
Differin
Order differin 15gr overnight delivery
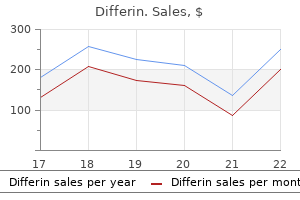
We report three population-based measures: patient experience measures acne bp5 purchase cheap differin line, avoidable hospitalizations for ambulatory care?sensitive conditions, and rates of low-value care in Medicare. Median compensation in 2017 was much lower for primary care physicians than for physicians in certain specialties, such as radiology and nonsurgical, procedural specialties, continuing to raise concerns about fee schedule mispricing and its impact on primary care. The evidence suggests that Medicare payments for physicians and other health professionals are adequate. Therefore, the Commission recommends that the 2020 payment rate for physician and other health professional services be updated by the amount specified in current law. In 2017, about 985,000 spending by restraining annual updates when spending health professionals billed Medicare through the fee exceeded certain parameters. In 2020, Medicare uses a fee schedule to pay for physician and there is no statutory update for clinicians. Report to the Congress: Medicare Payment Policy | March 2019 99 the broader health care delivery system. This year, we conducted nine focus groups of Medicare beneficiaries in three markets, and we conducted Very satisfed 68% 55% a primary care physician focus group in each location. In Somewhat satisfed 20 25 these markets, we also conducted site visits and interviews Somewhat dissatisfed 3 5 Very dissatisfed 2 1 with various providers. Overall, findings from our survey and focus groups are Note: Table excludes the following responses: Did not receive health care 2 in past 12 months, Don?t know, and Refused. Medicare beneficiaries overall satisfaction with care is similar to satisfaction among privately insured patients In our telephone survey, a slightly higher share of Are Medicare fee schedule payments Medicare beneficiaries reported that they were very or adequate in 2019? In particular, across specialties, and the change in input prices for in 2018, 70 percent of Medicare beneficiaries reported that physician and other health professional services. Overall, they never had to wait longer than they wanted for routine most indicators show no significant change from prior care, and 79 percent reported the same for illness or injury years. Medicare beneficiaries were less likely to report trouble obtaining either type of care when needed Beneficiaries access to care than privately insured individuals (the rates for privately We use a number of measures to assess beneficiary access insured individuals were 64 percent for routine care and 74 to timely, appropriate care, including direct reporting from percent for illness or injury care). The goal Medicare beneficiaries were also less likely than privately in surveying these two populations is to assess whether insured individuals to report that they waited longer than access concerns reported by Medicare beneficiaries are they wanted for care for illness or injury (Figure 4-2, p. Was it Primary care physician No problem 67 67 64 69a 71 63 63 63 59ab 67 Share of total insurance group 5. Medicare Private insurance Source:30 30 Always Always Usually Usually Notes about this graph: Sometimes Sometimes. Otherwise if you use the black selection tool, they will reset to graph default when you change the data. X-X finding a new primary care doctor, Medicare and private insurance Medicare Private insurance 50 50 A small problem A small problem A big problem A big problem 40 40 30 30 20 20 10 10 0 0 2006 2008 2010 2012 2014 2016 2018 2006 2008 2010 2012 2014 2016 2018 Note: the share of respondents looking for a new doctor each year is about 10 percent for primary care. Therefore, the share of Medicare respondents facing a problem (small or big) in obtaining a new primary care doctor was 2. Source: Beneficiaries report more difficulty accessing big problem, meaning that, on net, 1. We also ask respondents whether, when they are lookingNotes about this graph: this pattern of greater difficulty for Medicare for a new doctor, they are able to find one without Data is in the datasheet. Consistent with prior years, beneficiaries looking for a beneficiary focus groups. Otherwise if you use the black selection tool, they will reset to graphto report problems obtaining primary and specialty care 10 percent were looking for a new doctor, and of those default when you change the data. For specialty care, 19 percent were looking reported difficulty with certain specialty referrals, namely for a new doctor; of those looking, 8 percent reported a dermatologists (likely due to specialization in cosmetic dermatology vs. X-X trouble finding a new specialist, Medicare and private insurance Medicare Private insurance 25 25 A small problem A small problem A big problem A big problem 20 20 15 15 10 10 5 5 0 0 2006 2008 2010 2012 2014 2016 2018 2006 2008 2010 2012 2014 2016 2018 Note: the share of respondents looking for a new doctor each year is about 20 percent for specialty care. Therefore, the share of Medicare respondents facing a problem (small or big) in obtaining a new specialist was 2. Similar to prior years findings, that they could not obtain care as quickly as they wanted. Otherwise if you use the black selection tool, they will reset to graphMinority Medicare beneficiaries also reported higher rates telephone survey that Medicare beneficiaries who belongdefault when you change the data. Was it Primary care physician b b No problem 71 71 69 67 72 59 Share of total insurance group, by race 7. Was it Primary care physician No problem 71 72 68 67 68 64 Share of total insurance group, by area 7. In addition, Black beneficiaries are significantly more likely than non Supply of physicians and other health Hispanic White beneficiaries to report that they should professionals billing Medicare has kept pace with enrollment growth have seen a doctor but did not (15 percent vs. Between 2016 and differences in access between urban and rural beneficiaries 2017, the number of primary care physicians increased (Table 4-5). There was no significant difference between 4 by 1 percent, from almost 185,000 to just over 186,000. Urban percent between 2016 and 2017 (data not shown), the ratio beneficiaries reported more timely access to routine of primary care physicians to the number of beneficiaries care than urban individuals with private insurance. Similarly, the number of physicians in other individuals with private insurance were minimal and not specialties grew by 1 percent between 2016 and 2017, statistically significant in most cases. Similar to prior amount as payment in full (almost all claims are paid on years, rural beneficiaries were more likely than urban 6 assignment). Clinicians can also opt out of the Medicare with Medicare program and treat patients entirely outside of the Medicare Other indicators of access include the supply of clinicians benefit. Opt-out clinicians are concentrated in the provider billing Medicare; the share of physicians and other health specialties of dentistry and behavioral health (including professionals who are participating providers (which psychiatry). Most of the physicians who billed Medicare as hospitalists in 2017 billed as a primary care specialty in 2016. To maintain consistency across years, we assigned physicians who billed as hospitalists in 2017 to the primary care specialties group. The number billing Medicare includes those with a caseload of more than 15 different benefciaries during the year. Benefciary counts used to calculate numbers per 1,000 include those in fee-for-service Medicare and Medicare Advantage on the assumption that physicians and other health professionals are furnishing services to benefciaries in both programs. Figures for 2015 and 2016 may vary from fgures that appeared in prior Commission reports due to minor technical changes. Higher growth in the volume of clinician change in service use: units of service per beneficiary and services volume of services per beneficiary. However, we recommend measure thus accounts for changes in both the number of caution in interpreting such data because factors unrelated services and the complexity, or intensity, of those services. For example, growth in the volume of imaging services Evidence indicates that volume decreases could be related would account not just for any change in the number of to the movement of services from freestanding offices such services but also for any change in intensity. Each broad service category favor certain services because they are relatively contains multiple subcategories of similar services. Among We used claims data from 2012, 2016, and 2017 to analyze broad service categories, growth rates were 1. Use of behavioral health services is not reported for 2012 to 2016 because of a change in billing codes implemented in 2013. Some low-volume categories are not shown but are included in the summary calculations. However, this subcategory had a very low levelE&M of volume in 2012 (data not shown). E&M from 2009 to 2010 is not directly observable because of a change in payment policy for consultations. To compute cumulative volume growth Although care management/coordination experienced high for E&M through 2017, we used a growth rate for 2009 to 2010 of 1. Cumulative growth in the volume of imaging per beneficiary from 2000 to 2017 totaled 75 percent, which was much higher than cumulative growth during the services and for broad service categories were higher thanNotes about this graph: same period for major procedures and E&M services (47 the average annual growth rates from 2012 to 2016, except. By contrast, from 2012 Subcategories of a broad service category sometimes experienced more rapid volume growth in 2017 than the Use direct selection tool to select items for modi? As part of this ongoing effort, more than 80 vascular procedures subcategory had no change in units specialty societies have identified over 550 tests and of service in 2017 but a 9. The goal of Choosing Wisely is to promote 110 Physician and other health professional services: Assessing payment adequacy and updating payments and inform conversations between clinicians and their a freestanding office. Under this program, clinicians who order hospital?based E&M visits per beneficiary grew by 19.
Purchase genuine differin line
Splints must hold the finger in continuous acne essential oil recipe cheap 15 gr differin overnight delivery, full extension for a minimum duration of 6 weeks. Of the 12 articles considered for inclusion, 1 randomized trials and 3 systematic studies met the inclusion criteria. Recommendation: Instructions for Splint Wear It is recommended that careful instructions on splint wear be provided to patients. Strength of Evidence Recommended, Insufficient Evidence (I) Level of Confidence High Rationale for Recommendation There are no quality studies evaluating the use of instructions for splint wear for mallet finger. However, instructions appear critical for preventing treatment failures and are thus recommended. Of the 6 articles considered for inclusion, 0 randomized trials and 2 systematic studies met the inclusion criteria. Follow-up Visits Patients require a few appointments to reinforce importance of splinting and of not removing the splint unsupported. Medications Nonprescription medications are usually not required as mallet finger is generally not painful. Prescription medications are rarely required as mallet finger is generally not painful. Evidence for the Use of Medications There are no quality studies incorporated into this analysis. However, patients usually require careful education about splinting (see Education above). Evidence for the Use of Exercise There are no quality studies incorporated into this analysis. Of the 2 articles considered for inclusion, 01 randomized trials and 0 systematic studies met the inclusion criteria. Strength of Evidence Recommended, Insufficient Evidence (I) 195 Copyright 2016 Reed Group, Ltd. Recommendation: Surgical Interventions for Failed Splinting Cases of Mallet Finger Surgery is recommended for those cases that fail splinting yet have sufficient symptoms or concerns that an attempt at fixation is desired. Strength of Evidence Recommended, Insufficient Evidence (I) Level of Confidence Moderate Rationale for Recommendation Quality studies to determine which patients with mallet finger would be optimal for surgical interventions are not currently available. A low-quality study also suggested no difference in splinting outcomes among those presenting late. Of the 9 articles considered for inclusion, 8 randomized trials and 1 systematic studies met the inclusion criteria. Author/Year Score Sample Size Comparison Group Results Conclusion Comments Study Type (0-11) O?Brien 6. The dorsal splints immobilization and graded finger splints should be blind 1b mallet finger; Vs. Clinical suggests increased lag Sponsored by (N=27) measurement overestimates true occurs after the splint is the Canadian Vs. Abouna The two splints were equally Type of splint appears 1988 males, 41 (N=58) splint: 19/58 (33%) vs 19/49 effective, producing a cure or a immaterial. Open reduction and hook Extension block pinning found fixation was higher than that of versus open reduction for No plate fixation group to be more cost-effective than extension block pinning. Flexor Tendon Entrapment (Tenosynovitis and Trigger Digit) Diagnostic Criteria the diagnosis of flexor tendon entrapment is clinical. Patients without triggering will typically have only focal A1 pulley tenderness with or without a tendon nodule. The threshold for testing for confounding conditions such as diabetes mellitus, hypothyroidism and connective tissue disorders should be low particularly to prevent other morbidity. Splints have been used to treat trigger digits(27, 36) and they may be reasonable intervention for patients who decline injection, although it is recommended that patients be educated that the use of splints appears substantially less successful than injections (or surgery). Of the 3 articles considered for inclusion, 1 randomized trials and 1 systematic studies met the inclusion criteria. Follow-up Visits Follow-up visits are generally limited unless complications arise. Success of injections is usually high, thus 1 or 2 follow-up appointments are typical. Post-surgical outcomes for minimally invasive approaches are similarly excellent and necessitate few, if any follow-up appointments beyond 1 or 2. Evidence for the Use of Medications There are no quality studies incorporated into this analysis. Of the articles considered for inclusion, 1 randomized trial and 1 systematic studies met the inclusion criteria. Evidence for the Use of Exercise There are no quality studies incorporated into this analysis. Indications Triggering digit or symptoms of pain over the A-1 pulley thought to be consistent with stenosing tenosynovitis. Injection at the first appointment may be the most appropriate initial intervention. Quality studies have included betamethasone 6mg,(38, 1054) depot preparation of methylprednisolone 20mg;(1055) and triamcinolone 1mL(1056) most of which were generally combined with an anesthetic. However, there are no quality comparisons of doses and the need for topical anesthetic is untested in quality studies. Subcutaneous injection over the A-1 pulley appears as efficacious as attempted intrasheath injection. Strength of Evidence Strongly Recommended, Evidence (A) Level of Confidence High Rationale for Recommendation There are 2 high-quality and 2 moderate-quality studies incorporated into this analysis. Multiple studies have consistently demonstrated efficacy of these injections compared with placebo with estimates of success typically exceeding 80%. Some caution is warranted regarding repeated administrations with adverse effects including atrophy that generally recovers over time. Nevertheless, quality studies have documented their efficacy and thus, they are strongly recommended. Of the 18 articles considered for inclusion, 13 randomized trials and 3 systematic studies met the inclusion criteria. There were no complications and success rate may be even better if repeat injections are used. No significant injections with gradual gradually benefits Quervains (standard injection, acidic difference between groups for pre improvement over the patients over first week No mention of tenosynovitis). Topical surgical and between percutaneous females) with injection: 2ml of pain (N) open vs. Follow-up at 6 triggering rate at 6 weeks: suggest that groups although Sponsored by trigger finger. Systems, Smith triamcinolone= trigger finger than does and Nephew, 65 years dexa-methasone. We were unable to least grade 2 detect a statistically by Quinnell significant difference in and without the response of patients previous with and without diabetes treatment of to either treatment trigger digit. Rise of recurrent technique without any recurrence rates and No mention of hydrochloride without symptoms occurred in both groups at 3 significant difference in general outcome sponsorship. Excluded suspension 6mg with injection 47% good, 16% fair, 37% the treatment of trigger those >6 months 0. Surgery Recommendation: Surgery for Persistent or Chronic Flexor Tendon Entrapment Open release for persistent or chronic flexor tendon entrapment is moderately recommended. Those without any response should be evaluated carefully for possible alternate conditions. Adjunctive surgical treatment with glucocorticosteroid injection could be considered, although that evidence relies on a single moderate quality study. A moderate-quality study attempted to identify which third of the pulley was responsible for triggering; however, failures occurred in all surgical groups regardless of which third of the pulley was released. One moderate-quality study compared injections with percutaneous release combined with glucocorticosteroid injection and reported surgical release was superior,(1098) although the success rates were both lower than other reports. Surgical release is invasive (though less invasive with percutaneous release),(1108) has low adverse effects, but is costly. For those patients failing glucocorticosteroid injection(s), surgery is recommended.
Generic differin 15gr with visa
The certification issues include the amount of disease the driver has experienced and the severity of the symptoms skin care order on line differin. The potential risk is that if the disease is progressive, respiratory insufficiency may develop. Waiting Period No recommended time frame You should not certify the driver until etiology is confirmed and treatment has been shown to be adequate/effective, safe, and stable. Decision Maximum certification 2 years Recommend to certify if: the disease remains relatively stable and the driver has normal lung function and tolerates the medical regimen. Monitoring/Testing You should perform pulmonary function tests if you suspect the disease has become progressive and may cause extensive pulmonary symptoms. Follow-Up the driver should have follow-up dependent upon the clinical course of the condition and recommendation of the treating healthcare provider. Monitoring/Testing You may on a case-by-case basis obtain additional tests and/or consultation to adequately assess driver medical fitness for duty. If the conversion occurred within the last year, active disease may develop and prophylactic therapy should take place. This circumstance would not require limiting the activities of the driver unless medication side effects and/or adverse reactions occur. Follow-Up the driver should have follow-up dependent upon the clinical course of the condition and recommendation of the treating healthcare provider. Non-infectious Respiratory Diseases this category includes a number of diseases that cause significant long-term structural changes in the lungs and/or thorax and, therefore, interfere with the functioning of the lungs. Obvious difficulty breathing in a resting position is an indicator for additional pulmonary testing. Chest Wall Deformities Acute or chronic chest wall deformities may affect the mechanics of breathing with an abnormal vital capacity as the predominant abnormality. Examples of these disorders include kyphosis, kyphoscoliosis, pectus excavatum, ankylosing spondylitis, massive obesity, and recent thoracic/upper abdominal surgery or injury. The driver certified with a chest wall deformity should have airway function near normal. However, individuals may be particularly sensitive to the side effects of alcohol, antidepressants, and sleeping medications, even in small doses. Waiting Period No recommended time frame You should not certify the driver until etiology is confirmed and any associated treatment has been shown to be adequate/effective, safe, and stable. Page 128 of 260 Decision Maximum certification 2 years Recommend to certify if: As the medical examiner, you believe that the nature and severity of the medical condition does not endanger the health and safety of the driver and the public. Monitoring/Testing Obvious difficulty breathing in a resting position is an indicator for additional pulmonary function tests. Follow-Up the driver should have follow-up dependent upon the clinical course of the condition and recommendation of the treating healthcare provider. The driver may have substantial reduction in lung function prior to developing dyspnea on exertion. Waiting Period No recommended time frame You should not certify the driver until etiology is confirmed and treatment has been shown to be adequate/effective, safe, and stable. Page 129 of 260 Decision Maximum certification 2 years Recommend to certify if: As the medical examiner, you believe that the nature and severity of the medical condition of the driver is stable and does not endanger the health and safety of the driver and the public. Monitoring/Testing Obvious difficulty breathing in a resting position is an indicator for additional pulmonary function tests. Follow-Up the driver should have follow-up dependent upon the clinical course of the condition and recommendation of the treating healthcare provider. Some individuals have a mild form of the disease that may not be diagnosed until early adulthood. Individuals must be evaluated as to the extent of their disease and symptoms and ability to obtain therapy while working. Waiting Period No recommended time frame You should not certify the driver until it has been documented that treatment has been shown to be adequate/effective, safe, and stable and the driver complies with continuing medical surveillance by the appropriate specialist. Recommend to certify if: As the medical examiner, you believe that the nature and severity of the medical condition of the driver does not endanger the health and safety of the driver and the public. Monitoring/Testing Obvious difficulty breathing in a resting position is an indicator for additional pulmonary function tests. Follow-up the driver should have follow-up dependent upon the clinical course of the condition and recommendation of the treating specialist, but at least annually. A history of breathlessness while driving, walking short distances, climbing stairs, handling cargo or equipment, and entering or exiting the cab or cargo space should initiate a careful evaluation of pulmonary function for any disqualifying secondary conditions. Treatment side effects pose a significant potential problem because of the use of conicosteroids and cytotoxic agents and should be taken into account when assessing commercial drivers. Waiting Period No recommended time frame You should not certify the driver until etiology is confirmed and treatment has been shown to be adequate/effective, safe, and stable. Page 131 of 260 Decision Maximum certification 2 years Recommend to certify if: As the medical examiner, you believe that the nature and severity of the medical condition of the driver does not endanger the health and safety of the driver and the public. Monitoring/Testing Obvious difficulty breathing in a resting position is an indicator for additional pulmonary function tests. Follow-up the driver should have follow-up dependent upon the clinical course of the condition and recommendation of the treating healthcare provider. Pneumothorax Pneumothorax (air in the pleural space) may follow trauma to the chest or may occur spontaneously. Traumatic Pneumothorax A medical history and physical examination will provide the details of the event but may not help to ascertain recovery. Spontaneous Pneumothorax If spontaneous pneumothorax complicates an existing lung disease. Chest X-rays (especially views in deep inspiration and full expiration) will confirm the resolution of air from the pleural space but may show some residual pleural scarring or apical blebs or bullae. Waiting Period No recommended time frame Ensure complete recovery using chest X-rays. If there is air in the pleural space and/or air in the mediastinum (pneumomediastinum) additional time away from work is indicated. Decision Maximum certification 2 years Page 132 of 260 Recommend to certify if: the driver. Monitoring/Testing Chest X-rays with the frequency determined by both clinical assessment and by recurrence rates. Follow-up the driver should have follow-up dependent upon the clinical course of the condition and recommendation of the treating healthcare provider. Pulmonary Function Tests Physiological impairment is potentially present in many lung disorders. No further testing is necessary if the lung function is normal and no other abnormality is suspected. Secondary Respiratory Conditions and Underlying Disorders Cor Pulmonale Cor pulmonale refers to enlargement of the right ventricle secondary to disorders affecting lung structure or function. In North America, the most common pulmonary cause of cor pulmonale is hypoxic pulmonary vasoconstriction in individuals with chronic obstructive pulmonary disease. The most common cause of right ventricular dilation or enlargement is pulmonary hypertension secondary to left heart disease. Waiting Period No recommended time frame You should not certify the driver until diagnosis is confirmed and/or treatment has been shown to be adequate/effective, safe, and stable. Page 134 of 260 Recommend to certify if: As the medical examiner, you believe that the nature and severity of the medical condition does not endanger the health and safety of the driver and the public. Monitoring/Testing Obvious difficulty breathing in a resting position is an indicator for additional pulmonary function tests. Follow-up the driver should have follow-up dependent upon the clinical course of the condition and recommendation of the treating healthcare provider. Pulmonary Hypertension Pulmonary hypertension can occur with or without cor pulmonale. Significant pulmonary hypertension is pulmonary artery pressure greater than 50% systemic systolic blood pressure from any cause. Waiting Period No recommended time frame You should not certify the driver until diagnosis is confirmed and/or treatment has been shown to be adequate/effective, safe, and stable. Decision Maximum certification 1 year Recommend to certify if: As the medical examiner, you believe that the nature and severity of the medical condition does not endanger the health and safety of the driver and the public. Monitoring/Testing You may on a case-by-case basis obtain additional tests and/or consultation to adequately assess driver medical fitness for duty. Follow-up the driver should have follow-up dependent upon the clinical course of the condition and recommendation of the treating healthcare provider. Risk from Headaches Most individuals have experienced the symptoms of headaches, vertigo, and dizziness.
Buy differin 15gr low cost
Glucose metabolism in patients with acute myocardial infarction and no previous Israel: Israel Heart Society skin care now pueblo co best purchase for differin, Doron Aronson; Italy: Italian Federation. Oral glucose toler Cardiologists of Kazakhstan, Aigul Raissova; Kosovo (Republic of). Gyberg V, De Bacquer D, Kotseva K, De Backer G, Schnell O, Sundvall J, Society of Cardiology, Karlis Trusinskis; Lebanon:LebaneseSociety. Oral glucose tolerance test and HbA c for diagnosis of Jane Magri; Moldova (Republic of): Moldavian Society of. Risk identification and interventions to prevent type 2 diabetes in adults at high Society of Cardiology, Cristina Gavina; Romania: Romanian Society. Plasma high-sensitivity troponin T predicts end-stage renal disease and cardiovas 20. Perkovic V, Verdon C, Ninomiya T, Barzi F, Cass A, Patel A, Jardine M, Gallagher C, Prager R, Luger A, Pacher R, Clodi M. The relationship between proteinu vention of cardiac events in a population of diabetic patients without a history of. Arch Cardiovasc Dis vascular disease: a collaborative meta-analysis of 102 prospective studies. Silent coronary artery disease and incidence of cardiovascular and mortality Eliasson B, Gudbjornsdottir S. Effects of cardiac disease prevention in clinical practice: the Sixth Joint Task Force of the. Prevention in Clinical Practice (constituted by representatives of 10 societies and. Acampa W, Petretta M, Daniele S, Del Prete G, Assante R, Zampella E, Cuocolo by invited experts)Developed with the special contribution of the European. Risk stratification in uncomplicated type 2 diabetes: prospective evaluation of the Norhammar A. Detection of silent myocar Risk of cardiovascular disease and death in individuals with prediabetes defined. Risk reduction of cardiac events by screening of unknown asymp ence of age in a French multicenter study. Turrini F, Scarlini S, Mannucci C, Messora R, Giovanardi P, Magnavacchi P, with diabetes mellitus. Cappelli C, Evandri V, Zanasi A, Romano S, Cavani R, Ghidoni I, Tondi S, Bondi 54. Jellis C, Wright J, Kennedy D, Sacre J, Jenkins C, Haluska B, Martin J, Fenwick J. Akazawa S, Tojikubo M, Nakano Y, Nakamura S, Tamai H, Yonemoto K, analysis of data obtained in five longitudinal studies. Diabetes Care progression to predict cardiovascular events in the general population (the. Common carotid intima asymptomatic patients with diabetes: results of a randomized trial and meta-. Systematic review and persons at increased risk: a systematic review for the Community Preventive. Dietary fats and cardiovascular disease: a Presidential real-world impact on incidence, weight, and glucose. Macronutrients, food groups, and eating patterns in the manage Keinanen-Kiukaanniemi S, Laakso M, Louheranta A, Rastas M, Salminen V. Stevens W, Buck G, Barton J, Murphy K, Aung T, Haynes R, Cox J, Murawska 23-year follow-up study. Cardiovascular risk reduction with icosapent ethyl for hypertrigly intervention or metformin on diabetes development and microvascular compli-. Physical activity and mortality in individuals with diabetes mellitus: a prospective. Effects of acarbose on cardiovascular and diabetes out J Prev Cardiol 2012;19:1005A1033. Hirakawa Y, Arima H, Zoungas S, Ninomiya T, Cooper M, Hamet P, Mancia G, Effects of aerobic and resistance training on hemoglobin A1c levels in patients. N Engl J and risk of type 2 diabetes in European men and women: influence of beverage. Intensive structured self-monitoring of blood trol and macrovascular outcomes in type 2 diabetes. Hansen D, Niebauer J, Cornelissen V, Barna O, Neunhauserer D, Stettler C, glucose control with metformin on complications in overweight patients with. Exercise prescription in patients with different combina tes therapy on the progression of diabetic retinopathy in patients with type 1. Cardiovascular effects of bariatric sur Genuth S, Lachin J, Cleary P, Crofford O, Davis M, Rand L, Siebert C. Tocci G, Paneni F, Palano F, Sciarretta S, Ferrucci A, Kurtz T, Mancia G, Volpe or in favour of an aggressive approach. Effects of blood pressure lowering on its components: a meta-analysis of 50 studies and 534,906 individuals. Statins and risk of incident diabetes: a collaborative meta-analysis of rando 181. Efficacy and safety of alirocumab in insulin-treated individuals with type 1 or 185. Diabetes Care versus pravastatin (20 mg twice daily) in patients with previous statin intoler-. A, Young A, Lay M, Chen F, Sammons E, Waters E, Adler A, Bodansky J, Collins R, Keech A, Simes J, Peto R, Armitage J, Baigent C. Farmer A, McPherson R, Neil A, Simpson D, Peto R, Baigent C, Collins R, cholesterol-lowering therapy in 18,686 people with diabetes in 14 randomised. Halvorsen S, Huber K, Morais J, Patrono C, Rubboli A, Seljeflot I, Sibbing D, patients with insulin-treated diabetes. Zaccardi F, Rizzi A, Petrucci G, Ciaffardini F, Tanese L, Pagliaccia F, Cavalca V, 218. In vivo platelet activation and aspirin responsiveness in type 1 diabe impact on platelet reactivity of twice-daily with once-daily aspirin in people. Multimodality imaging in diabetic Mattoscio D, Zaccardi F, Liani R, Vazzana N, Del Ponte A, Ferrante E, Martini F. Gyberg V, De Bacquer D, De Backer G, Jennings C, Kotseva K, Mellbin L, recovery of platelet cyclooxygenase activity explains interindividual variability in. Patients with coronary artery disease and diabetes need improved Haemost 2011;106:491A499. Risk fac volume, distribution width, and count in type 2 diabetes, impaired fasting glu-. Reduced risk of heart failure with intensified multifactorial intervention in indi-. Ueki K, Sasako T, Okazaki Y, Kato M, Okahata S, Katsuyama H, Haraguchi M, 2006;295:306A313. Evidence-based medication and revascularization: powerful tools in the manage Stevens W, Buck G, Barton J, Murphy K, Aung T, Haynes R, Cox J, Murawska. Lancet Diabetes year outcome in patients with coronary artery disease: a report from the Euro. J Thorac Cardiovasc Surg Task Force on the management of stable coronary artery disease of the. Alogliptin after acute coronary syndrome in patients Martinez F, Masson C, Mazzone T, Meaney E, Nesto R, Pan C, Prager R, Raptis. Effect of linagliptin vs placebo on major cardiovas Secondary prevention of macrovascular events in patients with type 2 diabetes. Linagliptin effects on heart failure and related outcomes in individuals with type dial infarction in 2,445 patients with type 2 diabetes and previous myocardial. Pioglitazone use and heart failure in patients with type 2 diabetes and preexist-. Oral semaglutide Cordera R, La Macchia O, Zamboni C, Scaranna C, Boemi M, Iovine C, Lauro. Published online ahead of print 11 June R, Dotta F, Di Benedetto A, Citro G, Antenucci D, Ricci L, Giorgino F, Santini. Hall S, Rao-Melacini P, Wong G, Avezum A, Basile J, Chung N, Conget I, from a Diabetes Care Editors Expert Forum.
Diseases
- Cecato De lima Pinheiro syndrome
- Carnosinase deficiency
- Cystic hygroma
- Ankylosing vertebral hyperostosis with tylosis
- Fox Fordyce disease
- Dysostosis peripheral
- Covesdem syndrome
- Cleft lip palate abnormal thumbs microcephaly
- Pancreatic islet cell tumors
- Finnish lethal neonatal metabolic syndrome
Purchase discount differin online
Totally unable to bear weight both immediately can pretty confdently say that muscle A is not the after injury & (for 4 steps) in the emergency problem here skin care with honey generic 15gr differin fast delivery. To recap: in your repertoire, you have the Ottawa Ankle Rules (highly sensitive) and a radiograph (highly specifc). So when you couple these two types of tests together, you can arrive at a clinical decision that is strongly supported by the literature: one test rules a pathology out; the other test confrms the diagnosis of the pathology. Greater than 75% may be helpful when clustered with other tests, but metrics around 50-60% are no better than a coin toss and clearly we don?t want to make clinical decisions with a coin toss! Hopefully this has made the concept of statistics a little bit easier for you, and has helped you see their clinical relevance. It is essential, when we have a client come to us with an upper extremity problem, we make sure to rule out those For each one of the warning signs, there are many conditions that are beyond our scope. As clinicians we need to confrm signs and symptoms that point to a given diagnosis. A only pathology that radiates into the shoulder or down thorough low back examination would be appropriate the arm. There are numerous pathologies that produce to rule out mechanical mechanisms for the signs or upper extremity pain. Likewise, when may be specifc to certain periods of time within the we look at O, an obvious change in a wart or mole, lifespan and others may occur at any time. Whenever someone has a (multiple color tones), a diameter greater than six diagnosis of cancer in their history, you always have to millimeters, or a change in status. If I told you that six millimeters is the size of a pencil eraser, you get an idea in your head of the size of a lesion that should concern you. If this is the frst time you have seen this client, you are going to have to rely on his/her knowledge of the situation. You may have to ask the client if there has been a change in the wart or mole (size, shape, coloration) in the past few weeks or months. When you look at these images, you can see the different criteria for concern: multiple pigmentations, irregular borders, asymmetrical shapes. Now as a therapist, it doesn?t really matter what the labels are on these lesions. You need to recognize this is outside of your scope of practice and see to it that the client is referred to the appropriate medical professional. While skin cancers are among the more obvious For the forearm rolling test, you make a fst, hold your referrals, we have the ability to screen for other cancers forearms out in front of you in a horizontal position, as well. Maranhao, Maranhao-Filho, Lima, and Vincent and roll the forearms around each other. If one arm (2010) conducted an interesting study that looked at orbits around the other in an asymmetrical movement, 13 different clinical tests on the detection of unilateral the test would be positive. They actually found that the specifcity index fngers are held out in front in a horizontal was quite high for a variety of the tests studied. Again, a positive test is an asymmetrical motion of one fnger orbiting around the other. For fnger tapping, the client is asked to take the index fnger to thumb and doing a quick tapping motion as many times as possible for ten seconds. A greater than fve-rep difference between the right and left hands is a positive test. Foot tapping involves tapping your foot on the foor for ten seconds and looking to see if there is a fve-rep difference between the right and left feet. These are just a few examples, really simple things that can be done to screen for a brain tumor. As being said, it is important to remember that when you you can see from the statistics, all six of the tests have hear hoof beats, think horses, not zebras. The brain tumor is the zebra but in seconds to assess the likelihood of a unilateral brain there are grave consequences to missing this diagnosis. Likewise, positive predictive values the liver and gallbladder are in the right upper coupled with the high specifcity make these superb quadrant. In order to palpate these positive, a dialogue with the primary care physician structures, we need to get the rib cage out of the way. The way to do that is to have the client take a big deep breath, so that the ribcage elevates: now you can press In addition to cancer, there are several other medical inward and get to the gallbladder and liver. When we speak Liver Palpation about red fags in medical screening, we will defne a red fag as a sign or symptom that is a strong predictor of pathology. If you are a middle-aged adult, chances are you have had many headaches over the course of your life span. So a headache may not be a big concern for an adult but it may be a red fag for a three or four year old child. Gulick, iOrtho+ Mobile App, 2016 In addition, the heart refers to the left shoulder, and Murphy Technique so does the spleen. So we need to make sure that when a client reports left shoulder pain, we rule out cardiac and spleen dysfunction. Is there a family history of cardiac disease, any signs or symptoms of cardiac pathology, or any type of trauma to the thorax that could relate to spleen damage? The mid-thoracic region can be coming from the Gulick, iOrtho+ Mobile App, 2016 stomach; the right lower quadrant from the appendix. The musculoskeletal problem, we should frst rule out the other technique is called the Murphy technique, in possibility of visceral pathology. The clinician can come up from the iliac crest and move proximal towards the rib cage. If the client takes a breath, the ribs will elevate and an enlarged spleen will be revealed. Even the possibility of breast below represents some of the side effects of statins. Trouble talking & enunciating words important in the screening process that when we. Blinding headaches In reviewing this list, it is not hard to see that these effects appear in a large number of clients who present for treatment of physical limitations. Onset of these effects after the recent prescription of statins or an If you do in fact palpate such an entity, this would increase in the dosage of a statin may warrant a be the time to then talk to the client in greater detail conversation with the prescribing physician. Statin use has Finally, as you know, identifying the medications been associated with a 22-55% reduction in various a client is taking is very important. In addition, cancer deaths in women and when combined with ascertaining any recent change in medications can the anti-diabetes medication, metformin, found a 40% yield information about toxicity and/or side effects. Individuals who have taken a daily aspirin for 20 year have shown a 50% reduction in the risk of colon cancer. Finally, with regard to medications, the clinician must recognize the overall impact of any medication taken in combination with another. The cytochrome P450 enzymes are essential for the metabolism of numerous medications; this class has more than 50 enzymes, yet six of them are responsible for the metabolism of 90% of drugs. Interactions between beta-blockers and anti depressants, Plavix and Tylenol, and many others can occur. In addition, interactions can occur with non drug substances such as caffeine and alcohol. Free mobile apps such as Medscape and Epocrates are available for the Penn Shoulder Score was developed by mobile devices to render access to copious amounts of Brian Leggin in 1999; he specifcally states in his pharmaceutical information to aid your clients in the publication that he grants unrestricted use of this recognition and prevention of drug related side effects/ questionnaire for client care in clinical practice interactions. As we discussed previously, toolbox questionnaires can be very helpful in clinical practice because they give you information about many parameters other than just pain. In this particular case you would have a client rate each area from 0 to 10, then total the question scores, and divide by the number of questions that they answer (they can leave some questions blank, so the denominator may change from client to client). You then multiply by one-hundred: the higher the score, the greater the level of impairment. You summate the responses, divide by the total responses, subtract 1, multiply by 25, and that gives you a score. For example, if an individual indicates to you that his/her pain level went down from a 7 to a 5, what does that mean? A helpful toolbox questionnaire for the elbow is the Elbow Evaluation. In the instability section there are a number of questions about functional tasks. Incorporating this into your examinations can be helpful in seeing the big picture of a client. Toolbox questionnaires for the wrist and hand include the Patient-Rated Wrist Examination.
Buy differin now
The half-life of drugs in the aqueous 50% Systemic 10% Ocular is only a few hours skin care 8 year old discount differin 15 gr without a prescription, but effective concentrations of antibiot Conjunctiva & nose ics may last for 1?4 days when injected into the vitreous. Systemic Administration Infammations or infections involving the posterior ret ina, optic nerve or orbit that cannot be reached by local Conjunctiva: large Cornea: small hydrophilic molecules lipophilic molecules applications require systemic therapy. Large-sized molecules (such as penicillin) are not allowed to pass and when the molecular size is at the Drugs may be incorporated into carriers such as water borderline, lipid-solubility is again the most important soluble hydrophilic polymer inserts, collagen shields, water determining factor. Among the common antibiotic drugs, soluble vinyl alcohol flm inserts, liposomes and microparticu chloramphenicol, which is lipid-soluble, enters the eye lates which can remain in contact with the epithelium for many easily. Among the antimicrobial drugs many are bacteriostatic, but some are bactericidal, acting by competing for the raw Subconjunctival Injections materials necessary for the existence of the organisms. As these enable a wider range of substances to be introduced soon as the infuence of the drug is withdrawn, the remain into the eye, as the sclera allows the free and indiscriminate ing organisms may resume growth and multiply, so the transit of molecules of considerable size. Thus, antibiotics rationale of treatment is to keep the drug continuously in which do not penetrate the cornea enter the eye freely by contact with the infected tissue until the infection is this route. Since these drugs are rapidly excreted from the tions of antibiotics or steroids are required as in acute body or diffuse from any site of local application, repeated anterior segment infections and infammations. Bactericidal antibiotics are the penicillins, aminoglycosides, fuoroquinolones, and cephalosporins, Peribulbar/Sub-Tenon Injections while erythromycin, sodium sulphacetamide and trime Both anterior sub-Tenon and posterior peribulbar/retrobul thoprim are bacteriostatic. A short, curved needle with its bevel towards the ment of acute infections; in chronic infections they are rela globe is passed through a conjunctival incision and tively ineffective or a relapse follows their withdrawal. These the antibiotics are a class of substances derived from injections are used in the treatment of intermediate and fungi or other bacteria or are synthetic. Depots of crystalline suspensions on the inhibitory effect which one organism exerts on another. Other antimicrobial most cocci other than penicillinase-producing staphylo agents are effective against spirochaetes, rickettsiae, fungi and cocci, Neisseria and partly Escherichia coli. In general, effectivity against gram-positive organ isms is seen with penicillin G, erythromycin, oxacillin and Their intraocular penetration is good. Carbenicillin vancomycin, while neomycin, polymyxin B, azlocillin and sodium, ticarcillin and azlocillin are given parenterally and streptomycin are largely effective against gram-negative act against Pseudomonas aeruginosa. The broad-spectrum antibiotics?gentamicin, Penicillins show a synergistic action with antibiotics amikacin, ampicillin, cephalosporin, tobramycin, chloram of the aminoglycoside group. In deep-seated infammations phenicol, tetracycline, fuoroquinolones and others?are of the orbit or lids, they are administered parenterally. Cloxacillin and fucloxacillin: these penicillins are not Most of the currently available antibiotics are extremely affected by staphylococcal penicillinase and are therefore effective for conjunctival and corneal infections, and should used for treating staphylococcal infections which are resis be prescribed to be used every 1?2 hours for a few days and tant to other penicillins. If a fuoroquinolone or aminogly against penicillin-resistant staphylococci as cloxacillin, but coside drug does not show clinical effcacy, the drug should levels of fucloxacillin in the blood after oral administration be switched or a drug from another group added. This is because fucloxacillin is better absorbed from medications, their dosages and routes of administration. Serum levels following intramuscular or intra Penicillins venous injections of fucloxacillin are also higher than those All penicillins have a bactericidal effect, but have a short of cloxacillin. Differences in antibacterial activity, absorption Carbenicillin is resistant to the penicillinase produced and resistance to penicillinase depend on alteration of the by some strains of Proteus, Pseudomonas and coliform side-chains attached to the amino group. Most of them have a rather narrow antibacterial should be used for organisms which are resistant to benzyl spectrum, being chiefy confned to cocci and gram-positive penicillin but do not produce penicillinase. They diffuse readily into tissue fuids but not into Amoxycillin: this penicillin has an antibacterial activity the eye. When given systemically some have to be injected identical to that of ampicillin but its main advantage is intramuscularly because they are destroyed by the acidic that it is well absorbed after oral administration, producing gastric juice, others can be given by mouth. As patients are serum levels about twice as high as those after an equivalent liable to develop hypersensitivity to penicillin, it is wise to dose of oral ampicillin. Food in the stomach has little effect enquire about this before starting a course of treatment. The adult Immediate reactions such as urticaria and anaphylactic dose is 250?500 mg every 8 hours. Penicillins effective against coccal infections and drops effectively penetrate the vitreous. Oral gatifoxacin has gram-positive bacilli: Benzyl penicillin is not acidstable been shown to have extremely high levels in the vitreous. Penicillinase-resistant penicillins consist of cloxacillin these drugs have a structure and mode of action similar to sodium and flucloxacillin sodium. They are relatively resistant in their activity against penicillin-resistant staphylococci. Broad-spectrum penicillins such as ampicillin and penicillin may develop an allergy. When cephalosporins are amoxycillin are absorbed well orally and can also be used extensively, strains of staphylococci resistant to cloxa administered parenterally. The main adverse effect of of activity against many gram-negative organisms and gram cephalosporins is nephrotoxicity. All these agents are toxic to the eighth nerve and the hazolin and cephalexin, were highly effective against kidney, and interfere with neuromuscular conduction, causing gram-positive cocci, but moderately so for some gram serious paralysis in patients with myasthenia gravis or those negative enterobacilli. Intravitreal injec sporins, such as cefuroxime and cefaclor, had a wider tions are retinotoxic and may cause macular infarction. Some of the third-generation Streptomycin: this bactericidal drug is used in the cephalosporins. Thus, the drug Cephazolin is suitable for either intramuscular or intra should be used only after confrmation of in vitro suscepti venous administration. Cephradine can be given orally, intramuscularly or Soframycin is highly effective against gram-positive intravenously. Gentamicin: this drug may be used parenterally for the Ceftazidime acts against many gram-positive and gram treatment of serious infections by gram-positive and gram negative organisms, especially Pseudomonas. As the margin between toxicity and eff dose of 1?2 g intramuscularly or intravenously is given every cacy is narrow, it should be reserved for infections resistant to 8?12 hours. Because it is nephrotoxic and ototoxic and Cefuroxime and cefotaxime are available only as inject secreted through the kidneys, the dose must be decreased in able preparations. Gentamicin is effective against an exceptionally wide range of bacteria Aminoglycosides which includes penicillin-resistant strains of staphylococci this group includes streptomycin, soframycin, neomycin, and Ps. Pseudomonas strains show an increasing gentamicin, sisomycin, netilmycin, tobramycin and amikacin, incidence of resistance to gentamicin, therefore amikacin is Chapter | 13 Ocular Therapeutics 151 recommended for treating intraocular infections. Bactericidal methicillin-resistant Staphylococcus aureus and Staphylo concentrations are found in the aqueous following topical coccus epidermidis. As it may occasionally cause conjunctival necrosis, the It is the drug of choice in endophthalmitis together sub-Tenon route is recommended. It is toxic if used topically or Neomycin: this has similar properties to gentamicin subconjunctivally. It can be used topically, especially in combination with another antibiotic as eye Fluoroquinolones drops or ointment, but often causes contact allergy. These bactericidal drugs are derivatives of nalidixic acid and Sisomycin and netilmycin are similar to gentamicin, but have a broad spectrum of activity. Fortifed drops enhance treats a broad range of ocular pathogens, in conjunctivitis bioavailability and it can also be given sub-conjunctivally Haemophilus infuenzae, Staphylococcus aureus, Staphy or intravitreally. Because these drugs get deposited in the growing but is more retinotoxic than ceftazidime. For the treatment cartilage, they are not routinely recommended for treating of endophthalmitis, 0. Other Antibiotics Tetracyclines Chloramphenicol: this bacteriostatic antibiotic is effective Tetracyclines such as tetracycline, chlortetracycline and against bacteria, spirochaetes, rickettsiae, chlamydiae and oxytetracycline are broad-spectrum antibiotics with consid mycoplasmas. The molecule is small and lipid soluble so erable bacteriostatic action against both gram-positive and that on systemic administration it enters the eye in thera gram-negative organisms as well as some fungi, rickettsiae peutic concentrations. However, its effects on intraocular and the chlamydiae; the last group includes the infective infammations are usually not dramatic. Many bacteria have now developed spectrum for superfcial ocular infections and does not resistance to these drugs. Of all topical lar tissues either from the conjunctival sac or after systemic antibiotics, it is the least toxic to the corneal epithelium.
Buy differin 15gr amex
The shoulder joint is enclosed in a capsule that is lubricated on the inside and possesses a large fold underneath the joint acne laser treatment generic 15 gr differin visa. The capsule also includes ligaments and several small muscles collectively called rotator cuff muscles (supraspinatus, which is located above the bony spine of the scapula, infraspinatus, teres minor, and subscapularis) that wrap around the shoulder blade, inserting into the top of the humerus. Their function is to hold the ball of the arm bone against the socket and ensure its central position. Small rotator cuff muscles work in opposition to such powerful muscles as deltoids, biceps, and triceps, all of which pull the arm bone upward into the shoulder socket, counterbalancing gravity and the weight of the arm. Holding the instrument and the arms in front of the body for many hours will result in the overdevelopment of the deltoids, triceps, biceps and even pectoral muscles. Rotator cuff muscles will not be able to withstand such power and will cease to work efficiently in opposition to these excessively strong muscles. Gradually, the head of the humerus will start to be positioned too high and too far forward. Infraspinatus and teres minor (two of the rotator cuff muscles responsible for holding the head of the humerus in place) will become overstretched, weakened, and ineffective. Paull emphasizes that this situation is caused by playing long hours and not by poor technique 37 or excessive tension. Obviously, it is essential to take care of the body, to exercise and counter the pressure exerted upon musculoskeletal system by playing. Otherwise, this muscle imbalance will destabilize the shoulder joint, unavoidably leading to pain, and can be the initial culprit for most shoulder injuries such as shoulder impingement syndrome, rotator cuff tears, bursitis, etc. There is also another important factor to consider when discussing shoulder problems, or in fact, the mechanics of playing an instrument and any other playing related injuries. Patrone believe it is essential to 37 Paull and Harrison, the Athletic Musician, 74. Static load involves continuous muscle contractions and stress across a joint and its supporting structures. Dynamic load refers to the stress across a joint and its supporting structures resulting from movement, especially high-frequency and forceful movements. Holding and playing the violin or viola requires constant muscle contraction in the left shoulder as well as the neck for extended periods of time, and that is an example of static load (for further information on the neck, see below). This can be explained by the fact that the bowing arm is subjected to both static and dynamic loads (it is mostly held in an abducted position?moving away from the middle?and it is performing more repetitive motions as well, and thus at higher risk of injury). Four potential shoulder problems that most commonly trouble instrumentalists include shoulder impingement syndrome, subacromial and subdeltoid bursitis, bicipital tendonitis, and rotator cuff syndrome. It is important to realize that a shoulder injury may also cause pain in the arm, hand, and neck since the muscles that move the shoulders and 39 the neck (trapezius, rotator cuff muscles, and deltoids) work together. According to Horvath, tendonitis of the shoulder muscles is the most common cause of shoulder pain. This injury may occur as a result of the repetitive use of the arm at or above the shoulder level. Reduced blood supply caused by these motions leads to inflammation and microscopic tissue tears, as well as calcium deposits. Bursae are fluid-filled sacks that allow for the smooth action of tendons and ligaments, facilitating efficiency of motion by reducing friction between ligaments and bones. Holding the arm overhead or away from the body for long periods of time contributes to squeezing the rotator cuff muscles and the bursae at the shoulder joint. Inflammation may occur as a result of it, leading to thickening of the bursa and may change its texture from smooth to fibrous. This condition is called bursitis and causes radiating pain down the upper arm as well as restriction of movement. Rotator cuff tears appear among musicians usually as the result of repetitive strain and previous tendonitis injuries. As rotator cuff muscles become thinned and weakened, the tendons will gradually rip (as Horvath notes, the possibility of this injury significantly increases if a person is physically inactive). This injury causes pain starting at the shoulder and continuing down the upper arm, weakness of the arm, and the inability to raise it. Shoulder impingement syndrome occurs when the tendon of one of the rotator cuff muscles (supraspinatus) is pinched. Supraspinatus, which lies above the ridge (spine) on the surface of the scapula, reaches across the top of the humerus before connecting to the arm bone towards the front. Supraspinatus muscle travels within a rigid tunnel created by the shoulder joint and acromion, and is protected by a bursa. When the 47 head of the arm bone moves too high in its socket (this occurs when the arm is lifted), the supraspinatus tendon is pinched against the acromion, about halfway through the movement. Yoga and Shoulder Many serious problems for instrumentalists, especially upper string musicians, occur in the shoulder joints. The practice of Yoga may be used as an effective method for dealing with challenges of shoulder injury prevention and treatment. The remainder of this chapter will investigate the following three articles that offer convincing evidence in support of this claim: Shoulder Saver: How a Down Dog Each Day Keeps Painful 41 Injuries at Bay, by Julie Gudmestad, Headstand for Rotator Cuff Tear: Shirshasana 42 or Surgery, by Loren M. I will also supplement this information with observations drawn from my own research and experience of Yoga practice. Gudmestad explains that teres minor and infraspinatus control the external rotation of the shoulder, and if they are not exercised properly, they eventually weaken, leading to impingement syndrome, tendonitis, or bursitis injuries. Weakened and torn tissues of the muscle are extremely difficult to repair (sometimes even doctors compare this kind of surgery to attempts to sew up a run in a nylon stocking). Gudmestad proposes that teres minor and infraspinatus, as well as other rotator cuff muscles, are strengthened in Adho Mukha Svanasana (Downward Dog Pose). To understand the correct way of engaging the external rotators in Downward Dog, Gudmestad suggests trying it outside of the asana. She recommends standing facing a table or a desk, then leaning forward and placing the hands on it, palms down, bearing little weight. Then she advises looking at the elbows while noticing the crease on the inner sides and points of the elbows on the outer sides. The shoulders are externally rotating if the arms are rotated in such a way that the creases point forward. Many Yoga students slip (even while in Downward Dog) into internal rotation, which leaves teres minor and infraspinatus inactive. To remedy these problems, Gudmestad suggests oscillation between external and internal rotation, while practicing on the table with little 49 application of the weight. Gudmestad believes that it is possible to feel these muscles 44 contract across the back of the shoulder blade during external rotation. After learning to recognize the sensation of engaging the teres minor and infraspinatus, the next step is to practice the actual pose. Start by standing in Mountain Pose (for description of this asana, see Chapter 1 p. Bring the palms down to the floor, place them next to the outer edges of the feet or slightly in front of them, and allow the knees to bend further if needed. Straighten the arms (the index fingers are parallel), push the hips up, and lengthen the spine from the sacrum through the top of the head. While in this position, breathe deeply, gaze at the navel, and slightly press down the knuckles of the index fingers and thumbs. The shoulder blades slide slightly down toward the tailbone and away from each other, widening the back and creating space around the neck. For very advanced practitioners who are able to perform the ultimate version of this pose, the head reaches the floor, the feet are placed also on the floor, and the legs remain straight. If this does not occur comfortably and it will be the case for the majority of Yoga students one needs to allow either the knees to bend slightly or work in the direction of reaching the floor with the heels (without them actually touching the floor) while keeping the legs straight. After staying in this pose for about a minute and breathing deeply, rest in Child Pose (Balasana). Bring the knees to the floor, push the hips 51 back and sit lightly on your heels. To make this position more comfortable, one may allow the knees to move a little out or slightly raise the hips.
Cheap differin 15 gr mastercard
The stent Dr Palmberg: I believe we have consensus that the canal is supplied preloaded in an inserter that incorporates a based and suprachoroidal procedures are best suited for 27-gauge needle acne yahoo answers buy discount differin 15gr on line. They offer a great opportunity to safely now and can attest to the safety of this approach. I have been reasonably hydrophobic, it must be primed at the time of implantation. I like the fact that I can the device is in late-stage clinical development in the United avoid external cautery, which can both promote infammation States and is therefore not approved or available here, nor is it and induce astigmatism. The fbrosis is focally located at conducted a pilot study in the Dominican Republic and published 3-year data from that study. For instance, if we could measure distal implantation technique is familiar to surgeons who insert a lot outfow resistance, we might be able to identify patients who of tube shunts. If we better understood why suprachoroidal fltration procedures fail, Dr Ahmed: this device is a microtube without a plate. We still lose a number I have learned from performing the implantation procedure of trabeculectomies to wound-healing complications, so is that the plates limit bleb size. Glaucoma is a long-term disease, so of aqueous and controlled fow from the implant. Another I think we will need longer-term data?similar to the 5-year key factor is tube position. I prefer for the external tip to be data from the Tube Versus Trabeculectomy study33,42?to adequately posterior to produce a more posterior bleb, and better guide our surgical decisions on an individual patient I carefully place it under Tenon layer to avoid entrapment basis. With Dr Barton: Along those lines, I would like to see long-term experience, we will better understand what, if any, are the data on the durability of these new microtubes. For those glaucoma will be critical to determine their role in the treatment portfolio. We could review the expected outcomes the scleral fap and suturing it can induce astigmatism. It is gratifying to see a high proportion Summary and Take-Home Points of patients return to baseline vision within a few days after surgery with either of these microtube devices. Performance and safety of a new ab interno gelatin stent in refractory glaucoma at 12 months. Minimally invasive glaucoma surgery term follow-up will be needed to compare their outcomes with as primary stand-alone surgery for glaucoma. The effect of change in intraocular pressure on the natural References history of glaucoma: lowering intraocular pressure in glaucoma can result in improvement of visual felds. Update on minimally invasive glaucoma of ab interno trabeculectomy using a novel dual-blade device. Randomized evaluation of the trabecular micro-bypass phacoemulsifcation cataract surgery. Three-year follow-up of a novel aqueous prostaglandin: outcomes through 36 months. Adverse effects and risk factors for failure of standalone ab interno gelatin microstent of topical antiglaucoma medication. Treatment outcomes in the early surgery compared with laser and medicine in open-angle glaucoma. The relationship between control of intraocular pressure and Study comparing initial treatment randomized to medications or surgery. Reduction of intraocular pressure mitomycin C 1-year follow-up: result and complications. The Ocular Hypertension combined glaucoma and cataract surgery: clinical results of the smallest Treatment Study: a randomized trial determines that topical ocular ab interno gel stent [published online ahead of print May 29, 2017]. Which of the following skills is essential for the new glaucoma medication reliance for up to years. Your comments help us to determine the extent to which this educational activity has met its stated objectives, assess future educational needs, and create timely and pertinent future activities. This ensures that your certifcate is flled out correctly and is e-mailed to the proper address. They are used strictly for conducting post-activity follow-up surveys to assess the impact of this educational activity on your practice. If you answered Yes, we urge you to be specifc about where the bias occurred so we can address the perceived bias with the contributor and/or in the subject matter in future activities. Please list one or more things, if any, you learned from participating in this educational activity that you did not already know. As a result of the knowledge gained in this educational activity, how likely are you to implement changes in your practice? Related to what you learned in this activity, what barriers to implementing these changes or achieving better patient outcomes do you face? Please check the Core Competencies (as defned by the Accreditation Council for Graduate Medical Education) that were enhanced for you through participation in this activity. Complete, round capsulotomies are and tip that produces a quick, elegant, round capsulotomy in milliseconds. Very little stress on the zonules was observed during application of suction, capsulotomy, and suction release. Precision pulse capsulotomy preclinical safety and performance of a new capsulotomy technology. Comparison of manual, femtosecond laser, and precision pulse capsulotomy edge tear strength in paired human cadaver eyes. K1-5011 15mm blades Temporal Approach Wire Speculum with spring on nasal side K1-5012 15mm closed blades K1-5015 15mm open blades K1-5014 15mm solid blades 1 K1 Speculums Solid Blade Wire Speculum K1-5020 Barraquer, 10mm blades K1-5030 Barraquer, 15mm blades K1-5032 Feaster, 20mm blades (not shown) K1-5020 K1-5030 Kratz-Barraquer Wire Speculum 15mm blades one solid and one open wire K1-5044 for right eye K1-5045 for left eye right left Kratz-Barraquer Wire Speculum with open blades For unobstructed access to the cataract incision with phaco or I/A tip. K1-5049 heavy wire, 15mm blades (not shown) K1-5050 standard wire, 15mm blades K1-5051 standard wire, 13mm blades K1-5050 K1-5051 2 K1 Speculums Kratz-Barraquer Wire Speculum with wings For retracting the lids up and away from the globe to eliminate external pressure. K1-5060 15mm blades McIntyre Wire Speculum gently curved springs V-shaped blades are designed to retain surgical drape under the eyelids. K1-5070 closed wire, 13mm blades K1-5071 open wire, 13mm blades Nevyas Wire Speculum Designed to retain surgical drape under the eyelids while allowing unobstructed access to the cataract incision with phaco or I/A tip. K1-5073 16mm blades 3 K1 Speculums Lieberman Style, aspirating adjustable mechanism Features aspirating ports to remove excess fluid from the surgical field. K1-5171 Lieberman, Kratz style, 15mm blades K1-5173 Thorlakson, rounded, 11mm blades K1-5175 Lieberman, V-shaped, 15mm blades K1-5180 Chu, solid, reversible, 15mm blades K1-5179 replacement silicone tubing, 100cm (39) K1-5171 K1-5173 K1-5175 K1-5180 Double-X Aspirating Speculum adjustable, Kratz style 15mm blades K1-5191 4 K1 Speculums Sauer Lid Speculum K1-5300 for infants, 11mm blades K1-5302 for premature infants, 2mm blades Frankel Infant Lid Speculum adjustable For precise control of infant eyelid retraction. K1-5310 10mm blades Infant Wire Speculum interlacing 3mm & 5mm blades For use with newborns or infants. K1-5330 Alphonso Infant Lid Speculum 7mm finger grips and interlacing blades to facilitate insertion one blade 5mm, one blade 7mm K1-5340 5mm 5 K1 Speculums Infant Lid Speculum closed wire blades gently curved spring K1-5350 4mm blades Femto Lid Speculum flat 15mm wire blades with locking screw K1-5390 Cook Eye Speculum with locking screw K1-5401 #1, 8mm blades K1-5402 #2, 11mm blades K1-5403 #3, 15mm blades (not shown) 6 K1 Speculums Murdoch Eye Speculum with locking screw K1-5406 #2, 12mm blades K1-5407 #3, 15mm blades Mellinger Eye Speculum self retaining For unobstructed access to the cataract incision with phaco or I/A tip. K1-5411 15mm blades 7 K1 Speculums Williams Eye Speculum with locking screw K1-5500 11mm blades K1-5510 15mm blades Lancaster Eye Speculum adjustable mechanism with locking nut K1-5600 16mm blades Lester-Burch Eye Speculum with flanges on blades for retaining eye lashes adjustable mechanism with locking screw K1-5620 8 K1 Lieberman Speculums K1-5660 Lieberman, infant K-wire, 5mm K1-5665 Lieberman, infant solid blade, 5mm K1-5668 Tanna-Lieberman, 15mm blades with traction suture anchor posts K1-5670 Lieberman, K-wire, 10mm blades, small K1-5671 Lieberman, K-wire, 15mm blades, standard K1-5672 Seltzer, flattened K-wire, 15mm blades K1-5673 Thorlakson, rounded, 11mm blades K1-5674 Lieberman, triple post, 13mm blades K1-5675 Lieberman, V-shaped, 15mm blades K1-5671 K1-5677 Lieberman, solid blades, 10mm blades (not shown) K1-5678 Lieberman, solid blades, 15mm blades K1-5679 Ginsberg, flared upper blades, fenestrated lower blades, 15mm blades Aspirating versions available, see page 4. K1-5660 K1-5665 K1-5668 K1-5670 K1-5672 K1-5673 K1-5674 K1-5675 K1-5678 K1-5679 9 K1 Speculums Reversible Eye Speculum nasal side adjustable mechanism non-reflective finish Designed for nasal or temporal placement. K1-5696 patent pending K1-5691 K-wire, 15mm K1-5695 V-wire, 15mm K1-5696 Chu, 17mm K1-5697 Chu, 13mm K1-5698 Solid blades Key Features: 1 Unique Double-X mechanism retracts blades in a parallel motion for even tension along the lid. K1-5711 15mm blades Maumenee-Park Eye Speculum with canthus hook blade locking screws may be positioned vertically or horizontally K1-5800 15mm solid blades K1-5810 15mm fenestrated blades (not shown) 12 K1 Speculums Smirmaul Eye Speculum individually adjustable blades for elevating eyelids Ideal for glaucoma surgery. K1-5950 15mm solid blades K1-5951 15mm wire blades (not shown) Schott Eye Speculum with rotatable adjustment for precise control of blade elevation Ideal for glaucoma surgery. K1-5955 16mm wire blades 13 K1 Fixation Rings Flieringa Scleral Fixation Ring K1-7100 set of eight, 15mm-22mm K1-7140 14mm diameter K1-7150 15mm diameter K1-7160 16mm diameter K1-7170 17mm diameter K1-7180 18mm diameter K1-7190 19mm diameter K1-7200 20mm diameter K1-7210 21mm diameter K1-7220 22mm diameter McNeill-Goldman Scleral Fixation Ring and Blepharostat K1-7311 small, 15mm I. K1-8480 1 small, 1 large (set) K1-8481 20 x 28mm, small (pair) K1-8482 22 x 30mm, large (pair) Jaeger Lid Plate clear plastic K1-8500 Jaeger Lid Plate stainless steel K1-8520 Wright Fascia Needle 1mm x 6mm oval hole 140mm long K1-8540 17 K1 Retractors Knapp Lacrimal Retractor 4 prongs K1-9000 blunt K1-9001 sharp Walton Conjunctiva Retractor 6mm wide thin solid blade K1-9008 Helveston K1-9010 Tissue Retractor thin curved blade K1-9010 Barbie 7mm wide K1-9012 Big Barbie 9mm wide K1-9019 Great Big Barbie 11mm wide concave blade K1-9019 18 K1 Retractors Stevenson Lacrimal Sac Retractor 3 x 3 blunt prongs, adjustable K1-9500 Stevenson Lacrimal Sac Retractor solid blades with serrated edge adjustable K1-9520 13mm blades Agricola Lacrimal Sac Retractor 3 x 3 sharp prongs K1-9550 19 K2 Knives Tooke Corneal Knife straight blade with curved cutting edge K2-3650 Corneal Dissector For intrastromal dissection. K2-3660 angled, straight blade K2-3660 K2-3661 K2-3661 angled, curved blade Gill Corneal Knife curved cutting edge K2-3700 straight K2-3710 light curve Fukasaku Hockey Knife sharp 3mm front edge semi-sharp 6mm bottom edge K2-3735 20 K2 Spuds. Burrs Foreign Body Spud K2-4000 Golf Club, angled, lightly rounded tip K2-4050 Francis, angled, flag shaped tip K2-4100 Ellis, lightly curved and rounded tip K2-4000 K2-4050 K2-4100 Spud & Gouge in reversible handle For removing foreign bodies. K2-6539 K2-6539 Sterilizing Case with silicone insert autoclavable plastic K2-6555 for one knife K2-6556 for two knives K2-6555 K9-2024 for three knives Diamond Knife Diamond Knife Diamond Knife Diamond Knife Diamond Knife 30 cutting edge 45 cutting edge tri-facet spear 10-facet 1mm wide 1mm wide 1mm wide 1mm wide 1mm wide K2-6560 K2-6561 K2-6565 K2-6567 K2-6568 25 K2 Diamond Knives Diamond Step Knife Diamond Step Knife Diamond Step Knife single 45 cutting edge tri-facet 10-facet 1mm wide 1mm wide 1mm wide K2-6540 K2-6546 K2-6548 Precalibrated depth settings: 0. Choppers Wheeler Double-End Spatula lightly curved K3-2120 Barraquer Iris Spatula round, smooth K3-2300 0. K3-2344 for use in the right hand K3-2345 for use in the left hand Escaf Nucleus Manipulator flattened olive-shaped tip angled at 45 K3-2347 Knolle Nucleus Spatula malleable stainless steel, flat 0.