaining measures from adult patients However, it is important to note that informed consent provisions apply when decisions are made by a substitute decision-maker at the time that health or medical treatment is required, in the same way as they apply when a competent adult decides whether or not to undergo treatment. The treating health care team is obliged to give the substitute decision-maker sufficient information to make that decision in an informed manner. This is to ensure the decision is based on accurate information and not on any misunderstanding or misinterpretation of the facts. In these instances, there is a careful balance between pressuring the patient in to something they do not wish and ensuring the information provided to the patient is consistent with good medical practice. If those closest to the patient are involved in these discussions, care must also be taken to ensure the wishes and views of the patient, rather than their family, are followed. Offering and informed consent In non-urgent situations, the legislation requires that consent is obtained in order to withhold life 71 sustaining measures. However, the reading of this provision is the cause of some uncertainty and also linked to requirements for informed consent. The most extreme interpretation of these provisions would have doc to rs offering every conceivable medical treatment in order to obtain consent to withhold it (that is, not to provide it). This has caused implications for the practical application of the legislation that are unlikely to have been intended by Parliament when the withholding and withdrawing life-sustaining measures provisions were introduced in 2001. Discussing treatment options that in all reasonableness cannot be provided or would be considered potentially futile is counter-productive to an effective doc to r/patient relationship. Falsely raising hopes for a dying person and their family by suggesting forms of treatment that would not benefit the patient and have the potential of causing harm is cruel, callous and would not constitute good medical practice. In fact there is no legal or ethical obligation to offer medical treatment that is not clinically indicated (this is discussed further in section 1. However, it is recognised that prospective decision-making in the end-of-life arena is fraught with uncertainty. Therefore, decisions about what treatments to offer dying patients must be made based on the specific needs of each patient, not on what treatment was offered to another patient of similar age or condition. If the doc to r is aware that the patient objects to certain medical treatment being provided, and decisions are required urgently, the doc to r would be required to establish two other fac to rs: (i) the patient had minimal understanding of what the health care involves and why the 73 health care is required, and (ii) providing the health care would cause the patient no distress or only temporary 74 distress that would be outweighed by the benefits of providing the health care. It is recognised that in acute emergency situations, there is not always time to locate and verify some of the documents mentioned above. In these cases, when critical time is needed to save the life and health of the patient, best efforts must be made to obtain the appropriate legal consent, (or rely on authority in legislation where consent is not required), given the circumstances. Ignoring consent provisions in the legislation has the potential to expose the doc to r and other members of the health care team to risk of criminal and civil liability if the clinical decision is to not resuscitate the patient.
Buy wellbutrin sr 150mg cheap
J Spinal Disord sence of back pain mood disorder emotion generic wellbutrin sr 150mg free shipping, an absence of a work-related injury, pres Tech. Lumbar disc surgery: results of the including the foot, refex asymmetry and absence of back pain Prospective Lumbar Discec to my Study of the Joint Section on with straight leg raising have a better prognosis for good out Disorders of the Spine and Peripheral Nerves of the American comes following lumbar discec to my. The use of the operating Association of Neurological Surgeons and the Congress of microscope may decrease the need for facetec to my and improve Neurological Surgeons. Future Directions for Research Signs or Symp to ms Predictive of Favorable Surgical The work group identifed the following suggestions for future Outcomes References Bibliography studies, which would generate meaningful evidence to assist in 1. Lumbar disc surgery: results of the further defning the signs or symp to ms associated with lumbar Prospective Lumbar Discec to my Study of the Joint Section on Disorders of the Spine and Peripheral Nerves of the American radiculopathy that predict a favorable outcome in surgically Association of Neurological Surgeons and the Congress of treated patients with lumbar disc herniation with radiculopathy. Cauda equina syndrome secondary to lumbar disc gical intervention for cauda equina syndrome, a randomized herniation: a meta-analysis of surgical outcomes. The relationship between symp to ms and abnormal tive collection of information related to pre-operative functional magnetic resonance images of lumbar intervertebral disks. Correlation of preoperative depression and somatic percep Recommendation #2: tion scales with pos to perative disability and quality of life afer Collecting data regarding the preoperative characteristics and lumbar discec to my. The triad of nerve root enhancement, thickening, and displacement in patients with sci vention for lumbar disc herniation using validated outcomes atica and recurrent disk herniation in the pos to perative lumbar measures would potentially provide Level I. This information spine may prompt further surgical treatment in patients with could be collected using a prospective national registry. Posterior epidural Signs or Symp to ms Predictive of Favorable Surgical migration of lumbar disk fragments: report of two cases and Outcomes References review of the literature. Outcome evaluation of tion scales with pos to perative disability and quality of life afer the operative management of lumbar disc herniation causing lumbar discec to my. Trends multifac to rial outcome in lumbar discec to my A prospective in adolescent lumbar disk herniation. Lumbar disk protru sion rates of symp to matic patients using magnetic resonance imaging. The post-operative lumbar spine A radiological inves this clinical guideline should not be construed as including all proper methods of care or excluding or other acceptable methods of care reason ably directed to obtaining the same results. Physical examination for lumbar radiculopathy due to disc conjoined lumbosacral nerve roots versus lumbar intervertebral herniation in patients with low-back pain. Segmental over syndrome: fac to rs afecting long-term functional and sphinc lap: foot drop in S1 radiculopathy. The natural his to ry of disc herniation and the associated with recurrent disc herniation and disc height loss. Surgical vs nonop Clinical features of extraforaminal lumbar disc herniation based erative treatment for lumbar disk herniation: the Spine Patient on the radiographic location of the dorsal root ganglion. J Spinal Disord erative treatment for lumbar disk herniation: the Spine Patient Tech. Contrast tween diagnostic nerve root block and the results of surgery in fow selectivity during transforaminal lumbosacral epidural steroid injections. The efect of steroid injection compared with discec to my A prospective, sedation on diagnostic validity of facet joint nerve blocks: an randomized study. Apr 2004;86A(4):670 evaluation to assess similarities in population with involvement 679. A prospective, randomized, double-blind nerve root blocks in the treatment of lumbar radicular leg pain. A best-evidence review of diag of the evidence for selective nerve root injection in the treat nostic procedures for neck and low-back pain. Jan-Feb systematic review of diagnostic utility of selective nerve root 1980;5(1):68-77. The use of electromyography to steroid injections in lumbosacral radiculopathy: a prospective predict functional outcome following transforaminal epi randomized study. Surgical intervention prior to six months is suggested in patients with symp to matic lumbar disc herniation whose symp to ms are severe enough to warrant surgery. Earlier surgery (within six months to one year) is as sociated with faster recovery and improved long-term outcomes. Grade of Recommendation: B this clinical guideline should not be construed as including all proper methods of care or excluding or other acceptable methods of care reason ably directed to obtaining the same results. In patients available for follow-up at six months and 71 were available at for whom duration of leg pain was the shortest (less than four one year. Adjusted for age, when sessed at 52 weeks using the Roland Morris Disability Question time between symp to m onset and surgery was greater than 6. Relief of leg signifcantly worse at one year compared with when this period pain was faster for patients assigned to early surgery (p<0. In both groups, however, the probability of perceived six months and one year afer surgery. Prolonged duration of cluded that the one-year outcomes were similar for patients as preoperative symp to ms appears to impact negatively on patient signed to early surgery and those assigned to conservative treat outcome. Because of the high crossover rate, with 11% in the early to patients with symp to m duration less than six months when surgery group and 39% in the conservative group, this potential patients are managed with usual care prior to surgery. If the result was expressed as a coefcient, an increase lumbar disc herniation with radiculopathy. The authors the rate and extent of the recovery of ankle dorsifexion weak concluded that patients with sciatica for more than 12 months ness in patients treated with surgical decompression at various have a less favorable outcome. No variation was detected in the intervals [urgent (<10 days), expeditious (<30 days) and rou results for patients operated on in whom the duration of sciatica tine (>30 days)]. An peutic evidence that the duration of symp to ms of sciatic pain kle dorsifexion power at the long-term follow-up signifcantly (less than four months versus greater than 12 months) prior to correlated with the preoperative ankle dorsifexion power (p < surgery signifcantly and negatively afects outcomes afer lum 0. The authors concluded that the Nygaard et al described a prospective case series includ duration of ankle dorsifexion weakness did not correlate with this clinical guideline should not be construed as including all proper methods of care or excluding or other acceptable methods of care reason ably directed to obtaining the same results. Apr 15 peutic evidence that timing of surgery does not afect recovery of 2005;30(8):927-935. Cauda equina syndrome caused by intervertebral lumbar disk prolapse: mid-term results of 22 patients and literature review. Outcome evaluation of analyses of patients with mo to r defcits to provide information the operative management of lumbar disc herniation causing on the importance of timing of surgery on recovery from mo to r sciatica. Late results of surgery for herniated lumbar disk as related to duration of preoperative Surgical Timing References symp to ms and type of herniation. Duration of leg pain as a Recovery of ankle dorsifexion weakness following lumbar de predic to r of outcome afer surgery for lumbar disc herniation: a compressive surgery. Considerations on a pathology with diferent clinical herniation: a meta-analysis of surgical outcomes. Cauda equina syndrome caused syndrome: fac to rs afecting long-term functional and sphinc by intervertebral lumbar disk prolapse: mid-term results of 22 teric outcome. Cauda equina syndrome secondary to lumbar disc routine neurosurgical spinal surgery. Ceska outcomes of surgical and nonsurgical management of sciatica a Slovenska Neurologie a Neurochirurgie. Discec to my is suggested to provide more effective symp to m relief than medical/interventional care for patients with lumbar disc herniation with radiculopathy whose symp to ms warrant surgical intervention. In patients with less severe symp to ms, surgery or medical/interventional care appear to be effective for both short and long-term relief. Of the 100 patients included in the study, 50 were assigned Weinstein et al3,4 conducted a prospective randomized con to each treatment group. In the randomized group there were three months the surgically treated patients had a signifcant in 245 surgically treated patients and 256 medical/interventional crease in mo to r function compared to the patients treated with patients. At two years the mo to r function was surgically and 222 patients were treated medically/intervention not signifcantly diferent. Tere was 30% crossover from the medical/ surgically treated group expressed 92%-98% satisfaction versus interventional group to the surgical group. Tere were 27 one year, two years and four years the treatment efect in the patients that failed epidural steroid injections and crossed over intent- to -treat analysis favored surgery. Because of the large num dural steroid injection was not as efective as discec to my with bers of crossover patients, conclusions about the superiority or regard to reducing symp to ms associated with a large herniation equivalence of treatments are not warranted based on the intent of the lumbar disc. However, about 50% of patients who have injec compared to medical/interventional patients. Osterman et al5 described a prospective randomized con Weinstein et al2 reported results of both a prospective com trolled trial assessing outcomes of microdiscec to my compared parative study including 743 patients comparing surgical and to conservative treatment for lumbar disc herniation in patients medical/interventional treatment of lumbar intervertebral disc with six to 12 weeks of symp to ms.
Buy discount wellbutrin sr on line
Know when to use a low phosphate diet and phosphate-binding agents to treat hyperphosphatemia 5 depression definition webster discount wellbutrin sr 150mg mastercard. Know how magnesium salts should be administered and the specific drawbacks of each route of administration 6. Know that the organic matrix of bone contains collagen (particularly type I) and osteocalcin and that unmineralized bone matrix is called osteoid b. Know that bone mineral is deposited in the matrix and consists principally of hydroxyapatite, which contains calcium and phosphate c. Know that bone mineralization requires sufficient extracellular calcium and extracellular phosphate and is promoted by osteoblasts 2. Know that alkaline phosphatase is an enzyme essential for normal mineralization of bone 3. Know that alkaline phosphatase in liver and bone are biochemically distinguishable and that bone alkaline phosphatase is a marker of bone formation d. Be aware that bone is continually remodeled through the combined actions of osteoblasts and osteoclasts and that an imbalance between formation and resorption can lead to osteoporosis or osteopetrosis. Understand that longitudinal bone growth occurs at the growth plate by endochondral bone formation in which cartilage is created and then remodeled in to bone tissue 2. Be familiar with the mechanisms of replacement of cartilage with ossification centers 3. Recognize the causes of acquired osteoporosis in childhood, particularly disuse and glucocorticoid therapy 3. Know the foods rich in calcium so as to properly advise the optimal dietary calcium intake b. Recognize that osteogenesis imperfecta can be due to mutations of the type I collagen gene 2. Recognize the clinical features of osteogenesis imperfecta and the clinical spectrum of the disease 3. Know that "malignant" osteopetrosis is a recessively inherited disorder of osteoclasts 2. Know the various forms of therapy for osteopetrosis (including calcitriol, bone marrow transplantation) 3. Know the various causes of rickets and be able to determine the cause in a patient based on clinical and biochemical features 4. Know that rickets and osteopenia may occur in premature infants as a result of dietary phosphate and/or calcium deficiency 5. Know the principal clinical and biochemical manifestations of hypophosphatasia, an inherited deficiency of alkaline phosphatase leading to rickets-like bone disease and craniosynos to sis 2. Know that distal type renal tubular acidosis may lead to rickets in childhood and eventually to dense nephrocalcinosis 4. Recognize that aluminum to xicity may occur with parenteral nutrition of neonates 2. Be able to distinguish between benign and clinically significant forms of hyperphosphatasemia 2. Know that bone formation and resorption can be assessed by serum and urinary markers 7. Know the difference between soft-tissue calcification and ec to pic bone formation 3. Know the embryology of the formation and migration of the thyroid gland and the developmental genes involved b. Know the pattern and timing of hypothalamic-pituitary thyroidal function in the fetus 2. Understand the synthesis of thyroid hormones, including iodide metabolism, uptake, organification, incorporation in to thyroglobulin, coupling, and proteolytic secretion 3. Be aware of the changes in thyroid hormone concentrations in the immediate neonatal period and the first weeks after birth b. Be aware of the various proteins in blood which bind thyroid hormones and their relative clinical importance 5. Understand the metabolism of thyroid hormone, its regulation, and its physiologic significance 6. Know that thyroid hormone recep to rs belong to the nuclear (steroid) hormone recep to r superfamily, and that multiple isoforms exist c. Understand the role of the surge of thyroid hormone in thermal homeostasis, especially in the newborn period B. Be aware that transplacental passage of certain substances including radioiodine, iodides, propylthiouracil and methimazole administered to the mother may affect fetal thyroid development and/or function 2. Know the concentrations of thyroid hormones and their metabolites throughout fetal development b. Know the value of ultrasonography in detecting thyroidal enlargement in the fetus c. Know the efficiency of fetal brain deiodination in the face of fetal hypothyroidism d. Know that maternal hypothyroidism is associated with increased fetal loss and with mild cognitive delay in the infant. Know that when there is hypothyroidism in the mother and the fetus, severe mental retardation is likely in the fetus b. Be aware of potential effects on the breast-fed infant of antithyroidal agents ingested by the mother b. Recognize that worldwide iodide deficiency is the most common cause of congenital primary hypothyroidism and of preventable mental retardation c. Based on knowledge of embryology, understand the various ana to mical abnormalities causing congenital hypothyroidism (agenesis, maldescent, lingual thyroid) f. Know the approximate incidence of the various causes of congenital hypothyroidism g. Recognize that congenital central hypothyroidism is often associated with other pituitary hormone deficiencies 2. Be aware that congenital hypothyroidism is the most common disease screened for in newborns 4. Be familiar with the clinical significance of the effect of prematurity on thyroid function in the neonate 5. Know the clinical findings of congenital hypothyroidism and when they become manifest 7. Know the clinical findings of Pendred syndrome and recognize that mutations in the affected gene are an important cause of sensorineural deafness b. Be aware of techniques for defining the ana to my of the thyroid (scans and ultrasound) 4. Be aware that the recommended dosage of thyroxine per kg of body weight for congenital hypothyroidism changes with the age of the child 4. Be aware of the advantages of maintaining high-normal concentrations of thyroxine in serum for optimal outcome in treating congenital hypothyroidism 7. Know potential side effects of overtreatment of congenital hypo thyroidism (premature craniosynos to sis and advanced bone age) 8. Know that mild hypothyroidism frequently normalizes and that treatment may not be necessary d. Be familiar with the prognosis for future cognitive development in congenital hypothyroidism and the fac to rs that affect this prognosis. Be able to cite advantages and disadvantages of various systems of neonatal thyroid screening 4. Know the appropriate diagnostic approaches for children with various abnormalities on newborn screening 5. Be aware of various transient abnormalities in thyroid function which may be detected by neonatal screening 6. Recognize that congenital hypothyroidism may not be detected in a small number of infants by neonatal screening c. Be aware that thyroid hormone deficiency may develop during treatment of growth hormone deficiency c. Know which drugs may interfere with thyroid function (eg, iodides, lithium, and amiodarone) and the clinical correlates of these drugs in thyroid physiology d.
Purchase 150 mg wellbutrin sr with amex
First-trimester and quad screening have care center for delivery of the newborn if needed anxiety 7 year old buy wellbutrin sr 150mg low price, and similar detection rates for Down syndrome: more than perinatal hospice care as appropriate for a child with a 80% at a 5% positive result rate (Table 2) (5). Patients found gestational dating at the time of blood sampling is impor to have a fetus with a chromosomal abnormality often tant because inaccurate gestational dating decreases the benefit from referral to a genetics professional for further accuracy of the result. Can be performed at any clearly reported equivalent result) gestational age after 10 weeks 2. Low false-positive rate in high-risk women (or women at high risk of risk of Down syndrome Down syndrome) 3. Down syndrome screening in the first and/or second trimester: model predicted performance using meta-analysis parameters. Using stepwise sequen limited retrospective trial that this test may improve tial screening, the patient is given a preliminary risk second-trimester screening performance, its performance estimate after completion of the first-trimester analytes has not been evaluated rigorously in prospective stud and nuchal translucency screening. Limited data are available screening result indicates that the risk of aneuploidy is to compare the accuracy of the penta screen with other greater than the labora to ry-derived positive screening second-trimester screening tests. This screening test result and proceeds to quad screening in test provides a lower sensitivity for the detection of Down the second trimester. First Integrated Screening and Serum Integrated and second-trimester results are used to gether to Screening calculate a final risk of aneuploidy in patients at lower With integrated screening, the patient undergoes a first risk in the stepwise and sequential models. The sequential trimester nuchal translucency measurement and analyte approach takes advantage of the higher detection rate screening followed by a second-trimester quad screen achieved by incorporating the first and second-trimester and receives a single test result in the second trimester. Theoretically, the contingent approach by a certified ultrasonographer is unavailable, or if fetal should maintain high detection rates with low false position, maternal body habitus, or imaging properties positive rates while reducing the number of second preclude an accurate nuchal translucency measurement, trimester tests performed. Serum inte the use of multiple screening tests performed inde grated screening has a similar but slightly lower detec pendently (eg, a first-trimester screening test followed by tion rate than integrated screening (Table 2). Limitations a quad screen as an unlinked test) is not recommended of integrated screening include the withholding of first because it will result in an unacceptably high positive trimester screening test results until the second trimester screening rate and could deliver confusing risk esti and nonadherence of the second blood draw; rates of mates to patients. In patients who undergo first-trimester nonadherence in practice have been reported to be as screening, if later screening for risk of neural tube defects high as 25% without a written reminder to complete the is to be done with maternal serum alpha-fe to protein test (8). This amount increases on ultrasonography, the ultrasonographic identification throughout gestation and is cleared from the maternal of Down syndrome is more elusive. This approach seeks appear to have similar detection and false-positive rates, to identify major structural abnormalities and minor although direct comparison trials have not been performed. Screening can be performed from as early as 10 weeks duodenal atresia, which typically is identified in the third of gestation until term and offers the highest reported trimester. In contrast, second and third-trimester soft detection rate for Down syndrome: more than 98% detec ultrasonographic markers for aneuploidy are nonspecific tion with positive screening rates of less than 0. Further, can reflect or progress to an overt fetal abnormality (eg, published studies have excluded those who have no report thickened nuchal fold, renal pelvis dilation, or echogenic able result, and these women are at increased risk of fetal bowel). Inclusion of these women in the common in unaffected fetuses, it is difficult to use these calculations would yield lower sensitivity for fetal aneu findings to distinguish between pregnancies affected or ploidy. As an isolated finding, an result as screen positive will decrease the specificity and increase the positive screening rate for this testing. In contrast, an isolated echogenic intracardiac focus carries one of the lowest risks of fetal aneuploidy (12, 13). Additional follow-up for isolated All women should be offered the option of aneuploidy ultrasonographic markers generally is not indicated other screening or diagnostic testing for fetal genetic disorders, than for isolated renal pelvis dilation, echogenic bowel, regardless of maternal age. Patients with affected by many fac to rs, including a desire for informa these markers may benefit from referral for detailed tion before delivery, prior obstetric his to ry, family his to ry, ultrasonography and follow-up. Other fac to rs to be considered use of second-trimester ultrasonographic markers include include gestational age at presentation, the availability of the lack of standardization in measurements and charac a reliable nuchal translucency measurement, screening teristics that define a positive test result, and the lack of test sensitivity and limitations, the cost of screening, the understanding of how fac to rs such as high maternal body constraints of long-term care of an affected child, and mass index, multiple gestation, machine quality, and options for pregnancy care or termination for an abnor experience of the ultrasonographer and ultrasonologist mal diagnostic test result. Regardless of which screening tests are 6 Published Ahead of Print Practice Bulletin: Screening for Fetal Aneuploidy offered, information about the detection (sensitivity) and the finding of an increased nuchal translucency positive screening and false-positive rates, advantages, extending along the length of the fetus in which septa disadvantages, and limitations should be communicated tions are clearly visible is referred to as a cystic hygroma. At the time of counseling regarding aneu this finding is associated with a 50% likelihood of fetal ploidy screening, the benefits and risks of diagnostic aneuploidy (most commonly Down syndrome, 45,X, and testing (amniocentesis and chorionic villus sampling) also trisomy 18). After counseling, patients may have a major structural malformation, such as congenital decline screening or diagnostic testing for any reason. Less than 20% of such pregnan What is the role of ultrasonography in cies will result in a healthy live-born infant at term (33). As such, ultrasonography trimester ultrasonography for gestational dating even if should not be used in isolation to diagnose or exclude Down nuchal translucency measurement is unavailable or cannot syndrome. If an enlarged nuchal translucency, an obvious disorders, and the various soft markers have different anomaly, or a cystic hygroma is identified on ultrasono degrees of association with Down syndrome. The risk of graphy, the patient should be offered genetic counseling aneuploidy associated with each marker should be consid and diagnostic testing for aneuploidy as well as follow-up ered individually within the complete clinical context. Given presence of soft ultrasonographic markers for aneuploidy the high risk of congenital heart disease in these fetuses, warrants a targeted ultrasound to exclude other evident referral for fetal cardiac ultrasonography should be con abnormalities and a review or offering of screening tests sidered. Of the soft markers, third-trimester or cystic hygroma and normal fetal karyotype should be follow-up is only indicated for isolated renal pelvis dilation, offered an ana to mic evaluation in the second trimester, fetal echogenic bowel, or shortened humerus or femur (14). For cardiac ultrasonography, and further counseling regarding women who have already undergone screening for aneu the potential for genetic syndromes not detected by aneu ploidy and have received a negative screening test result, ploidy screening. However, further detailed counseling is recom the first-trimester screening, or first-trimester combined mended for fetuses with a hypoplastic or absent nasal bone, screening, comprising nuchal translucency measurement echogenic bowel, or nuchal skinfold thickening (14). If an and serum analyte measurements combined in to a single isolated ultrasonographic marker for aneuploidy is detected, test, is performed before 14 0/7 weeks of gestation (with the patient should be offered aneuploidy screening if it was the range determined by the labora to ry accepting the not offered previously. Advantages of genetic syndromes and isolated anomalies, such as con first-trimester screening are a slightly higher, but not genital heart defects, abdominal wall defects, and dia significantly different, detection rate for Down syndrome phragmatic hernia, even with normal chromosomes on compared with second-trimester screening. These patients should be offered the potential for earlier diagnoses as well as the ability a targeted ultrasound examination and fetal echocardiog to screen for other fetal or placental disorders. Second-trimester detailed ana to mic survey dysplasias, congenital heart disease, and and fetal cardiac ultrasonography other anomalies First trimester: Large single or multilocular If septate, approximately 50% are aneuploid 1. If aneuploidy screen result is negative, no chamber view further evaluation is required. If isolated finding, aneuploidy screening pyelectasis fi 4 mm in anteroposterior should be offered if not performed previously diameter up to 20 weeks of 2. Further counseling echogenic bowel echogenic as bone Associated with aneuploidy, intra-amniotic 2. Detailed ana to mic survey thickened nuchal fold the occipital bone to outer > 99% specificity for Down syndrome 2. Further detailed genetic counseling and skin in the midline Most powerful second-trimester marker aneuploidy screening or diagnostic testing Second trimester: mild Lateral ventricular atrial Associated with aneuploidy 1. Repeat ultrasound in third trimester Second trimester: Discrete cyst(s) in one or In isolation, no aneuploidy association 1. Second-trimester detailed ana to mic survey choroid plexus cysts both choroid plexus(es) and fetal cardiac ultrasound 2. Consider aneuploidy screening or diagnostic testing if other markers are present Second trimester: short Measurement < 2. Fetal imaging: executive summary of a joint Eunice Kennedy Shriver National Institute of Child Health and Human Development, Society for Maternal-Fetal Medicine, American Institute of Ultrasound in Medicine, American College of Obstetricians and Gynecologists, American College of Radiology, Society for Pediatric Radiology, and Society of Radiologists in Ultrasound Fetal Imaging workshop. First-trimester septated cystic hygroma: prevalence, natural his to ry, and pediatric outcome. Fetal nuchal translucency: ultrasound screening for chromosomal defects in first trimester of pregnancy. Based on cy to genetic confirmation, the positive syndrome and placental sulfatase deficiency if indicated predictive value, or chance that a positive screening test by an extremely low unconjugated estriol value.