
Lopid
Best 300 mg lopid
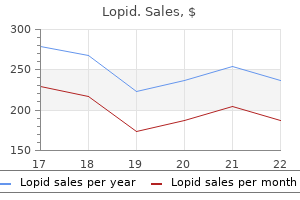
The Firm’s risk management governance and oversight framework involves Governance and Oversight Functions understanding drivers of risks treatment wpw generic 300 mg lopid with visa, types of risks, and impacts of the Firm manages its risk through risk governance and risks. The scope of a particular function may include one or more drivers, types and/or impacts of risk. For example, Country Risk Management oversees country risk which may be a driver of risk or an aggregation of exposures that could give rise to multiple risk types such as credit or market risk. The following sections discusses the risk governance and oversight functions in place to manage the risks inherent in the Firms business activities. Drivers of Risks Drivers of risks include, but are not limited to , the economic Risk governance and oversight functions Page environment, regulatory or government policy, competitor Strategic risk 84 or market evolution, business decisions, process or Capital risk 85–94 Liquidity risk 95–100 judgment error, deliberate wrongdoing, dysfunctional Reputation risk 101 markets, and natural disasters. The first line of defense is responsible for assess select strategic risks, credit risks and market risks. The Internal Audit Function is headed by the General Auditor, who reports to the Audit Committee. In addition, there are other functions that contribute to the firmwide control environment including Finance, Human Resources, Legal, and Control Management. The chart below illustrates the Board of Directors and key senior management level committees in the Firm’s risk governance structure. In addition, there are other committees, forums and paths of escalation that support the oversight of risk which are not shown in the chart below. The Committee’s responsibilities escalate to the Board the information necessary to facilitate include oversight of management’s exercise of its the Board’s exercise of its duties. Each committee of the Board oversees reputation risk and/or conduct risk issues within its scope of responsibility. The governance framework supports the consistent the Firm’s compensation programs and reviews and identification and escalation of fiduciary risk or fiduciary approves the Firm’s overall compensation philosophy, related conflict of interest risk. The regional committees are established operational risks, including existing and emerging issues similarly, as appropriate, for the region. Board of operational risk issues, focusing on processes with control Directors is responsible for the oversight of management of concerns and overseeing control remediation. Committee is responsible for monitoring the Firm’s overall balance sheet, liquidity risk and interest rate risk. The Risk Identification Capital Governance Committee is responsible for overseeing the Firm has a Risk Identification process designed to the Firm’s strategic end-to-end capital management and facilitate the first line of defense’s responsibility to identify governance framework, including capital planning, capital material risks inherent to the Firm, catalog them in a strategy, and the implementation of regulatory capital central repository and review the most material risks on a requirements. Strategic risk adjusted returns, strong capital and robust liquidity, is key includes the risk to current or anticipated earnings, capital, to management of strategic risk. For further information on liquidity, enterprise value, or the Firm’s reputation arising capital risk, refer to Capital Risk Management on pages from adverse business decisions, poor implementation of 85-94. For further information on liquidity risk, refer to business decisions, or lack of responsiveness to changes in Liquidity Risk Management on pages 95–100 the industry or external environment. For further information on reputation risk, refer to Overview Reputation Risk Management on page 101. As part of the strategic planning framework, and other relevant governance forums. Guided by the Firm’s How We Do Business Principles (the “Principles”), the strategic priorities and initiatives are updated annually and include evaluating performance against prior year initiatives, assessment of the operating environment, refinement of existing strategies and development of new strategies. These strategic priorities and initiatives are then incorporated in the Firm’s budget, and are reviewed by the Board of Directors. In the process of developing the strategic initiatives, line of business and Corporate leadership identify the strategic risks associated with their strategic initiatives and those risks are incorporated into the Firmwide Risk Identification process and monitored and assessed as part of the Firmwide Risk Appetite framework. For further information on Risk Identification, refer to Enterprise-Wide Risk Management on page 79. For further information on the Risk Appetite framework, refer to Enterprise-Wide Risk Management on page 80. The capital governance framework requires regular A strong capital position is essential to the Firm’s business monitoring of the Firm’s capital positions, stress testing and strategy and competitive position. Maintaining a strong defining escalation protocols, both at the Firm and material balance sheet to manage through economic volatility is considered a strategic imperative of the Firm’s Board of legal entity levels. The Firm’s Contingency capital plan fortress balance sheet philosophy focuses on risk-adjusted the Firm’s contingency capital plan, which is approved by returns, strong capital and robust liquidity. Senior management considers the the contingency capital plan defines how the Firm implications on the Firm’s capital prior to making any calibrates its targeted capital levels and meets minimum significant decisions that could impact future business capital requirements, monitors the ongoing appropriateness activities. In addition to considering the Firm’s earnings of planned distributions, and sets out the capital outlook, senior management evaluates all sources and uses contingency actions that must be taken or considered at of capital with a view to ensuring the Firm’s capital various levels of capital depletion during a period of stress. Board of Directors of the ongoing assessment of the Firm’s the Firm meets these objectives through the establishment processes for managing the sources and uses of capital as of internal minimum capital requirements and a strong well as compliance with supervisory expectations for capital capital management governance framework, both in planning and capital adequacy. The Firm’s Capital risk management is intended to be flexible in order Audit Committee is responsible for reviewing and approving to react to a range of potential events. These scenarios are articulated in terms of Regulatory capital macroeconomic factors, which are key drivers of business the Federal Reserve establishes capital requirements, results; global market shocks, which generate short-term including well-capitalized standards, for the consolidated but severe trading losses; and idiosyncratic operational risk financial holding company. The scenarios are intended to capture and stress minimum capital requirements for the Firm’s national key vulnerabilities and idiosyncratic risks facing the Firm. Accordingly, management generally follow the Capital Accord of the Basel Committee, considers additional stresses outside these scenarios, as as amended from time to time. While the tolerances; required capital remained subject to the transitional rules during 2018, the Firm’s capital ratios as of December 31. Performing independent assessment of the Firm’s capital 2018 were equivalent whether calculated on a transitional management activities; and or fully phased-in basis. The which are available on the Firm’s website second (“Method 2”), modifies the Method 1 requirements jpmorganchaseco. Certain banking organizations, including the Firm, 2018 2017 are required to hold additional amounts of capital to serve Fully Phased-In: as a “capital conservation buffer”. Total leverage financial environment in which large, internationally active exposure is calculated by taking the Firm’s total average on banks function. The Federal deducted for Tier 1 capital, and adding certain off-balance Reserve will continue to review the buffer at least annually. The amounts in the rollforward categories are estimates, based on the predominant driver of the change. Supplementary leverage ratio the table below presents the Firm’s assessed level of capital the following table presents the components of the Firm’s allocated to each line of business as of the dates indicated. Line of business equity (Allocated capital) December 31, December 31, (in millions, except ratio) December 31, 2018 2017 Tier 1 capital $ 209,093 $ 208,564 January 1, (in billions) 2019 2018 2017 Total average assets 2,636,505 $ 2,562,155 Consumer & Community Banking $ 52. On October 30, established as key measures of a business segment’s 2018, the Firm redeemed $1. On December 1, assumptions and methodologies used in capital allocation 2017, the Firm redeemed all $1. As of January 1, 2019, line of For additional information on the Firm’s preferred stock, business capital allocations have increased due to a refer to Note 20. There were no repurchases of warrants liquidated, resulting in $475 million of trust preferred during the years ended December 31, 2018, 2017 and securities and $15 million of trust common securities 2016. Year ended December 31, (in millions) 2018 2017 2016 On December 18, 2017, the Delaware trusts that issued Total number of shares of common stock seven series of outstanding trust preferred securities were repurchased 181. The Firm from time to time enters into written trading plans For additional information, refer to Note 19. A Rule 10b5-1 repurchase plan the Capital Management governance framework in line with allows the Firm to repurchase its equity during periods the Firm’s capital management objectives. All purchases under Rule 10b5-1 plans must be of Directors increased the quarterly common stock dividend made according to predefined schedules established when from $0. The Firm’s dividends are subject to the Board of Directors’ approval on a the authorization to repurchase common equity will be quarterly basis. The repurchase program does not Common dividend payout ratio 30% 33% 30% include specific price targets or timetables; may be Common equity executed through open market purchases or privately During the year ended December 31, 2018, warrant negotiated transactions, or utilizing Rule 10b5-1 plans; and holders exercised their right to purchase 14. The Firm issued from For additional information regarding repurchases of the treasury stock 9. There were no warrants Registrant’s Common Equity, Related Stockholder Matters outstanding at December 31, 2018, as any warrants that and Issuer Purchases of Equity Securities on page 30. Effective June 28, 2018, the Firm’s Board of Directors authorized the repurchase of up to $20.
300 mg lopid overnight delivery
Right anterior oblique view for visualization of the proximal common bile duct and the gallbladder Sonographic evaluation of the bile ducts should include the following fve images (Fig symptoms 6dpiui lopid 300 mg for sale. If there is excessive gas in the bowel, the patient should be examined standing (sitting will not usually displace bowel gas). In most patients, the gallbladder is best imaged using the liver as an acoustic window. It is recommended that the gallbladder be imaged with the patient in the supine, lef posterior oblique, lef lateral decubitus and semiprone positions. In each position, it is important to visualize the gallbladder neck, because stones may be hidden in this region. The interlobar fssure can be a valuable anatomical landmark for localizing the gallbladder when the latter is contracted or when it is small and flled with stones (Fig. Visualization with the patient on the hands and knees can demonstrate gallstones more clearly, as they can move anteriorly. The intrahepatic bile ducts travel in the portal triads adjacent to the portal veins and hepatic arteries. At the porta hepatis, the main right and lef hepatic ducts join to form the common hepatic duct. The common bile duct descends into the posterior and lateral aspect of the pancreas head before entering the ampulla. The term ‘common duct’ is used for the common hepatic duct and common bile duct together. In a longitudinal view of the porta hepatis, the common duct is seen anterior to the portal vein. The intrahepatic ducts are considered normal if their diameter is 2 mm or less and not more than 40% of the diameter of the adjacent portal vein (Fig. The common hepatic duct, high in the porta hepatis as it crosses over the right hepatic artery, has an internal diameter of less than 4 mm (Fig. A duct with a diameter of 5 mm is acceptable, while one with a diameter of 6 mm requires further investigation. It is divided into a fundus, a body and a neck, which continues into the cystic duct. The wall of the gallbladder consists of a mucosal layer (hyperechoic), a smooth muscle layer (hypoechoic), a perimuscular connective tissue layer (hyperechoic) and a serosal layer (hypoechoic). The intrahepatic gallbladder is usually in the plane of the interlobar fssure that divides into the right and lef lobe (see Fig. The transverse diameter of the normal gallbladder is less than 4 cm, while its longitudinal diameter is less than 10 cm; its wall thickness is less than 3 mm. The most accurate measurements of the gallbladder wall are made from the anterior subhepatic wall in a long-axis image (Fig. The diameter of the common duct is measured at its proximal portion (open arrow) in this view. The most accurate measurements are obtained from the anterior subhepatic gallbladder wall (arrows) in a long-axis or transverse image Pathological findings Gallbladder Stones Sonography plays the primary role in imaging the gallbladder. The typical sonographic appearance of gallstones is a mobile intraluminal echogenic focus with an associated acoustic shadow (Fig. Small stones attenuate the beam less than larger stones and therefore produce less well defned shadows. The patient’s position should be shifed during the procedure to demonstrate the presence of the stones as well as to diferentiate them from polyps and other entities. The echogenic line seen in the near feld is the gallbladder wall, and the echogenic line with posterior shadowing is a stone (Fig. The longest arrow indicates the perimuscular layer of the gallbladder wall, the intermediate arrow the lumen of the gallbladder or thickened muscular layer and the shortest arrow the anterior surface of stones Sludge Gallbladder sludge consists of a combination of cholesterol crystals and granules of calcium bilirubinate in thick, viscous bile. The sonographic appearance of sludge is that of amorphous, low-level echoes, with the gallbladder in a dependent position with no acoustic shadowing. Lack of internal vascularity, mobility and a normal wall are signs of the presence of sludge. The artefactual echo caused by the section thickness and side-lobe artefact can also mimic sludge. Tese artefacts can be reduced by appropriate focusing, by centring the gallbladder in the feld of view and by optimizing the gain settings. The sludge (arrows) is mobile, as seen by changing the patient’s position a b 175 Acute calculous cholecystitis this type of cholecystitis is caused by impaction of gallstones in the cystic duct or the gallbladder neck, resulting in obstruction, with luminal distension, ischaemia, superinfection and, eventually, necrosis of the gallbladder. The sonographic features of acute calculous cholecystitis include: calculi in the gallbladder; thickening of the anterior gallbladder wall; positive Murphy’s sign; distension of the gallbladder (volume > 70 ml); impacted stone in the cystic duct or gallbladder neck; pericystic fuid collection (sign of actual or impending perforation); intraluminal wall desquamation; and hypervascularization of the gallbladder wall on colour and power Doppler sonog raphy (Fig. Acute calculous cholecystitis: (a) a stone impacted in the gallbladder neck (short arrow) and thickening of the anterior gallbladder wall (long arrow); (b) hypervascularization of the gallbladder wall (arrows) is seen on power Doppler sonography a b Gallstones are the single most important fnding in cases of acute calculous cholecystitis. In the absence of stones, other sonographic fndings suggesting acute cholecystitis may indicate the need for cholescintigraphy. The sonographic Murphy’s sign refers to focal tenderness directly over the gallbladder when pressure is applied by the transducer; it has 94% sensitivity and 85% specifcity. To avoid a false positive for Murphy’s sign, it is best to apply pressure with the transducer over areas other than the gallbladder frst and then to compress the gallbladder. Murphy’s sign is positive in only 33% of patients with acute gangrenous cholecystitis. Occasionally, normal individuals have a thickened gallbladder wall due to poor postprandial distension of the gallbladder. On colour or power Doppler sonography, increased blood fow in the distal half of the gallbladder suggests acute cholecystitis. Although none of the signs described above is pathognomonic of acute cholecystitis, the combination of several fndings should lead 176 to the correct diagnosis. Acute acalculous cholecystitis The sonographic abnormalities in acalculous cholecystitis are similar to those in calculous cholecystitis, other than gallbladder stones. As the sonographic fndings in early acalculous cholecystitis may be subtle or nonspecifc, a follow-up examination 24–48 h later may be valuable. In the appropriate clinical setting, progressive wall thickening is highly suggestive of acalculous cholecystitis. In children, acute cholecystitis may be acalculous, with increased gallbladder-wall thickening, signs of hydrops, a positive sonographic Murphy’s sign and increased diameter of the common bile duct, with sludge. Gangrenous cholecystitis In 20–30% of patients with acute cholecystitis, gangrenous changes develop, which are characterized pathologically by intramural haemorrhage, necrosis and microabscess formation. Sonographic fndings in gangrenous cholecystitis include bands of non layering, echogenic tissue within the lumen, representing sloughed membranes and blood (Fig. The gallbladder wall is irregular, with small intramural fuid collections, which represent abscesses or haemorrhage. The gallbladder wall is difusely thickened, with an irregular, striated appearance (short arrows). In the gallbladder lumen, sludge is noted Perforation Gallbladder perforation occurs in 5–10% of cases and requires immediate cholecystectomy or percutaneous cholecystostomy because of the high mortality rate (greater than 20%). Diabetes, malignancy and use of immunosuppressive drugs predispose to perforation. The commonest site of perforation is the gallbladder fundus, because of its relatively poor blood supply. Sealed-of perforation, in which fuid leaking from the gallbladder is localized around it, is commoner than acute free perforation. The sonographic features of gallbladder perforation vary from a well circumscribed collection of fuid to a solid hypoechoic mass around a deformed gallbladder (Fig. Perforation of the gallbladder may extend into the adjacent liver parenchyma, forming an intrahepatic abscess collection (Fig. The ‘sonographic hole sign’, caused by focal interruption of the gallbladder wall, is a direct sign of perforation. Disruption of the gallbladder wall indicates a perforation site (white arrow) Emphysematous cholecystitis Emphysematous cholecystitis is a rare infection caused by gas-forming bacteria, such as Escherichia coli or clostridia, within either the wall or lumen of the gallbladder. Surgical or percutaneous intervention is required because of the poor prognosis and high mortality rate due to this condition. The sonographic fndings in emphysematous cholecystitis include echogenic lines with posterior ‘dirty’ shadowing in the gallbladder wall, with or without echogenic spots, and posterior ‘dirty’ shadowing in the gallbladder or a bright echogenic band with difuse acoustic shadowing within the gallbladder fossa (Fig. It may be difcult to diferentiate from a ‘porcelain’ gallbladder, except that the latter shows posterior clear shadowing. Cholecystoenteric fstula, which can have gas bubbles, does not result in intramural gas in the gallbladder.
Diseases
- Cogan syndrome
- Alopecia congenita keratosis palmoplantaris
- Chromosome 6, monosomy 6q
- Sutton disease II
- Mycosis fungoides
- Metaphyseal chondrodysplasia Schmid type
- Heart situs anomaly
- Atelosteogenesis, type II
- Sternal cleft
- Blamronesis
Order lopid without a prescription
A cross-sectional study with almost 3000 adolescents showed that the performance of several health-related fitness tests (handgrip strength symptoms 0f yeast infectiion in women best 300 mg lopid, bent arm hang, standing-long jump, 4x10m shuttle run test, and seat and reach) was higher in adolescents with high levels of cardiorespiratory fitness compared to those with lower levels of cardiorespiratory fitness (Ortega et al. Cardiorespiratory fitness is influenced by several factors including age, sex, health status, and genetics. It has been suggested that up to 40% of variation in the level of cardiorespiratory fitness is attributable to genetic factors (Bouchard et al. However, as stated before, the level of cardiorespiratory fitness is mainly determined by physical activity patterns. In children and adolescents, there is a positive association between objectively measured physical activity and cardiorespiratory fitness (Brage et al. Recent reports indicate that these findings are also valid in apparently healthy persons, and persons with a disease, such as diabetes mellitus, hypertension, metabolic syndrome and several types of cancer (LaMonte & Blair, 2006). High cardiorespiratory fitness during adolescence has also been associated with a healthier cardiovascular profile during these years, and also later in life (Castillo-Garzon et al. It has been suggested that cardiorespiratory fitness be included in the European Health Monitoring System for the adult population (Sjöström et al. The specific aims of the separate studies were as follows: To examine the associations of cardiorespiratory fitness with a clustering of metabolic risk factors in children, and to examine whether there is a cardiorespiratory fitness level associated with a low metabolic risk (Study I). Study design, sampling procedure, participation rates and study protocol have been reported elsewhere (Poortvliet et al. In Estonia, the city of Tartu and its surrounding rural area was the geographical sampling area. In Sweden, 8 municipalities (Botkyrka, Haninge, Huddinge, Nynäshamn, Salem, Södertälje, Tyresö, and Örebro) were chosen for data collection. Written informed consent was obtained from parents of the children and from both the parents of the adolescents and the adolescents themselves. Participants the basic characteristics of the participants and the variables examined in each sub-study are presented in Table 1. Skinfold thickness was measured with a Harpenden caliper (Baty International, Burguess Hill, U. All measurements were taken twice and in rotation, and the mean value was calculated. If the difference between the two measurements was more than two millimeters a third measurement was taken and the two closest measurements were averaged. Waist circumference was measured in duplicate with a metal anthropometric tape midway between the lowest rib and the iliac crest at the end of a gentle expiration. Identification of pubertal development was assessed according to Tanner and Whitehouse (Tanner & Whitehouse, 1976). Pubertal stage was recorded by a researcher of the same gender as the child, after brief observation. Breast development in girls, and genital development in boys, were used for pubertal classification. At least three days of recording, with a minimum of 10 hours registration per day, was set as an inclusion criterion. Total physical activity was expressed as total counts recorded, divided by total registered time (counts/min). The time engaged in moderate physical activity and vigorous physical activity was calculated and presented as the average time per day during the complete registration. Each minute over the specific cut-off was summarized in the corresponding intensity level category. Validation studies examining the accelerometer used in this study and the construction of summary variables for intensity of movement suggest that it is a valid and reliable measure of children’s and adolescent’s physical activity (Trost et al. The precision of objective assessment of physical activity in children is superior to subjective methods, however there are some limitations which should be highlighted. The accelerometer must be removed during swimming, contact sports, showering, and bathing. Four to five days of activity monitoring have been proposed as a suitable duration for accurate and reliable estimates of usual physical activity behavior in children (Trost et al. When expressed as energy expended in movement, heavier adolescents seem to engage in relatively large amounts of physical activity because they use more energy to move their bodies for a given amount activity compared to lighter adolescents. However, when physical activity is expressed as movement, heavier adolescents will appear to engage in less physical activity than lighter peers. The time spent in physical activity of various intensities seems more pertinent for purpose of making exercise recommendations (Ekelund et al. Cardiorespiratory Fitness Cardiorespiratory fitness was determined by a maximum cycle-ergometer test as described elsewhere (Hansen et al. The subjects cycled at 50-70 revolutions per minute on an electronically braked Monark cycle-ergometer (Monark 829E Ergomedic, Vansbro, Sweden). The test protocol was sex and age-specific, and is presented in detail in Table 2. The test was finished when the subject could no longer maintain the pedalling frequency of at least 30 revolutions per minute, even after vocal encouragement. Age Weight Initial work ǻ Work Stages Gender (years) (kg) rate (W) rate (W) (seconds) Girls & boys 9-10 < 30 20 20 180 Girls & boys 9-10 > 30 25 25 180 Girls 15-16 40 40 180 Boys 15-16 50 50 180 Kg, kilogram; W, power output; ǻ, increase. A true exhaustive effort was considered to have been achieved if the subject had a heart rate higher than 185 beats per minute, and at the same time the leader observed that the child could no longer keep up. The power output was calculated as: W1+ (W2 t/180), where W1 is the work rate at the final fully completed stage, W2 is the work rate increment at the final incomplete stage, and t is time in seconds at the final incomplete stage. However, cardiorespiratory fitness was also expressed as W/kg, as a more direct score. The test used has been previously validated in children of the same age (Riddoch et al. Blood Variables With the subject in the supine position, blood samples were taken by venipuncture after an overnight fast, using vacuum tubes (Vacuette, Greiner Lab Technologies Inc). Blood was centrifuged for 10 minutes at 2000 g, serum was separated within 30-60 minutes, and the samples were stored at -80qC. An appropriate cuff size was chosen according to the manufacturer’s recommendation after checking the arm circumference. Recordings were made every second minute for 10 or more minutes with the aim of obtaining a set of systolic recordings not varying by more than 5 mmHg. The mean value of the last three recordings was used as the resting systolic and diastolic blood pressure, in mmHg. Each of these variables was standardized as follows: standardized value = (value mean)/ standard deviation. The mean of the standardized values of systolic and diastolic blood pressure was calculated. The metabolic risk score was calculated as the mean of the six standardized scores separately for boys and girls. Children being below the 75th percentile of the score were defined as having low metabolic risk, and children being at or above the 75th percentile of the score were defined as having high risk. Other approaches have been made elsewhere in order to compute a clustering of metabolic risk factors in healthy children (Brage et al. We have computed a similar risk score that has been reported previously because of similarities in ages of the studied children, and study methodology (Brage et al. All variables were checked for normality of distribution before the analysis, and transformations were applied when necessary. The association between markers of insulin resistance and cardiorespiratory fitness was assessed by multiple regression analyses, separately by body fat and waist circumference tertiles. Moreover, the results suggest that a cardiorespiratory fitness level that confers a low metabolic risk is identifiable. The results also indicate that the deleterious consequences ascribed to high levels of total and central fatness could be counteracted by having high levels of cardiorespiratory fitness. The data call for the development and testing of preventive strategies, especially for those children with low cardiorespiratory fitness, and also reinforce the need to include cardiorespiratory fitness testing in national and European health monitoring systems. Cardiorespiratory Fitness and Metabolic Risk in Children (Study I) High cardiovascular fitness is associated with low metabolic risk score in children; the European Youth Heart Study. In the first study, the associations of cardiorespiratory fitness with a clustering of metabolic risk factors in children were studied, and we examined if there was a cardiorespiratory fitness level associated with a low metabolic risk.
Order lopid us
I (S)(R) elevated white cell count or other serological features of Primary Tumor of the Sacrum infection medicine 503 discount lopid amex, together with imaging evidence of the pres Code 533. X4pR Diagnostic Features Imaging or other evidence of arthritis affecting the sac roiliac joints. Usually deep and aching Hyperparathyroidism with “heaviness and numbness” in the leg from buttock Code 532. Page 189 System no evidence that the constrictive effects of spinal steno Musculoskeletal system. These latter forms of pain ostensibly arise from the disorders of one Main Features or more of the disks or zygapophysial joints whose os Patients usually have a long history of gradually increas teophytic overgrowth coincidentally causes the stenosis. Walking also pathology is restricted to a single intervertebral foramen produces overt or subtle neurological features in the and as such does not encroach upon the vertebral canal lower limbs that range from sensations of heaviness or as a whole. The onset of Treatment these neurological features may be measured in terms of Surgical decompression. Differential Diagnosis Peripheral vascular claudication, sciatic nerve compres Associated Symptoms sion, osteoarthritis of hip or knee, retroperitoneal tu There may be paresthesias and bowel or bladder distur mors, other tumor or abscess, prolapsed lumbar disk. X6*R Legs Signs and Laboratory Findings X-rays usually demonstrate diffuse severe degenerative disease with facet hypertrophy and a shallow anteropos terior diameter of the lumbar canal. The dilemma posed by this condition is the Definition discrepancy between physical signs, which are usually Sacral spinal pain associated with a congenital vertebral not great, and the subjective complaints. Diagnostic Features Pathology Imaging evidence of a congenital vertebral anomaly Encroachment upon and narrowing of the vertebral canal affecting the sacrum. Congenital narrowing of the There is no evidence that congenital anomalies per se vertebral canal may predispose to this condition insofar cause pain. Although they may be associated with pain, as symptoms may arise in the face of osteophytes and the specificity of this association is unknown. This clas syndesmophytes that in other individuals would not sification should be used only when the cause of pain cause significant encroachment. The mechanism of the cannot be otherwise specified, but should not be used to neurological features is unknown but may involve con imply that the congenital anomaly is the actual source of striction of the dural sac with obstruction of flow of the pain. X0*R other compromise of one or more nerve roots but there is Page 190 Pain Referred from Abdominal or sis. Sacral spinal pain associated with disease of an abdomi Patients given this diagnosis could in due course be ac nal or pelvic viscus or vessel that reasonably can be in corded a more definitive diagnosis once appropriate di terpreted as the source of pain. In some instances, a more definitive diagnosis might be attain Clinical Features able using currently available techniques, but for logistic Sacral spinal pain with or without referred pain, together or ethical reasons these may not have been applied. X8*S Diagnostic Features Imaging or other evidence of the primary disease affect ing an abdominal or pelvic viscus or vessel. Stressing the sacroiliac joint by clinical tests that are selective for the joint reproduces the patient’s pain, or Sacral Spinal Pain of Unknown or 3. Definition Sacral spinal pain occurring in a patient whose clinical Pathology features and associated features do not enable the cause Unknown. Presumably the pain is caused by excessive and source of the pain to be determined, and whose stresses being imposed on the ligaments of the sacroiliac cause or source cannot be or has not been determined by joint as a result of some structural fault in the joint itself special investigations. Remarks this category does not encompass sacroiliitis, ankylos Diagnostic Features ing spondylitis, or seronegative spondylarthropathies Sacral spinal pain for which no other cause has been that may be demonstrated by radionuclide imaging other found or can be attributed. While there are beliefs that such disorders can befall the sacroiliac joint, no clinical tests Remarks of laudable validity and reliability have been devised this definition is intended to cover those complaints that whereby this condition can be diagnosed. The presence for whatever reason currently defy conventional diagno Page 191 of such a condition, however, in the absence of any overt Code inflammatory joint disease, is implied by a positive re 533. Until such time as appropriate clinical tests are demon Reference strated to be valid and reliable, any diagnosis of sacroil Waisbrod, H. X8hS features and associated features do not enable the cause and source of the pain to be determined, and whose cause or source cannot be or has not been determined by special investigations. Definition Diagnostic Features Pain perceived in the coccygeal region, stemming from Coccygeal pain for which no other cause has been found one or both of the posterior sacrococcygeal joints. Diagnostic Criteria Remarks Complete relief of pain upon infiltration of the puta this definition is intended to cover those complaints that tively symptomatic joint or joints with local anesthetic, for whatever reason currently defy conventional diagno provided that the injection can be shown to have been sis. Patients given this diagnosis could in due course be ac Code corded a more definitive diagnosis once appropriate di 533. Definition Clinical Features Generalized spinal pain associated with a metabolic Generalized spinal pain with or without referred pain. Diagnostic Features Radiographic or other imaging evidence of multiple Clinical Features fractures throughout the vertebral column. Page 193 Clinical Features Signs Generalized spinal pain with or without referred pain. Diagnostic Features Imaging or other evidence of arthritis affecting the joints Laboratory Findings of multiple regions of the vertebral column. Definition Etiology Aching low back pain and stiffness of gradual develop Unknown; may be immunological, with possible envi ment due to chronic inflammatory change of unknown ronmental factors, along with apparent genetic suscepti origin. Chronic aching lumbar pain and stiffness with “gelling” System and with characteristic X-ray changes as described. Differential Diagnosis Main Features Psoriatic spondylitis; Reiter’s spondylitis; mechanical Prevalence in 1-2% of the population. X3bR back pain of insidious onset, aching discomfort, and stiffness while sleeping that forces the patient to get up and move around; morning stiffness is usually greater than half an hour in duration, and stiffness occurs also Back Pain of Other Visceral or after periods of inactivity (“gelling phenomenon”). Other entities to consider are radiation fibro Definition sis, lumbosacral neuritis, and disk disease. Progressively intense pain in the low back or hip with radiation into the lower extremity. The local Dull aching sacral pain accompanied by burning or pain is pressure-like or aching in quality. Main Features Pain in a sacral distribution usually occurs in the fifth, Associated Symptoms sixth, and seventh decades as a result of the spread of Typically, leg weakness and numbness occur three to bladder, gynecological, or colonic cancer. Sphincter distur aching midline pain and usually burning or throbbing bance is uncommon. The Signs and Laboratory Findings rectal and perineal component of the pain may respond There may be tenderness in the region of the sciatic poorly to analgesic agents. Focal weakness and sensory Associated Symptoms loss with depressed deep tendon reflexes may be evi With bilateral involvement, sphincter incontinence and dent. Signs and Laboratory Findings There may be tenderness over the sacrum and in the re An intravenous pyelogram may show hydronephrosis. It may show a paralumbar or pelvic soft tissue ment of S1 and S2 roots will produce weakness of ankle mass and there may be bony erosion of the pelvic side plantar flexion, and the ankle jerks may be absent. Myelography may be positive if there is epidural is usually sensory loss in the perianal region and in the extension of disease. Usual Course Summary of Essential Features and Diagnostic the pain and sensory loss may be unilateral initially Criteria with progression to bilateral sacral involvement and Low back and hip pain radiating into the leg is followed sphincter disturbance. The physical findings Social and Physical Disability indicate that more than one nerve root is involved. Page 195 Summary of Essential Features Differential Diagnosis the essential features are dull aching sacral pain with the differential diagnosis includes post-traumatic neu burning or throbbing perineal pain. There is usually sac romas in patients with previous pelvic surgery, pelvic ral sensory loss and sphincter incontinence. Psychological causes may play an important part in (See also 1-16) protracted low back pain in a large number of patients. They will, however, rarely be seen to be the sole cause of Code the pain, nor will the diagnosis emphasize them in the first 533. X l a Definition Hypoesthesia and painful dysesthesia in the distribution of the lateral femoral cutaneous nerve. Main Features Prevalence: more common in middle age, males slightly System more often than females. Pain Quality: all complaints are Main Features of pain or related sensations in the upper anterolateral Constant pain in the groin and medial thigh; there may thigh region; patients may describe burning, tingling, be sensory loss in medial thigh and weakness in thigh aching, numbness, hypersensitivity to touch, or just adductor muscles. Associated Symptoms Signs If secondary to obturator hernia, pain is increased by an Hypoesthesia and paresthesia in upper anterolateral increase in intra-abdominal pressure.
Buy lopid 300 mg line
This title most nearly captures the main idea of the passage and the author’s purpose in writing the piece medicine 2632 discount lopid 300mg visa. The passage clearly states that Wolfgang took an interest in the clavier when his sister was learning to play the instrument. In the second paragraph, the passage states that Wolfgang’s first public appearance was at Linz and that after this concert, word of his genius traveled to Vienna. The passage does not say anything about Wolfgang preferring one instrument to another. The third paragraph states that at the time, it was not uncom mon for child prodigies to have extensive concert tours. The main point of the passage is to describe Mozart’s experi ences as a child prodigy, or a highly talented child. The titles in choices a, b, and d all imply that the passage will provide information, which it does not. Choice c is the most ac curate choice because the passage deals mainly with remember ing the fair. Sentence 1 (choice a) contains the phrase should have been a colos sal failure, which is an opinion of the author. The sentence preceding and leading into sentence 3 speaks of the very brief time—a month—that the organizers of the fair had to find a new site and get information out. Choices b and d are incorrect because they could not have been known about at the time the fair was moved. Choice c is incorrect because there is no indication in the passage that New York officials tried to stop the fair. Nonfiction, on the other hand, refers to a piece of writing about something that did happen. History books and biographies are nonfiction because they address actual events and real people. Finally, informational writing refers to passages whose purpose is to inform the reader about something. Informational passages contain facts and figures, and include newspaper articles, business memos, legal documents, and so on. In this section, you will be dealing with nonfiction and information pas sages, such as the type you might find in a textbook. Some common purposes include: to inform to entertain to alert to persuade 8787 501 Reading Comprehension Questions found in standardized tests. These passages are not necessarily more difficult than the ones you’ve already covered in the earlier chapters of this book. However, they do call more heavily for the special skill of making inferences, of identifying implicit, as opposed to explicit, ideas stated in the text. What clues can you deduce from the writing style about the author’s attitude toward the subject? Try to pick out individual words that further each writer’s intent and support each writer’s opinion. Active reading techniques like these will keep you focused on some very detailed reading comprehension passages. It is technically a seed, produced by the coconut palm tree, and as such is one of the largest edible seeds produced by any plant. Its unusual contents also make it unique in the seed world—the interior consists of both “meat” and “water. Portuguese explorers gave the nut its name in the 15th century, referring to it as coco, meaning “ghost” in their language. The three dimples and the hairy texture reminded them of a ghost’s face, and the tree has retained that name ever since. It is used to make marga rine, as well as various cooking oils, and these cooking oils are used by fast-food restaurants around the world to make such diet staples as French fries. The coconut fluid is a favorite drink in hot climates, providing a cool and refreshing beverage right off the tree. This water is also used by manufacturers of various sports drinks because of its isotonic electrolyte properties. Coconut oil is used for cosmetics, medicines, and can even be used in place of diesel fuel. Dried coconut shells are used in many countries as a tool, such as a buffer for shining wood floors. The shells are also used for shirt buttons, and are commonly found 88 501 Reading Comprehension Questions on Hawaiian clothing. The coconut palm tree, which produces the nut, also produces countless useful items. Homeowners and renters know this basic fact, but they often don’t know what kinds of adjustments they can make in their homes and apartments that will result in savings. For those willing to spend some time and money to reap long term energy savings, an energy audit is the way to go. The auditor will pinpoint areas of your home that use the most energy and offer solutions to lower your energy use and costs. Trained energy auditors know what to look for and can locate a variety of flaws that may be resulting in energy inefficiency, including inadequate insula tion, construction flaws, and uneven heat distribution. When it’s time to replace old appliances, it’s wise to spend a bit more for an energy-efficient model, and be sure that you are taking advantage of energy-saving settings already on your current refrig erator, dishwasher, washing machine, or dryer. Caulk old windows that might be leaky to prevent drafts, and choose double-paned windows if you’re building an addition or replacing old windows. Most areas of your home or apartment offer opportunities to save energy and money. You can reduce your $130 monthly lighting costs to $65 by using fluorescent bulbs instead of incandescent. If you’re interested in starting a book club, you should consider the following options and recommendations. Before recruiting, think carefully about how many people you want to participate and also what the club’s focus will be. Some are even more specific, focusing only on a particular genre such as mysteries, science fiction, or romance. All of these possibilities can make for a great club, but it is important to decide on a focus at the outset so the guidelines will be clear to the group and prospective member. Notify friends and family, advertise in the local newspaper, and hang flyers on bulletin boards in local stores, colleges, libraries, and bookstores. When enough people express interest, schedule a kick-off meeting during which decisions will be made about specific guidelines that will ensure the club runs smoothly. This meeting will need to estab lish where the group will meet (rotating homes or a public venue such as a library or coffee shop); how often the group will meet, and on what day of the week and at what time; how long the meetings will be; how books will be chosen and by whom; who will lead the group (if anyone); and whether refreshments will be served and if so, who will supply them. By the end of this meeting, these guidelines should be set and a book selection and date for the first official meet ing should be finalized. Planning and running a book club is not without challenges, but when a book club is run effectively, the experience can be extremely rewarding for everyone involved. Which of the following organizational patterns is the main one used in the passage? According to the passage, when starting a book club, the first thing a person should do is a. The strike resulted in huge financial losses for the company and the threat of a national boycott on Hartville products. The situation resulted in the formation of an employee task force, supported by Hartville management, to review circumstances that led to the strike. The task-force findings follow: N Hartville’s overtime pay schedule is well below the national level, and overtime is mandatory at least once a week. N Employees working in the manufacturing department have an alarmingly high rate of repetitive stress injury. The equipment they are working with is extremely old and dangerous and does not meet current health and safety standards. The task force recommended that equipment be evaluated and brought up-to date immediately. Employees report conflicting and/or confusing policies relating to sick and personal days, which have resulted in numerous misunder standings about procedures and allowances as well as unfair disciplinary action. N In the past four years, five pregnant women with clean work records were terminated soon after their pregnancies were public.
Generic 300mg lopid with amex
Diabetic foot to thermal or mechanical trauma treatment kidney infection discount lopid american express, and to the Ultrasound: Doppler ultrasound to see the blood flow late detection of infection processes or tissue breakdown. The Effects on foot morphology (deformities): due to most of test is not painful and involves the technician moving a the above alterations, a significant imbalance of peripheral non-invasive probe over the blood vessels of the lower musculature and soft tissue does have place in the foot extremities. These specialists are skilled in Diabetic foot are represented by a high longitudinal arch dealing with diabetic lower extremity infections, bone (rigid cavus foot), hammer toes and hallux valgus. With an angiogram, a catheter is There are certain general as well as confirmatory tests for inserted through the artery in the groin and dye is injected Diabetic foot ulcer just like any other disease. This procedure studies of circulation in the legs, and consultation with is usually performed with local anaesthesia and a light specialists. For a lower extremity wound or ulcer, this may involve probing the wound with a blunt probe to determine its depth. Minor surgical debridement of the wound (cleaning or cutting away of tissue) may be necessary to determine the seriousness of the wound. Infection (as above) in a patient who is systemically well and Moderate 3 metabolically stable but which has >1 of the following characteristics: cellulitis extending >2 cm, lymphangitic streaking, spread beneath the superficial fascia, deep-tissue abscess, gangrene, and involvement of muscle, tendon, joint or bone Infection in a patient with systemic toxicity or metabolic Severe 4 instability. In addition, they must understand that chronic osteomyelitis cannot be cured with antibiotics Treatment of foot ulcer involves close monitoring of alone and that adequate surgical debridement is necessary. The oxygen levels in the skin of patients with peripheral vascular Patients who are unwilling to undergo the surgical disease, for example, are closely observed. Diabetics are procedure must understand the long-term complications of urged to quickly consult a physician at the first sign of chronic osteomyelitis. Patients with foot ulcer may also infection is not adequately treated with sufficient surgical be required to quit smoking (if they are smokers) and debridement and/or amputation, systemic complications, change lifestyle habits that contribute to the condition. Patients are also advised to switch to of septic complications, but it does not affect the long-term cushioned shoes or other prescription footwear. Healthcare professionals usually extend systemic (metabolic) issues and coordinated management, self-care training to such patients. They are taught how to preferably by a multidisciplinary foot-care team the team prevent and manage foot ulcer, monitor their blood sugar managing these infections should include, or have ready levels, inspect their feet at a regular basis, and also control. Patients with diabetes must be careful to avoid foot trauma and to properly care for their feet to minimize the 368 Journal of Scientific and Innovative Research Figure 1: Depicts approach treating a patient with foot ulcer Figure 2: Depicts considering hospitalization 369 Journal of Scientific and Innovative Research Figure 3: Depicts diabetic patient with a foot infection who is not responding well to treatment Conclusion 6. Causal pathways for incident lower extremity ulcers in patients with diabetes from two settings. The North-West Diabetes Foot Care Study: incidence of, and risk factors for, new diabetic foot ulceration in a community-based patient cohort. The effectiveness of footwear and offloading interventions to prevent and heal foot ulcers and reduce plantar pressure in diabetes: a systematic review. The carcinogenicity assessment provides information on the carcinogenic hazard potential of the substance in question and quantitative estimates of risk from oral and inhalation exposure may be derived. The information includes a weight-of-evidence judgment of the likelihood that the agent is a human carcinogen and the conditions under which the carcinogenic effects may be expressed. Quantitative risk estimates may be derived from the application of a low-dose extrapolation procedure. If derived, the oral slope factor is a plausible upper bound on the estimate of risk per mg/kg-day of oral exposure. Similarly, an inhalation unit risk is a 3 plausible upper bound on the estimate of risk per μg/m air breathed. Primary, peer-literature identified through September 2011 was included where that literature was determined to be critical to the assessment. Other peer reviewed information, including health assessments developed by other organizations, review articles, and independent analyses of the health effects data were retrieved and may be included in the assessment where appropriate. It should be noted that references have been added to the Toxicological Review after the external peer review in response to peer reviewers’ comments and for the sake of completeness. These references have not changed the overall qualitative and quantitative conclusions. Selected chemical and physical properties of dichloromethane are listed in Table 2-1. Coast Guard (1999) Auto ignition temperature 640°C Holbrook (2003) 5 Latent heat of vaporization 3. The older method involves the direct reaction of methane with chlorine either at high temperatures or at lower temperatures under catalytic or photolytic conditions (Holbrook, 2003). The more 1 “Dichloromethane” is used throughout this summary even if a specific paper used the term “methylene chloride. Excess methyl chloride is then reacted in the gas phase thermally with chlorine to produce dichloromethane (Holbrook, 2003). Dichloromethane has been used in paint strippers and removers, as a propellant in aerosols, in the manufacture of drugs, pharmaceuticals, film coatings, electronics, and polyurethane foam, and as a metal-cleaning solvent. Dichloromethane production rose sharply in the decades following the war due to the increased demand for this substance for use mainly in paint strippers (Hardie, 1964; Searles and McPhail, 1949). As other solvent uses and its use in aerosol propellants became important, demand for this substance increased further (Anthony, 1979). Some of the dichloromethane released to soil or water is expected to volatilize to air. In soil, dichloromethane is expected to be highly mobile and may migrate to groundwater. The potential for dichloromethane to bioconcentrate in aquatic or marine organisms is low. Dichloromethane may biodegrade in soil or water under both aerobic and anaerobic conditions. Oral—Gastrointestinal Tract Absorption There are currently no data available on absorption of dichloromethane following oral intake in humans. However, after oral administration in animals, dichloromethane is rapidly and nearly completely absorbed in the gastrointestinal tract (Angelo et al. At several time points within 40 minutes of dose administration, <2% of the dose was found in the lower part of the gastrointestinal tract, indicating that the majority of dichloromethane absorption occurs in the upper gastrointestinal tract (Angelo et al. Similar results were reported in mature male B6C3F1 mice exposed to up to 50 mg/kg (Angelo et al. In mature male Sprague Dawley rats administered a single dose (1 or 50 mg/kg) of radiolabeled dichloromethane, <1% of the label was found in feces collected for 48 hours after dose administration (McKenna and Zempel, 1981). Absorption of dichloromethane generally follows first-order kinetics (Angelo et al. The vehicle appears to affect the rate but not the extent of gastrointestinal absorption, with an aqueous vehicle resulting in a more rapid absorption of dichloromethane than an oil-based vehicle (Angelo et al. Inhalation—Respiratory Tract Absorption Several studies in humans have demonstrated absorption of dichloromethane following inhalation exposure. There was a pause of about 20 minutes without exposure between rest and exercise periods. Uptake of dichloromethane was estimated at about 55% 2 while resting and about 40, 30, and 35% at respective workloads of 50, 100, and 150 watts. Blood levels of dichloromethane correlated directly with exposure concentrations, and did not appear to increase when a workload was applied (Astrand et al. Similar reports of rapid uptake and a direct correlation between dichloromethane exposure level and blood levels in humans have been presented by other groups (DiVincenzo and Kaplan, 1981; DiVincenzo et al. A later study by the same group (DiVincenzo and Kaplan, 1981) similarly reported a rapid absorption of dichloromethane in volunteers exposed to 50–200 ppm for 7. A steady-state level, as assessed by levels of unchanged dichloromethane in the expired air, was reached quickly (1–2 hours), with exhaled dichloromethane levels increasing with increasing exposure level. Estimated pulmonary uptake was 69–75% and did not vary appreciably with exposure concentration. In another experiment in which one of the investigators was seated during exposure to 100 ppm dichloromethane for 2 hours, concentrations of dichloromethane in expired air reached an apparent plateau of about 70 ppm within the first hour of exposure (Riley et al. Body fat may influence absorption of dichloromethane, as evidenced by data from an experiment involving 12 men, ages 21–35, divided into two groups (n = 6 per group) based on percent body fat (Engström and Bjurström, 1977). Total uptake of dichloromethane during a light exercise period (50 watts) for 1 hour with an exposure level of 750 ppm was positively correlated with percent body fat (r = 0. Initially, dichloromethane is readily absorbed following inhalation exposure, as evidenced by rapid appearance of dichloromethane in blood, tissues, and expired air (Withey and Karpinski, 1985; Stott and McKenna, 1984; Anders and Sunram, 1982; Carlsson and Hultengren, 1975; Roth et al. For example, absorption of inhaled 500 ppm dichloromethane in anesthetized, mature male F344 rats reached an apparent plateau within 10–20 minutes and was relatively constant for up to 2 hours (Stott and McKenna, 1984). In these experiments, absorption was calculated from measurements of exposure (nose only) and effluent concentrations and ventilation flow rate in intact animals; double tracheostomized rats were used to measure absorption in the isolated upper respiratory tract and the lower respiratory tract. Twenty minutes after a single intravenous dose of 10 mg [ C]-dichloromethane/kg to mature male B6C3F1 mice (Angelo et al.
Woody Climber (American Ivy). Lopid.
- Are there safety concerns?
- What is American Ivy?
- Digestive disorders, stimulating sweating, reducing swelling (astringent), and as a tonic.
- Dosing considerations for American Ivy.
- How does American Ivy work?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96300

Cheap 300 mg lopid with amex
Since then symptoms 8 days before period purchase cheapest lopid and lopid, Orange County has made tremendous strides, by steadily improving the rate of people with diabetes who have had less than two A1C tests annually. Orange County, again, has consistently shown 11 better guideline compliance than the state. There has been concern about the number of residents who self-monitor their blood glucose as recommended. Recommendations vary, based on medication use, mealtimes, and overall blood sugar control; but the rates of those who check it at least once a day have increased from 81. Though this rate has not changed significantly, it is above the state rates of 12 83. Over the past five years there have been slight, but significant, changes in disparities among 13 different groups in Orange County with regard to the diabetes rate (see Table below). Females, those older than 45, and those with incomes below $50,000 per year, are all more likely to be told that they have diabetes than was the case in 2009, but this is a trend that has not remained consistent over the years. In 2007, residents with incomes above $50,000 per year had similar rates of diagnosed diabetes as those with lower incomes; and in 2008, males were marginally more likely than females to have been diagnosed with diabetes. Primary Data: Residents’ Concerns Quantitative: Survey Diabetes was not specifically asked about on the Community Health Opinion Survey. Current Initiatives and Activities There are several initiatives in the county focused on diabetes prevention and management. The program also targets those who have historically lacked access to such care including minority populations, the under/uninsured, those living in rural areas, and those lacking transportation to classes, and provides linguistically accessible services to those who participate. The Health Department leads the county’s diabetes task force, which is a group of medical professionals and community groups addressing the burden of diabetes in Orange County. The 113 2011 Orange County Community Health Assessment Orange County Department on Aging offers chronic disease management classes including diabetes education, and works in partnership with the health department. Interpretations: Disparities; Emerging Issues; Gaps and Unmet Needs; and Strategies In regards to diabetes, more education is needed to help the community understand how to prevent diabetes and how to best manage diabetes once diagnosed. Particularly in the northern portion of the county where many low-income elderly people reside, more outreach could be done to educate and help them combat the complications of diabetes. The Orange County Diabetes Task Force identified a need for more Registered Dietitians, and diabetes classes/programs in the community. It was noted that many of these outreach educational efforts need to be provided in languages other than English due to the growing immigrant and refugee population in Orange County. There is also a recognized benefit from encouraging industries/companies to offer worksite health and wellness programs to promote healthy behaviors that prevent obesity and chronic disease. Access to primary care for low income residents continues to be a concern and is needed in order for them to receive the proper screening necessary to determine if they have diabetes and how to access the needed treatment, particularly medications and blood glucose testing supplies to prevent complications. To save medical costs, insurance companies should be encouraged to cover or expand coverage for Medical Nutrition Therapy and Diabetes Self-Management Education. The number of children and adults who are overweight or obese is rapidly increasing and as a result, the number of people who have diabetes, especially children, is increasing at an alarming rate. Increasing the opportunities for safe play and exercise for both children and adults and improving the nutritional content of restaurant/fast food choices will help to ward off the potential for early onset of diabetes. It will be important that these health education messages and services be linguistically and culturally tailored, to meet the needs of all of the residents of Orange County. According to the American Heart Association, it has been estimated that “if all forms of cardiovascular disease were eliminated, the nationwide life expectancy would rise by nearly seven 1 2 years. It is estimated that each person who dies from a stroke has had their life shortened by an average of 4. Many people survive strokes but are left with disabilities requiring lengthy terms of rehabilitation to regain strength, mobility, and cognitive and verbal skills. The true cost of heart disease and stroke is greater than just dollars and cents, it also encompasses the human and societal costs brought on by lost productivity, disability and premature death. Factors, that cannot be controlled, that increase the chances of experiencing heart disease or stroke include family history, age, or gender. These include elevated blood cholesterol, high blood pressure, family, diabetes, tobacco 5 use and exposure to second hand smoke, overweight and obesity, physical inactivity, a diet high in 6 fat and sodium, and certain types of dental disease. In addition to the primary risk factors listed above, secondary factors that can contribute to heart and cerebrovascular disease include stress, 7 low socio-economic status, isolation, depression, and discrimination. Cerebrovascular disease (often resulting in a stroke) is the third leading cause of death in both the 9 state and the county. North Carolina is also part of a band of Southeastern States that have the highest rates of stroke in the nation. Not only are both heart disease and stroke prevalent, but they are also very costly. In 2009, heart disease and cerebrovascular disease were Orange County’s leading causes of hospitalizations and hospital expenses, at $31,730,269 for heart disease and $7,290,187 for cerebrovascular disease. The average length of hospital stay for heart disease and cerebrovascular disease was 4. The total direct hospital charges for heart disease in North Carolina are estimated 13 to be nearly $3. These figures do not take into account the total costs of these diseases to the individual, families, and society. Though heart disease is the second leading cause of death in Orange County, there have been some encouraging trends. Between the years 2001 and 2005 the age-adjusted death rate for heart disease 14 15 in Orange County was 165. With this current rate, the County has already surpassed the Healthy Carolinians 2020 heart disease target of 161. Like heart disease, Orange County’s age-adjusted death rate for cerebrovascular disease is better than 17 the state’s, with a county rate of 39. Primary Data: Residents’ Concerns Quantitative: Survey Heart disease and stroke were not included on the Community Health Opinion Survey. Qualitative: Focus Groups Heart disease and stroke were not discussed during the focus group discussions. The mission is to help “people achieve optimal health in a safe and supportive environment by integrating professional resources, innovative programs and personalized service. The Cardiac Rehab program is a twelve-week outpatient program for individuals recovering from cardiac events or surgery. The program components include exercise, nutrition, medication management, stress management and psycho-social support. The Bridge is for individuals who do not need cardiac rehab, but would benefit from professional guidance in learning to exercise safely. Exercise sessions are supervised by nurses and exercise physiologists and health education is tailored for the participant’s needs. Interpretations: Disparities; Emerging Issues; Gaps and Unmet Needs; and Strategies Despite these seemingly positive statistics, a closer examination of the data shows that some segments of the population are not doing as well as others. There is a disparity in the heart disease and cerebrovascular disease death rates for whites and African Americans in Orange County. The disparity in heart disease death rates is even greater for females, with the rate for African American women being 1. If people are unaware of their cholesterol levels, they are unlikely to take steps to control their cholesterol. Even if they do make efforts to lower their risks of high cholesterol, without measuring cholesterol levels they have no way of knowing if the steps they are taking are working. The causes of the disparity in health status between whites and other racial and ethnic groups, particularly African Americans, are multiple, ranging from family history to the effects of poverty, racism, and behaviors. Of all the risk factors, those most easily controlled are health behaviors such as smoking, diet, and exercise. The Table below shows the differences in the percentages of African American and white adults that engage in some health behaviors that may account for some of the health disparities in heart disease and strokes noted in North Carolina. Table 34: Percentages of North Carolina Adults with Selected Risk Factors/Conditions, by,21 Race/Ethnicity African American White Current smoking (2006–2008) 22. More and more Americans are becoming overweight or obese as a result of calorie-laden diets and lack of physical activity.
Lopid 300mg cheap
Other than direct penetration with Mucorales medicine 7 purchase lopid 300mg on line, the most common mode of transmission is through inhalation of fungal spores that can result in sinus, orbital, rhino, central nervous system, or pulmonary infections. Di abetics carry a particularly high risk of developing this infection, because when the dis ease is uncontrolled, this results in impairment of neutrophil function, phagocytosis, and oxidative reactions as well as increases free iron, which acts as a substrate, which enhances mucormycosis growth. Primary penetration of fungal spores through breach of the skin barrier is the most common cause of cutaneous mucormycosis. The presentation of oral and maxillofacial involvement including the face, nose, or palate is seen in 50% of cases but has been noted to be early diagnostic signs. Necrotic eschar of the palate as a result of extension of mucormycosis rhinosinusitis. If left untreated, extension into the orbit can lead to orbital cellulitis, corneal anesthesia, facial anhidrosis, proptosis, diplopia, loss of vision, ophthalmople gia, or trigeminal/facial/orbital/optic nerve involvement. In a study by Chamilos and colleagues,44 if initial Amphotericin B treatment is delayed, it is associated with signif icant increase in overall mortalities. As an alternative to Amphotericin B, posaconazole (an antifungal triazole) has shown a clinical efficacy in the treatment of refractory cases initially treated with Amphotericin B (known as salvage therapy). The therapy provides reduction in tissue hypoxia and acidosis and provides high oxygen concentrations that are considered fungistatic, resulting in wound healing while enhancing neutrophilic action. The spore form is found most commonly in moist, warm soil areas in the central and eastern United States, especially around the Mississippi and the Ohio River Valley and particularly in areas of exposure to ex cretions of bats and birds. Diagnosis A new blood culture test is now available that uses a lysis-centrifugation blood culture technique that can rapidly detect organisms in patients with disseminated histoplas mosis. Biopsy and culture of tissue from biopsy, body fluids, and secretions are also used. Oral Manifestations Oral manifestations of a histoplasma infection can present in all types of histoplasmo sis (acute, chronic, and disseminated), but with variable occurrence. In one review of 78 patients with histoplasmosis, oral manifestations were found in 19% of acute cases, 31% of subacute cases, and 66% in disseminated cases. These lesions can often appear similar in appearance to squamous cell carcinomas with a firm base, necrotic center, and rolled borders. Primary localized histoplasmosis: oral manifes tations in immunocompetent patients. Itraconazole is a commonly used antifungal agent and may be needed for 3 to 12 months. The endemic areas for Blastomyces in the United States include the Midwest ern, south-central, and southeastern states with the highest concentration in the Ohio and Mississippi River valleys, the Great Lakes, and Saint Lawrence River. This rare fungal infection has a yearly incident rate of 1 to 2 cases per 100,000 in the United States. Most oral lesions are ulcerative, but there may be verrucous lesions, granulomas, sessile-based projections, abscess in the mandible with radiographic bone loss, and mobile teeth. More than 50 species of Crypto coccus have been identified, but only 2 species are known to cause human disease, namely, Cryptococcus neoformans and Cryptococcus gattii. Oral Cryptococcosis can manifest as superficial ulcers, violaceous nodules, granu loma, cancerous looking lesions, or draining sinuses (Fig. Diagnosis of Cryptococcosis depends on isolation of the organism in culture from the involved site, including skin and oral lesions, blood, cerebrospinal fluid, and bron choalveolar lavage. Treatment Management of Cryptococcosis depends on the site of involvement and the immune status of the patient. It is considered the second most common opportunistic fungal infection after the Candida species. Crypto coccal tongue lesion in a stem cell transplant patient: first reported case. The most common portal of entry is by inhalation of fungal spores into the sinuses and the respiratory tract. Once inhaled, in the absence of appropriate host defenses, the spores enlarge, germinate, and dissemi nate hematogenously by vascular invasion. Defects in ciliary clearance in the airways, compromised innate and adaptive defense against Aspergillus, predispose an individual to develop disease. In the oral and maxillary region, rhinosinusitis is the most common manifestation, either invasive, destructive invasive, or allergic form. Spores occasionally get introduced to the antrum via an oroantral communica tion during a dental procedure, such as a root canal perforation or a dental extraction, and become pathogenic. Invasive fungal sinusitis can have an acute and fulminant course with a 342 Telles et al high mortality occurring predominantly in the immunocompromised patient,68 or a chronic indolent, granulomatous form with progression through the sinus mucosa, un derlying bone and tissue. Clinically, Aspergillus rhinosinusitis can present with head ache, fever, nasal congestion, facial swelling, purulent or bloody nasal discharge. It should be suspected in a patient with recurrent or refractory sinusitis not responding to antibiotic therapy. Oral lesions associated with Aspergillosis and other systemic mycoses usually occur as a part of a disseminated disease from the lungs, but occasionally can reflect extension from a contiguous structure such as the maxillary sinus or a primary infec tion of the oral mucosa. Necrotic ulcers are one of the most frequently encountered lesions, as shown in Figs. In the advanced stage, these lesions transform into gray necrotic lesions extending into the attached gingiva with ulceration and pseudomembrane. In the late stage, progressive destruction of alveolar bone and surrounding facial muscles is noted, with histopathologic evidence of infil tration of fungal hyphae into the tissues. The presence of deep perioral ulceration in an immunocompromised patient should raise suspicion for fungal infection, including Aspergillosis. Orofacial osteomyelitis, including of the paranasal sinuses, jaw, and skull base, has been reported. Gabrielli and colleagues71 reviewed 310 cases of osteomyelitis caused by Aspergillus species and found 18% of the cases involved the maxillofacial area. Diagnosis of aspergillosis requires a histopathologic examination and culture of affected tissue and fluid. Angioinvasion is characteristic of Aspergillus along with tis sue and bone necrosis. Diffuse edematous swelling of the palatal mucosa (bottom arrows) with focal ulcer ation (top arrow). In Southern California, as much as 75% of the population is found to have immunity to the organism. Cutaneous involvement is the most frequent extrapulmonary mani festation, especially of the face and the extremities. Serum antibodies immunoglobulin M (IgM) and IgG are the most frequently used diagnostic tests. IgM can be detected early in the disease (1–3 weeks), whereas IgG levels are raised after 8 to 10 weeks of symptom presentation. However, appropriate follow-up every 3 to 6 months should be performed in these patients until radiographic resolution is achieved. However, many suggest 344 Telles et al that it may be underdiagnosed or misdiagnosed due to its close resemblance to dis eases cause by Candida sp, particularly of the oral cavity. G can didum is considered a resident flora in humans and has been isolated from multiple sources, including the mouth, respiratory tract, gastrointestinal tract, skin, and vagina. Bonifaz and colleagues84 re ported a total of 12 cases of oral geotrichosis and found 3 clinical varieties, with pseu domembranous being the most common type (75%), followed by hyperplastic and palatine ulcer. Pseudomembranous geotrichosis appears as white plaques on an erythematous background, which can be easily scraped off, and can be mistaken for candidiasis very easily. It mainly involves the tongue (glossitis) along with the buccal mucosa, soft palate, and rarely, the pharynx. Because treatment for oral geotrichosis is similar to treatment of candidiasis (ie, re sponds to typical anti-candidal drugs), it is thought that many cases are misdiag nosed. The villous manifestations of geotrichosis comparably resemble candidiasis as well as some viral infections. On the other hand, palatine ulcers are deeper and appear similar to other mold infections, such as mucormycosis or aspergillosis, which can be very aggressive with cerebral extension and carry a poor prognosis. The hyphae may, however, be confused easily with pseu dohyphae and blastoconidia of Candida. Molecular biology is the most accurate technique and can identify different species.

Order lopid in united states online
Medical and Prescription Drug the out-of-pocket limit is the most you could pay in a plan year for covered services medications during pregnancy chart purchase 300mg lopid amex. Out-of-Network: $13,100 individual/ out-of-pocket limit, depending upon plan coverage. Be aware, your network provider might use an out-of-network provider for some services (such as lab work). Deductible, then $120 copay For non-routine obstetrical care or Office visits No Charge per visit complications of pregnancy, cost sharing may apply. Your Rights to Continue Coverage: There are agencies that can help if you want to continue your coverage after it ends. The contact information for those agencies is: Department of Labor Employee Benefits Security Administration. Other coverage options may be available to you too, including buying individual insurance coverage through the Health Insurance Marketplace. For more information about your rights, look at the explanation of benefits you will receive for that medical claim. Your plan documents also provide complete information to submit a claim, appeal, or a grievance for any reason to your plan. For more information about your rights, this notice, or assistance, contact: Department of Labor Employee Benefits Security Administration. Yes If you don’t have Minimum Essential Coverage for a month, you’ll have to make a payment when you file your tax return unless you qualify for an exemption from the requirement that you have health coverage for that month. Yes If your plan doesn’t meet the Minimum Value Standards, you may be eligible for a premium tax credit to help you pay for a plan through the Marketplace. Your actual costs will be different depending on the actual care you receive, the prices your providers charge, and many other factors. Focus on the cost sharing amounts (deductibles, copayments and coinsurance) and excluded services under the plan. Use this information to compare the portion of costs you might pay under different health plans. Our friendly, local customer tobacco users quit for good ° Popular local and national family of people in need, so we service representatives answer attractions, such as zoos and. Award-winning care managers who invest in programs to create your calls quickly and effciently amusement parks provide education and support for chronic healthier communities. Alternative care options Experience and innovation mean Tools to maintain and improve health You can see a naturopath or other alternative care better care for you. You get more for your health With myProvidence, our secure member portal provider for covered benefts, including periodic exams and your health care dollar. You’ll receive discounts on and benefts information, you can: same rate as they would be for a primary care provider, of the nation’s top massage therapy, ftness as long as the alternative care provider is licensed to . Get a baseline of your overall health 10 most integrated classes, gym memberships, perform the services. For more information about plan benefts and enrollment requirements, limitations and exclusions, see the plan contract or contact our sales team or your insurance producer. Providence plans are also available through the Federal Health Insurance Marketplace at HealthCare. Please note that the selling area for each plan may be different from the provider network. Plans available from Plans available directly the Federal Health Plan name and metal tier from Providence or Insurance Marketplace Standard plans Connect plans your producer at HealthCare. Signature Network Available in these counties: Clackamas, Hood River, Multnomah, Choice Network Washington, Yamhill (zip code 97132 only) We can help you fnd the right plan for you. Signature Network: Baker, Columbia, Coos, Curry, Gilliam, Grant, Harney, Josephine, Klamath, – Portland metro area 503-574-5000 Lake, Malheur, Morrow, Sherman, Tillamook, – All other areas 800-988-0088 Umatilla, Union, Wallowa, Wasco, Wheeler. With your insurance producer Choice Network: Benton, Clackamas, Clatsop, Apply during open enrollment from Nov. After the open enrollment period ends, Crook, Deschutes, Douglas, Hood River, you must have a qualifying life event to enroll in a health insurance plan. Qualifying life events include losing employer Jackson, Jefferson, Lane, Lincoln, Linn, Marion, coverage, marriage and the birth of a child. Multnomah, Polk, Washington, Yamhill Providence Progressive Dental plan: All counties in Oregon 4 5 Connect (continued) Connect Connect 2500 Silver Connect 7350 Bronze Connect plans combine a medical home model of care with a tailored provider network. The medical home In-network In-network No Out-of-network benefits No Out-of-network benefits model provides a team of health professionals that supports all aspects of your overall Offce Visits for Medical Services well-being, from wellness and prevention to helping you manage chronic conditions. Primary Care Provider $25✓ $50✓ Express Care Virtual, Express Care Clinics or Connect plans offer: Providence Connect Network: A network of more $0✓ $0✓ Web-direct visits than 70 primary care clinics in Clackamas, Hood. More than 70 medical home clinics Alternative care provider $25✓ $50✓ River, Multnomah, Washington and Yamhill (Zip code in the Portland metro area Specialist $50✓ $0 97132 only) counties designated as medical homes. You must Inpatient hospital services and maternity care 30% 0% use an in-network provider to Emergency receive benefts Emergency services $250 then 30% 0% (All emergency services are treated as in-network). Access to specialists via referral from Hood River Urgent Care the medical home Wash. Pediatric dental coverage and optional To see if your provider is in one of our medical homes, Outpatient surgery at an ambulatory surgery family dental coverage 30% 0% select "Medical Home Primary Care Providers" under center or hospital-based facility. Chiropractic manipulation and acupuncture $25✓ $25✓ acupuncture are covered in-network (limited to three visits combined per calendar year) Prescription Drugs Connect Preferred generic $20✓ $30✓ Non-preferred generic $35✓ $60✓ Preferred brand name $75✓ $0 Connect 2500 Silver Connect 7350 Bronze Non-preferred brand name 50% 0% In-network In-network Specialty 50% 0% No Out-of-network benefits No Out-of-network benefits Pediatric Vision Services (children aged 18 years and younger) Annual deductible Routine eye exams (one exam/calendar year) Covered in full✓ Covered in full✓ $2,500/$5,000 $7,350/$14,700 Individual/Family Vision hardware (frames, lenses, contact lenses); Covered in full✓ Covered in full✓ Annual out-of-pocket maximum limits apply $7,350/$14,700 $7,350/$14,700 Individual/Family Adult Vision Services After meeting your deductible, you pay the following amounts for covered services. Routine eye exams (one exam/calendar year) $25✓ $25✓ the deductible does not apply for some covered services. These are marked with ✓ Vision hardware Preventive Care Not covered Not covered (frames, lenses, contact lenses); limits apply Periodic health exams and well-baby care (from Pediatric Dental Services* (children aged 18 years and younger) Covered in full✓ Covered in full✓ any provider licensed to perform the service) Preventive services (includes routine exams, Maternity prenatal care Covered in full✓ Covered in full✓ Covered in full✓ Covered in full✓ cleanings, X-rays, topical fluoride) Gynecological exams (one per calendar year); Basic services (restorative fillings) 50% 0% Covered in full✓ Covered in full✓ Pap tests Major services (includes oral surgery, crowns, Mammograms Covered in full✓ Covered in full✓ periodontics, endodontics, denture and bridge 50% 0% 6 Colorectal cancer screenings (preventive, age 50 work) 7 Covered in full✓ Covered in full✓ and over) ✓ Deductible is waived for these services * Dental services subject to medical deductible and out-of-pocket maximum Note: In order to access the in-network cost shares, you must work through your medical home. No out of network benefits Offce Visits for Medical Services Standard plans offer: Providence Signature Network: A network of Primary Care Provider $20✓ $40✓ $0 nearly 1 million health care providers nationwide. Copays starting as low as $10 and Express Care Virtual, Express Care Clinics or both in Providence facilities and in other locations $0✓ $0✓ $0 deductibles as low as $1,000 Web-direct visits Providence Choice Network: A network of over. No out-of-network benefts are included 230 primary care clinics designated as medical homes Alternative care provider $40✓ $80✓ $0 with this plan. You must use an in Specialist $40✓ $80✓ $0 network provider to receive benefts Clatsop Columbia Hospital Services Hood River. Inpatient hospital services and maternity care 20% 30% 0% will be the Providence Choice Network. In Morrow Yamhill Clackamas Union Emergency other counties, your provider network is Wasco Polk Marion Emergency services the Providence Signature Network Baker 20% 30% 0% Linn Jefferson Grant (All emergency services are treated as in-network. Access to specialists via referral from the Crook Urgent Care medical home for Standard plans on the Lane Deschutes Urgent care services $60✓ $70✓ $0 Choice network. Chiropractic manipulation and acupuncture Not covered Not covered Not covered Note: Standard plans do not cover chiropractic manipulation, acupuncture, adult routine vision exams and vision Prescription Drugs hardware, or pediatric dental services. Generic $10✓ $15✓ $0 Preferred brand name $30✓ $60✓ 0% Standard Non-preferred brand name 50%✓ 50%✓ 0% Providence Oregon Providence Oregon Providence Oregon Specialty 50%✓ 50%✓ 0% Standard Gold Standard Silver Standard Bronze** Pediatric Vision Services (children aged 18 years and younger) In-network Routine eye exams (one exam/calendar year) Covered in full✓ Covered in full✓ Covered in full✓ No out of network benefits Vision hardware Covered in full✓ Covered in full✓ Covered in full✓ Annual deductible (frames, lenses, contact lenses); Limits apply $1,000/ $2,000 $2,500/ $5,000 $6,550/$13,100 Individual/family Adult Vision Services Annual out-of-pocket maximum Routine eye exams (one exam/calendar year) Not covered Not covered Not covered $6,850/ $13,700 $7,350/$14,700 $6,550/$13,100 Individual/family Vision hardware (frames, lenses, contact lenses); After meeting your deductible, you pay the following amounts for covered services. The deductible does not apply Not covered Not covered Not covered limits apply for some covered services. Basic and major services, including extractions, crowns and dentures, are also covered. Through this guide can help you decide which the plan, you have access to more than 2,300 in-network dental provider listings in type to use in each situation. Oregon and southwest Washington and more than 270,000 in-network provider listings nationwide. In-network diagnostic and preventive care services, reducing your costs in subsequent years of service. There is no out-of-network coverage, so you must * * services, including root canals, crowns, bridges (free) Virtual (free) Clinics (free) use an in-network provider to receive benefts. These are marked with ✓ In-network Primary Care ($$) Urgent Care ($$$) Emergency ($$$$$) Year 1 Year 2 Year 3 Diagnostic and preventive services (includes routine exams, X-rays, cleanings, Covered in Covered in Covered in Want to see someone who knows Know you need help right away, but Think your life may be in danger? Urgent care can deal with attack, stroke, uncontrolled Basic services (includes restorative fillings) 50% 40% 20% preventive care or follow-up? Major services (includes oral surgery, crowns, endodontics, periodontics, See your primary care provider. You may near you not purchase our dental plan if you get your Providence medical plan through the Marketplace.
Buy online lopid
In contrast medicine 44334 purchase generic lopid from india, another study [22] found pacifier suction as the most common habit in the investigated population (65. This fact, however, is probably explained by the age of the children in the sample, who were between 3 and 5 years old, constituting a smaller age group. The literature consulted also suggested the connection between malocclusion and postural alterations, especially between head and neck [22, 23] but it is necessary to explore and measure these variables more accurately, especially in the age groups characterized by periods of transitions and changes in the craniofacial complex. Neural connections exist between the cervical and trigeminal sensorimotor systems, showing that strong neuromusculoskeletal and neurophysiological connections are involved in the interrelationship between the orofacial and cervical regions. This reinforces the existence of simultaneous and coordinated activity between the neck and jaw muscles, however, this relationship has not yet been investigated in a more systematized manner [23]. In this way, the knowledge of these factors and their detection by the dental surgeon is of immense importance for an early and effective intervention, in order to prevent the future consequences that these habits can bring, both aesthetic and functional and/or psychological [24, 25]. It also indicates the need for broader investigations, with similar methodologies to facilitate the comparison of results, in order to elucidate the gaps still present in the relationship between deleterious oral habits and postural changes clinically relevant to clinical practice. Is there a relation between harmful oral habits and facial typology and dental occlusion? The relationship of bottle feeding and other sucking behaviors with speech disorder in Patagonian preschoolers. Body posture and the stomatognathic functions in mouth breathing children: a literature review. Obstructive sleep apnea prevents the expected difference in craniofacial growth of boys and girls. Deficits in working memory, Reading comprehension and arithmetic skills in children with mouth breathing syndrome: analytical cross-sectional study. Coordination of the stomatognathic and postural systeactivities and their functional status. Muscular, functional and orthodontic changes in preschool children with enlarged adenoids and tonsils. Characteristics of the occlusion and prevalence of malocclusion in children treated at the Federal University of Goiás. The influence of using digital diagnostic information on orthodontic treatment planning a pilot study. Orientation and position of head posture, scapula and thoracic spine in mouth-breathing children. An overview of the prevalence of malocclusion in 6 to 10-year-old children in Brazil. Malocclusion, breast feedint and deleterious buccal habits in preschool children an association study. Spine deviations and orthodontic treatment of asymmetric malocclusions in children. Siclauskiene M, Smailiene D, Lopatiene K, Cekanauskas E, Pribuisiene R, Sidlauskas M. Relationships between malocclusion, body posture, and nasopharyngeal pathology in pre orthodontic children. Estudo das relações entre mastigação e postura de cabeça e pescoço revisão sistemática. Effects of unilateral mastication on the stomatognathic system and possible predisposing factors in schoolchildren from Medellin. The macro-esthetics (face), mini-esthetics (smile), and micro-esthetics (dental component) coordinate to offer a complete approach to esthetic treatment planning. The chapter presents a broad vision of aesthetic treatment designed to take readers to another stage of smile designing with dental implants that can increase patient results and outcomes. It is a challenging task that requires putting together anatomical, biochemical, biologic, gnathologic and esthetic knowledge in to a plan of treatment to provide the patients a satisfying and functional and long-term outcome [1]. It is essential to offer a lifelong guarantee for dental surgical work and long-term guarantee for prosthetic restoration, which exhibits the tendency of “material fatigue”. In everyday practice, as well as in teaching, there must be reliable clinical workflow and it Karpiński T. The challenge lies in being able to incorporate procedures and techniques in to treatment allowing predictability and effective, fast and minimally invasive procedures. The goal is to develop a treatment plan having benefits in the parameters of high-end esthetics and minimal invasiveness. Management of peri-implant tissues is concerned with providing natural outcome of a smile. By undergoing a specific protocol of treatment, satisfying results are achieved independent of the employed implant system [1, 2]. Insertion protocol using an undersized drill so as to obtain a good primary stability 2. When will be the periodontal treatments become a decision for inserting an implant? There are many articles reporting high success rates (having no radiographic changes) in case of immediate implant placement in fresh extraction socket of a periodontally compromised tooth [3-4]. Systemic and controversial antibiotics are used preoperatively, until the contrary trials have proved otherwise. Immediate implant placing and loading have shown to be clinically reliable having high rates of success. Drawing from the current literature and on experience, it is reasonable to affirm that: rate of success in implant supported restoration in full-arch cases in the maxilla is 97% and for mandible at 98%. In case the periodontally treated tooth is mobile and is infected after one year of treatment, and height of residual bone is less than 10 mm, tooth must be extracted and implant placed. This is minimally invasive treatment, and prevents vertical grafting and gives the patient fixed construction [4-5]. The integration of tooth into implant construction is performed under these conditions, according to the recent studies, statistics and the experience Karpiński T. In case, the tooth has prognosis of ten years and prosthetic reconstruction permits the tooth extraction, and it is possible to sustain prosthetic reconstruction with minor modifications, then the tooth can be taken for reconstruction [8]. If tooth has prognosis less than 5 years, it cannot be included in reconstruction. Under the above-mentioned conditions, the prognosis for the restoration on the implants will be twenty years, of the patient has the occlusion and hygiene control and has a professional cleaning once every 4 months. Under these parameters, the individual diagnosis and planning are the next stage [8-9]. The technician has to work with appropriate inter-dental brush for allowing proper cleaning of the prosthesis that could be screw retained or cemented. It is a well-known fact that the edentulous or partially edentulous patients could be having muscular dis-coordination, even if there are no symptoms observed. This discoordination could be drastic in case arch is restored on the implants, titanium or Zirconia abutments or e max crowns that do not exhibit resilience, tolerance or elasticity. So, it is realized that occlusion should be perfect in habitual, centric and lateral movements [4-10]. It is essential to understand the exact 3D shape and the architecture of the defect for knowing the design of the flap [3]. In this software program clinician and dental technician is able to virtually place the implant and run number of test for ensuring best location outcome [13-15]. The patient is also one of the 3D “parameters” whose character could be implemented and improved with the help of high quality support of Karpiński T. Static records that are used to record the smile include radiographs, study models and film/digital photographs (Fig. The American Academy of Cosmetic Dentistry Photographic Accreditation Review of 1995 recommended that facio-maxillary photographs for aesthetic treatment planning should have full face smiling, full face showing lips relaxed, profile full smile, and left and right lateral views of full smile [17-20]. Videoclips recorded before, during, and after the treatment allows the dentist to check the dynamic display zone in the front view during facial animation; such videoclips can be utilise to comparison and assess the effects of aesthetic treatment and face change over time. In addition to this, the diagnostic information, which is acquired from dynamic visualization of the smiling face, video imaging has the potential to affect communication at staff meetings and consultations [21-26]. In case of full-arch rehabilitation, it is necessary to respect certain dimensions. As maxillary implants get inserted in palatial section of sockets, it is required for the technicians to measure inter-premolar distance to give the dimensions of initial dental crowns. Taking into consideration of all these parameters that ensure common workflow with the technician and common language, he or she will be ready to create a mock up or wax-up of the ideal situation [31].