
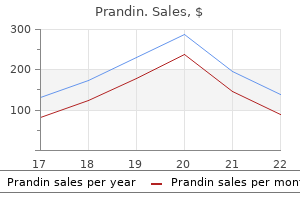
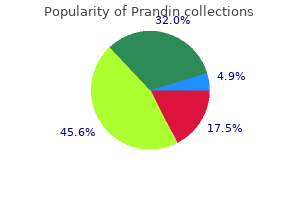
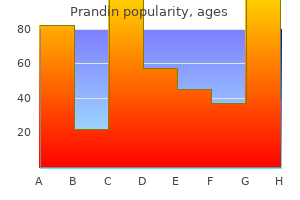
Prandin
2mg prandin overnight delivery
Endotoxins are also problematical; some are often referred to as pyrogens as they indirectly the active ingredient is often present at relatively low induce fever diabetes mellitus diagnosis and screening discount prandin 1 mg visa. They are mainly fragments of microbial concentrations, particularly in pharmaceuticals, but if it lipopolysaccharides liberated from mostly Gram is attacked the product is rendered useless. These active negative bacteria, although some may originate from ingredient may be therapeutic or antimicrobial agents, fungi and other microorganisms. It is vitally important and in cosmetics and toiletries they are mostly deter to eliminate them from injectable products. Examples of attack on quently, ultrapure water, free from these materials, is active ingredients include breakdown of antibiotics used in the manufacture of intravenous drugs and in capsules, tablets and in solution. In addition, aspirin and heroin are both broken ture of the ingredients, the physicochemical characteris down by the bacterium Acinetobacter lwoffii. Atropine, tics of the product and the inoculum of biodeteriogen an alkaloid used in eye preparations, is degraded by that initiates attack. However, any organisms found Pseudomonas and Corynebacterium species, and hy when measurable changes become detectable may not drocortisone is attacked by the fungus Cladosporium necessarily be those responsible for initiating the attack: herbarum. In fact, several organisms In many cosmetics and toiletries, the active ingredient may have been involved in sequential attack from initia is a detergent. Shampoos, for example, often contain tion to the point when changes become detectable. Breakdown results in reduced lathering clude odours resulting from the production of organic properties and may generate unpleasant odours, partic acids, fatty acids, amines, ammonia and hydrogen sul ularly hydrogen sulphide resulting from the reduction of phide. For detergents, there must be a compromise alter the pH, which can markedly affect physical prop between resistance to attack in use, and biodegrad erties, including viscosity and colour. Spoiled creams ability once the material enters the sewage system and and lotions may also develop lumps and slime, or environment. The fatty Factors in uencing microbial spoilage acids may then be broken down via b-oxidation to form odorous ketones. Even semisolids with high fat/oil con Microbial growth is determined by the nutrient status of tent are not immune, as fungi may grow in surface lms the product formulation, its pH, oxygen concentration, of moisture. The size and composi liners must be impregnated with preservative to avoid tion of the microbial inoculum is obviously of major this problem. Sources include the raw materials, and contamination during stages of manufacture, packag Assessment of microbial contamination ing and storage, and while in use. The life of the product (microbiological quality control) from manufacture to sale, and the duration and treat ment received while in use are crucially important. Some Microbial quality control is conducted to: of these products can spend several months or longer in 1 monitor microbial contamination of raw materials; a warm humid bathroom. During this time they may be 2 monitor and con rm the efficacy of operations such subject to repeated challenge by microorganisms. For as sterilization; example, a jar of hand cream is challenged each time the 3 control the danger from pathogenic microorganisms user takes a sample. Water activity can be reduced by the presence For products that must be sterile, the detection of of solutes such as salts or polyethylene glycol, but it is viable organisms is crucially important, as the presence difficult to prevent moisture lms from developing on of any viable organism is evidence of process failure. Consequently, surface biodete some products the sterilization treatment may be severe, rioration can occur on what may essentially be a resis. Most biodeterioration of cosmetics and process may apparently be free from viable organisms, pharmaceuticals is due to aerobic and facultative but it is only after days or weeks that survivors recover microorganisms. Removal of oxygen would of tests is vitally important in determining the efficacy of therefore prevent most spoilage. Product pH also deter Additional evidence of microbial activity within a prod mines the effectiveness of the preservatives. Many of uct may come from changes occurring to the pH, viscos those allowed become less effective as the pH is raised ity, emulsion stability, etc. Some product changes of this nature occur, biodeterioration is components may assist microbial survival. Sensitive analytical tests are available for the Package design also in uences the susceptibility of a detection of very low levels of mycotoxins. Some plastics are perme of endotoxins (pyrogens) can be determined by febrile able to oxygen and moisture, which may support micro response in animals such as rabbits, or now more bial activities. Cap liners are often made of cork or readily via the Limulus test (amoebocyte lysate assay). From here crab (Limulus polyphemus), which clot in the presence they can go on to invade the product. This test is very sensitive and can detect Microbial biodeterioration of materials and its control 255 as little as 10-12g/ml. The detection of microbial en activity spectrum, solubility, stability, volatility, zymes is often important, as they too can persist after toxicity, irritancy, colour, odour, taste, the pH of the cell death. In many cases the product biodeteriogens, or a group of standard organ actual quantity of preservative that is available for isms is frequently used in the testing of cosmetics antimicrobial action may be only a small portion of and pharmaceuticals, which normally includes the total preservative present in the product. Pseudomonas aeruginosa (Gram-negative), Staphylo Nevertheless, the remaining unavailable preservative coccus aureus(Gram-positive), Candida albicans(yeast) can still contribute to the possible toxicity or irritancy to and Aspergillus niger (lamentous fungus). Al Many cosmetic and pharmaceutical products are ternatively, repeated sequential challenges may be given multiphase systems. In emulsi ed products available preservative may be considerably reduced because Factors affecting the performance of preservatives many undergo partition, predominantly into the oil the aim of incorporating preservatives into many of phase, or are solubilized into surfactant micelles. Once these products is to kill or inhibit the growth of microor within the oil phase or micelle, the preservative is not ganisms that enter during the repeated use of the prod immediately available to act on contaminating micro uct, as relatively few products are of the single dose type. The extent of the distribution is dependent As little preservative as possible should be used and upon the partition coefficient, and many preservatives wherever feasible the least toxic one that will do the job. Further loss of available preservative may by microorganisms; overdosing with preservative occur through weak bonding with non-micellar surfac agents is uneconomical, has greater toxicity and can tants and hydrocarbon polymers, and adsorption to lead to greater environmental pollution. Ideally, preservatives should be: the oil phase ingredients 1 broad spectrum, effective against all microorganisms likely to enter the product; 2 free from toxicity, irritancy and allergenicity to the Aqueous phase user; preservative 3 stable, able to withstand production procedures and the life of the product; Inactive form Degraded 4 compatible with all other formulation ingredients;. Thiomersal mercuric chloride and related compounds Quaternary ammonium Are cationic surfactants that disrupt cell membranes. Activity reduced by organic matter, more effective against Gram-positive bacteria chloride than Gram-negative bacteria, yeasts or moulds. Benzalkonium chloride acts synergistically with phenyl mercuric nitrate Phenolic compounds Denature proteins and disrupt cell membranes. Used as antiseptics at low concentrations, and as disinfectants at higher concentrations. Preservative of cosmetics and pharmaceuticals, and many other materials Organic acids and Includes propionic acid and propionates, sorbic acid and sorbates (0. Active at acid pH, causing membrane disruption; possible role in toothpaste, skin creams and lotions Packaging can also in uence the effectiveness of the Table 16. Also, their adsorption to rubber, c (K w) in cork or card cap inserts can reduce preservative action. However, some formulation components aid preserva Preservative Liquid paraffin Vegetable oil tion, performing as activators or collaborators. Microbial biodeterioration of materials and its control 257 Often there are great bene ts to be gained from the Cain, R. These may Books include changes in colour, tensile strength or elasticity, Allsopp, D. Institution of Chemical very favourable conditions for the microorganisms, Engineers, Rugby. Academic biogenic weathering of calcareous litharenite stones caused Press, London. Animal Animal cell culture is predominantly used in the produc cells, particularly those from mammals, usually demand tion of a wide range of health-care products, including very complex media (see Chapter 5), but genetic modi therapeutic and analytical proteins, monoclonal anti cation of cells is being used to reduce their reliance on bodies and viral vaccines (Table 17. The separated cells may then be airlift systems of capacities up to 10000 and 2000L, re grown as a primary culture. Anchorage-dependent cells must be immobi dependent and must be cultured as a monolayer on solid lized or entrapped, using stationary monolayer cultures, support materials.
Discount prandin 1 mg otc
Recurrent cellulitis after coronary bypass sur ed cloths to prevent skin and soft-tissue infection in Marine recruits: a gery diabetes friendly foods purchase line prandin. Association with super cial fungal infection in saphenous venec cluster-randomized, double-blind, controlled effectiveness trial. Skin and soft-tissue infections requiring hospitalization at an academic Philadelphia: Lippincott Williams & Wilkins, 2004. Rapid resolution of cellulitis in and preventive antibiotic therapy: timing, duration and economics. Antibiotic and prednisolone therapy of erysip crobial prophylaxis in surgical procedures. Infectious Diseases Society elas: a randomized, double blind, placebo-controlled study. Relapse of erysipelas following treatment with advisory statement from the National Surgical Infection Prevention prednisolone or placebo in addition to antibiotics: a 1-year follow-up. Use of corticosteroids in treating infectious ple-dose antimicrobial prophylaxis for major surgery: a systematic re diseases. Timing ofantimicrobial pro bacterial cellulitis and erysipelas of the leg in the Netherlands. A predictive model of lowing total hip arthroplasty: timely administration is the most impor recurrent lower extremity cellulitis in a population-based cohort. Principles and practice of infec ized patients: a prospective case-control study. Incidence of adverse events temic antibiotic therapy in localised wound infections among hospital and negligence in hospitalized patients. Optimal imaging strategy for community-acquired caused by community-associated methicillin-resistant Staphylococcus Staphylococcus aureus musculoskeletal infections in children. Septic pulmonary emboli and bacter infections associated with a toxic shock-like syndrome and scarlet fever emia associated with deep tissue infections caused by community-ac toxin A. Necrotizing soft-tissue infection: diagnosis in an outbreak of disease among military trainees in San Diego, Cali and management. Linezolid compared with beta-lactam antibiotic treatment for invasive Strepto versus vancomycin in treatment of complicated skin and soft tissue in coccus pyogenes infection. Life-threatening clostridial infec macrolide and multidrug-resistant Streptococcus pyogenes isolated tions. Catching up with important players in atheroscle caused by Clostridium perfringens. Macrolide resistance mycin, rifampin, tetracycline, metronidazole, and penicillin for effica and emm type distribution of invasive pediatric group A streptococcal cy in prevention of experimental gas gangrene due to Clostridium isolates: three-year prospective surveillance from a childrens hospital. Comparative in vitro activity of ertapenem and 11 view of 21 consecutive patients. A comparative double blind study of acquired, methicillin-resistant Staphylococcus aureus infection. Clinical presentation and bacteriologic analysis of infected human matosis: microbiology, histopathology, clinical presentation, diagnosis bites in patients presenting to emergency departments. Prophylactic antibiotics in common dog bite wounds: a therapeutic strategies for melioidosis and glanders. Antibiotic prophylaxis for bac forms of certain cephalosporins, erythromycin, and oxacillin against terial infections in afebrile neutropenic patients following chemother Pasteurella multocida. Infectious complications those of selected macrolides and other agents against aerobic and an among 620 consecutive heart transplant patients at Stanford Univer aerobic pathogens isolated from soft tissue bite infections in humans. Antibiotic suscep bination with blood cultures for improvement of microbiological doc tibilities of human isolates of Pasteurella multocida. Detection and identi cation of microorganisms by gene am tions for vaccine use and other preventive measures. Successful treatment pro 2010 update by the Infectious Diseases Society of America. Anthrax as a biological infectious complications among hematopoietic cell transplant recipi weapon: medical and public health management. Management of gram-positive Signi cance of aspergillemia in patients with cancer: a 10-year study. What can we learn from studies comparing line mucormycosis (Rhizopus rhizopodiformis) of skin and subcutaneous zolid with vancomycin in neutropenic patients when vancomycin dosag tissue: epidemiology, mycology and treatment. Efficacy and safety of linezolid compared with vancomycin in a experience at a cancer center and review. Nontuberculous mycobacterial infection in patients with neutropenia during cancer chemotherapy. Cellulitis and nodular skin lesions infections in patients with haematological disorders. Cryptococcal panniculitis in an im treatment of invasive fungal infection in patients with cancer and neu munocompromised patient: a case report and review of the literature. Committee on Infectious Diseases, American Academy for preventing varicella-zoster virus disease after hematopoietic cell of Pediatrics. General Warfarin sodium is an orally administered anticoagulant drug that is marketed most commonly as Coumadin. Pharmacogenomics as a science examines associations among variations in genes with individual responses to a drug or medication. This would be an once-in-a-lifetime test, absent any reason to believe that the patients personal genetic characteristics would change over time. Have received fewer than five days of warfarin in the anticoagulation regimen for which the testing is ordered; and 3. Are enrolled in a prospective, randomized, controlled clinical study when that study meets the following standards. The research study is well-supported by available scientific and medical information or it is intended to clarify or establish the health outcomes of interventions already in common clinical use. All aspects of the research study are conducted according to the appropriate standards of scientific integrity. The research study has a written protocol that clearly addresses, or incorporates by reference, the Medicare standards. The clinical research study is not designed to exclusively test toxicity or disease pathophysiology in healthy individuals.
Diseases
- Photoaugliaphobia
- Charcot Marie Tooth disease deafness recessive type
- Letterer Siwe disease
- Pillay syndrome
- Charcot Marie Tooth disease type 4B
- Collins Sakati syndrome
- Arthrogryposis multiplex congenita, distal type 1
- Renal cancer
- Paramyotonia congenita of von Eulenburg
- Maffucci syndrome
Cheapest prandin
Media concentrations normally need be no manganese diabetes test edmonton buy prandin 0.5mg amex, molybdenum, nickel, selenium and zinc, are greater than 100mg/L. Sulphur is required for the production of the sulphur containing amino acids cystine, cysteine and methion ine, and some vitamins. Many bacteria can grow on media merely con Main elemental cell composition = C4H7O2N taining carbon and energy sources, and basic mineral elements. Microorganisms that are able to grow on this minimal medium are referred to as prototrophs. How Other minor elements, mostly calcium, iron, potas ever, other microorganisms must be given speci c com sium and magnesium, must be provided in relatively pounds in a part or fully constructed form. Several minor elements are essential for speci c substances, such as amino acids or vitamins, are called enzyme activities. Few mi have structural roles: magnesium ions are involved in the croorganisms require fat-soluble vitamins (A, D, E and stabilization of ribosomes, and some are necessary for K); and vitamin C, although often improving growth, is maintaining cell wall and membrane integrity. Nutrients from the environment must be transported across the cell membrane into the cell. This is often the Trace elements rate-limiting step in the conversion of raw materials to Trace elements include cobalt, copper, manganese, products and therefore is of major importance to indus Microbial growth and nutrition 23 trial fermentation processes. This is referred to as group translocation, which is Such nutrients are usually soluble in lipids and can performed by many prokaryotic cells. During periods when nutrient concentrations are very However, it is an inefficient mechanism, as the rate low, as during the stationary phase of a batch culture of uptake is dependent on the magnitude of the (see below, Microbial growth kinetics), some organisms concentration gradient across the membrane. Most produce metabolites capable of scavaging for remaining solutes must be transported via speci c active mecha metal ions. Sideramines, which include the hydroxam nisms, because membranes are selectively permeable. Alterna Also, microorganisms usually inhabit natural environ tively, some microorganisms may produce compounds ments where nutrient concentrations are low. Conse whose role in vivo is to render their membranes more quently, it is essential that they can accumulate solutes permeable to certain metal ions. Most solute uptake involves carrier proteins (per Utilization of high molecular weight materials meases) that span the membrane. It Utilization of polymeric substrates (polysaccharides, is driven solely by the concentration gradient across the proteins and lipids) requires additional activities. However, nutrient uptake zoa and other eukaryotic organisms without cell walls into the cell continues, because their intracellular con can ingest relatively large pieces of food materials from centration does not increase, as they are immediately their environment by phagocytosis (engulfment) into metabolized on entry. Hy prokaryotes, is used to transport sugars and amino drolytic enzymes are then secreted into the vacuole acids, and their selective carriers usually function for a to break down the polymers to their constituent group of related solutes. For organisms with a rigid cell wall this rates, at least up to concentrations at which the carrier is not usually possible. Many of these extracellu which is important in environments where nutrient lar enzymes have major industrial applications (see levels are low. As in fa Microbial growth can be de ned as an orderly cilitated diffusion, protein carriers are involved; many increase in cellular components, resulting in cell are highly speci c, whereas others function with groups enlargement and eventually leading to cell division. Where proton gradients are de nition is not strictly accurate as it implies that a involved (see Chapter 3, Electron transport), the nutri consequence of growth is always an increase in cell ent entering the cell, such as a sugar, amino acid or or numbers. However, under certain conditions growth ganic acid molecule, is simultaneously transported with can occur without cell division, for example, when cells a proton, and is referred to as symport. Here sodium ions leave the cell bers remain constant, but the concentration of biomass in exchange for the entry of protons, which is termed continues to increase. The sodium gradient established drives uptake organisms, such as some fungi, that are not divided into of nutrients. Their growth results only in increased Some compounds may be modi ed during uptake. Sugars, for example, can be phosphorylated using Growth kinetics of homogeneous unicellular suspen 24 Chapter 2 sion cultures can be modelled using differential equa Microbial fermentations in liquid media can be car tions in a continuum model. Batch and assemblages, particularly bio lms, colonies, ocs, growth involves a closed system where all nutrients mats and pellicles, is much more complex. In fact, het are present at the start of the fermentation within a erogeneous systems require a very different approach xed volume. The only further additions may be acids using cellular automaton and Swarm system models, or bases for pH control, or gases. In fed-batch systems fresh medium or medium isms and heterogeneous systems will not be discussed components are fed continuously, intermittently or are here. Continuous fermentations binary ssion in homogeneous suspension cultures, are open systems where fresh medium is continuously where cell division produces identical daughter cells. Therefore, the generation time or doubling time (td) is the time required for a microbial population Batch growth to double. Theoretically, after one generation, both the microbial cell population and biomass concentration During batch fermentations the population of microor have doubled. However, as previously stated, under ganisms goes through several distinct growth phases: certain conditions growth can be associated with an lag, acceleration, exponential growth, deceleration, sta increase in biomass and not cell numbers. In the lag phase virtually no eration time recorded during microbial growth is in re growth occurs and the microbial population remains ality an average value, as the cells will not be dividing at relatively constant. At any one time there are cells at metabolic activity as the microbial inoculum adapts to different stages of their cell cycle. However, under certain conditions fresh medium they may be de cient in essential enzymes, synchronous growth can be induced so that all cells vitamins or cofactors, etc. The chemical composition of the fermen Microorganisms able to sporulate produce spores for survival during stationary phase Deceleration Stationary Death phase Exponential Acceleration Idiophase* Lag (secondary metabolism) Trophophase* Only observed in some Fig. Microbial growth and nutrition 25 tation media in uences the length of the lag phase. Physiological stress may the product is a curve with a constantly increasing slope also have an effect, especially as cells are often trans. Generally, inocula prepared from cells har equation: vested in the exponential growth phase (period of most rapid growth) exhibit shorter lag phases than those har x =x emt 2. Mathematically, this exponential growth can be +mxwherem=gradient (min equation 2. For cell biomass, exponential phase, a plot of natural log of biomass con growth can be considered as an autocatalytic reaction. This can be described as follows: (a) (b) Gradient= 0 50 100 150 200 0 50 100 150 200 Time (min) Time (min) (c) Fig. However, under conditions where an essen log, the gradient of the semilog plot is equal to m/2. If we consider a hypothetical If we consider a situation where at time zero, the cell case where the microbial cell population at this point biomass is xo, then after a xed period of time (t) of ex of exponential growth is one (No=1), we can describe ponential growth, equivalent to one doubling time (td), binary ssion as follows: the microbial biomass will double to 2xo, i. After a certain time the of exponential growth is determined by dividing by the growth rate decreases and eventually stops. This cessa time period (t): tion of growth can be due to depletion of essential nutri ln N ln N ents (carbon source, essential amino acids, etc. This divisions per hour, unit time, but rather in the mean gen impact of essential nutrient depletion on growth can eration time or doubling time (td), that is, the time be described mathematically by the Monod equation, required to undergo a single generation that doubles the in a form similar to that used in biochemistry, population. Substrate concentration (g/L) S = concentration of limiting substrate (g/L); Ks = satu leased from lysed cells, and in some cases producing sec ration constant, concentration (g/L) of limiting nu ondary metabolites. The duration of the stationary trient enabling growth at half the maximum speci c phase varies depending on the microorganisms involved growth rate, i. However, as the level of this substrate decreases, it eventually becomes limiting and During batch fermentations certain environmental can no longer sustain mmax. This is the beginning of the conditions continually change, particularly nutrient deceleration phase. As the residual concentration of the and product concentrations, as does the speci c growth limiting substrate approaches Ks and then falls below rate, because the cells must pass through the sequence this concentration, there is an accompanying gradual of growth phases described above.
Quality prandin 2mg
The malo-lactic 11 greater dihydroxyacetone phosphate reductase and fermentation reduces the acidity through the decar glycerol phosphatase activities to increase glycerol boxylation of this dicarboxylic acid to lactic acid diabetes type 2 medication metformin buy genuine prandin on line, a levels. Where malo-lactic Also, strains suitable for immobilization may be use fermentations are required, suitable lactic acid bacteria ful for some purposes. For example, their use in produc such as Leuconostoc oenos may be speci cally inocu ing sparkling wine is currently being examined. Not only is acidity reduced, but other useful avour components are produced and the wine becomes Continuous wine fermentation more microbiologically stable. It is rare for other Continuous fermentation has potential advantages microorganisms to grow in wine after it has been sub over batch systems (see Beer brewing p. This has been attempted in southern France for the production of Following fermentation the wine must be protected red wine using fermenters of 500000L capacity. Over against both microbiological and non-microbiological 150000kg of grapes are processed each day and a corre spoilage, particularly oxidation. Al ternatively, the winemaker may choose to leave the wine on the yeast sediment (lees) for 2 weeks to 9 months, in Secondary wine fermentation order to release more yeast avour compounds. It also protects the wine against chemical further activities of yeasts or other microorganisms. Some wine is stored for a period of a few carbonated sparkling wines, or the growth of aerobic weeks to several years in wooden casks, where it ac surface/ lm yeasts to produce no sherry; or lactic acid quires additional avour characters. Ultimately the bacteria may be encouraged to perform a malo-lactic wine is ltered, pasteurized or sterile ltered, and lled fermentation. Some may be glucose, with only small quantities of other simple served as naturally conditioned cask cider, analogous to sugars, oligosaccharides and starch. However, most ciders are clear contains soluble pectin, which consists of polymers of and sterile ltered or ash pasteurized products. The major are arti cially carbonated and analogous to bottled and acid is l(-) malic acid, along with variable quantities keg beer. In France, carbonation may be achieved via the of the phenolic acids: quinic, chlorogenic, shikimic Charmat process. Polyphenolic constituents are some sparkling wines, involves a bulk secondary fer tannins, primarily epi-catechin, and dimeric and trimer mentation under pressure. Other minor components include ascorbic acid, minerals and esters such as ethyl-methyl butyrate. Single apple cultivars can be used, Traditional wooden fermentation casks are used with but more often cider is prepared from blends. Fermenter depths in mace, consisting of skin, pips and core, can be used for excess of 14. Cane sugar is the usual source of additional the production of concentrate as furfurals (sugar degra fermentables, without which alcohol levels rarely ex dation product) may be formed, which could impede ceed 6. These are primarily Apple juice composition varies depending upon the Kloeckera apiculata, Aureobasidium pullulans and apple varieties used. Compared with brewers wort, it species of Rhodotorula, Torulopsis, Candida and Met has a lower pH of 3. A typical sugar ria such as Gluconobacter species are usually present composition is 75% fructose, 15% sucrose and 10% but lactic acid bacteria are rare. However, levels of Food and beverage fermentations 199 microorganisms rise if the fruit is allowed to fall to derived from the enzymic degradation of pectin. As a result, cider does not clear as pectins lease nitrogenous compounds into the cider, including remain undegraded unless additional pectinases are amino acids and peptides, along with pantothenic acid, added. In many countries the maximum legal limit racked (decanted from the sediment) or partially clari for sulphur dioxide is around 200mg/L, which ade ed by centrifugation before storage under an inert gas quately retards aerobic yeasts, and both lactic and acetic blanket for several months. These yeast preparations origi nate from cider fermentations or may be selected wine Naturally carbonated cider is a relatively small propor making strains. Lower soluble nitrogen levels, tion of the market and is produced by carrying out a sec compared with brewers wort, lead to relatively slow ondary yeast fermentation. However, a more common fermentation rates, which is exacerbated by the lower secondary fermentation is malo-lactic fermentation (see concentrations of yeasts used for pitching. It is only 106cells/ml, rising to 5 107cells/ml by the end of performed by lactic acid bacteria, usually non-slime the fermentation. Supplementing the juice with ammo forming strains of Leuconostoc mesenteroides, Lacto nium salts does not increase the fermentation rate, but bacillus collinoides and occasionally Pediococcus makes its progress more predictable. Ideally, the cider yeasts should exhibit the the conversion of quinic acid to dihydroshikimic acid following properties: and generates other avour compounds. The fermentation is pitched to give an initial yeast of sugars derived directly from plant extracts and concentration of 2 107cells/ml that increases to 2 108 fruit juices, or indirectly from hydrolysed grain and cells/ml by the end of the fermentation. Distillation residues may be used as that are desirable alcoholic beverages in their own an animal feed supplement. Others tion of these intermediate products results in whisky such as Scottish grain, bourbon and rye whiskies are dis from unhopped beer, and brandies from wine and cider. Maturation is usually performed in oak casks for several years, the minimum period depending upon the speci c local legislation. Whiskies are prepared from malted barley, exclusively Used casks, which have previously held sherry or bour in the case of Scottish and Irish malt whiskies, or with bon, can also be used to impart particular characteristics various proportions of added cereal starch for other to the whisky. Wood components, referred to as wood whiskies, such as bourbon, grain and rye whiskey. The malt, and other cereals include aromatic aldehydes, lactones, furfurals and where used, are extracted and sacchari ed to form a tannins. In some cases, the Vinegar production whole mash is fermented rather than separating the spent grains from the wort and is termed in grains fer the normal course of events when a natural solution of mentation. Certain fermentations, referred to as sour fermentable sugars (fruit juice or other plant extracts) is mash, also have a preliminary fermentation with lactic exposed to indigenous microbial activities is an alco acid bacteria, usually Lactobacillus delbrueckii. The yeast fermenta sufficient acetic acid is produced it may be classi ed as tion is then performed by speci c distilling strains of S. This term is derived from the French words vin cerevisiae, which are sometimes supplemented with (wine) andaigre(sour). Some whisky yeasts are able a condiment that contains a minimum of 4% (w/v) to ferment maltodextrins because they are hybrids acetic acid. Food and beverage fermentations 201 Vinegars have been produced for several thousand. Other minor products include acetalde years from local fermentable substrates and alcoholic hyde, ethyl acetate and acetoin. They are mainly produced from fruit juices bacteria are members of the genera Acetobacter and and sugar syrups, including maple syrup, molasses and Gluconobacter, mostly A. Where alcohol sources are used di some instances, mixed cultures are more efficient than a rectly, including wine, cider and spirit alcohol, they re single organism.
Cheap prandin 1 mg with visa
The posterior placenta praevia is difficult to be identified due to shadowing from the presenting part of the foetus signs ng diabetes order prandin 1 mg with visa. This can be overcome by head-down tilt of the patient or displacing, the presenting part manually. If difficulty still present, the distance between the presenting part and the promontory of the sacrum is measured. El-Mowafi In mid pregnancy the placenta reaches the internal os in up to 20% of pregnancies. With increasing gestational age and the formation of the lower uterine segment, a gap develops between the placental edge and the internal os " placental migration". So it is recommended to repeat scan when placenta praevia is diagnosed in mid pregnancy. Ultrasonography for: differentiation between abruptio placentae (retroplacental haematoma in a normally implanted placenta), marginal bleeding (separation of the margine of a normally implanted placenta) and placenta praevia (in the lower uterine segment), assessment of foetal viability age, position and presentation. Then management is carried out as following: (I) If the patient is not in labour: Look to the amount of bleeding; If the bleeding is severe, continue antishock measures and do immediate caesarean section. If the bleeding is slight, look to the gestational age; If completed 37 weeks (36 weeks by some authors) or more, pregnancy is terminated by induction of labour or caesarean section (see later). At this time, the foetus is mature and the mother will be in a risk of severe haemorrhage as term file:///D|/Webs On David/gfmer/Books/El Mowafi/Bleeding in late pregnancy. If less than 37 weeks (36 weeks by others), conservative treatment is indicated till the end of 37 (or 36) weeks but not more. Conservative treatment: the patient is kept hospitalized with bed rest and observation till delivery. According to the findings, the patient will be delivered either vaginally by amniotomy + oxytocin or by caesarean section. Vaginal delivery is allowed if the following findings are fulfilled: Placenta praevia is lateralis or marginalis anterior, bleeding is slight, vertex presentation, adequate pelvis with no soft tissue obstruction. Amniotomy has 2 benefits: Allows descent of head so it compresses the placental site preventing further bleeding. As the bulging of fore bag of water during contractions with intact membranes will drag the edge of the placenta evoking more bleeding. Caesarean section is indicated in: Placenta praevia centralis whether complete or incomplete even if the foetus is dead. Other obstetric indications as contracted pelvis, cord prolapse and elderly primigravida. If placenta praevia was anteriorly implanted it is gently displaced laterally to reach the foetal head otherwise cut through it (not preferred). Hypertensive disorders of pregnancy (30%) due to spasm and degenerative changes in the decidual arterioles. Passive congestion of the uterus due to pressure of the gravid uterus on the inferior vena cava. Pathogenesis q Separation of the placenta results in formation of a retroplacental haematoma and its extension leads to more separation of the adjacent placental tissue (concealed haemorrhage). Dark vaginal bleeding results from escape of blood from the retroplacental haematoma. Signs: (A) General examination: 1 Shock is usually present and may be marked and not proportionate to the amount of visible bleeding due to: file:///D|/Webs On David/gfmer/Books/El Mowafi/Abruptio placentae. El-Mowafi concealed and/ or revealed haemorrhage, overdistension of the uterus and damage of the myometrium causing neurogenic shock. Ultrasound: detects normally sited placenta with retroplacental haematoma that may dissect the placental margin. Assessment of the patients condition, general and abdominal file:///D|/Webs On David/gfmer/Books/El Mowafi/Abruptio placentae. Delivery: Patient with abruptio placenta has to be delivered and usually there is no place for conservative treatment. Postpartum: the patient is more liable for postpartum haemorrhage so oxytocin is continued after delivery of the foetus, methergin is given with delivery of the shoulders if there is no hypertension with continuous massage of the uterus. Signs: (A) General examination: the general condition proportionates to the amount of bleeding as all the blood loss is revealed (B) Abdominal examination: No characteristic signs. Investigations Ultrasound reveals a normally situated placenta in the upper uterine segment with no retroplacental haematoma. Ruptured Vasa Praevia In velamentous insertion of the cord, some of the foetal vessels in the membranes cross the region of the internal os. When the membranes ruptures, the foetal vessels are torn and bleeding occurs which is usually slight. Apts test: 4-6 drops of the antepartum haemorrhage blood is added to 10 ml of water then 2 ml of sodium hydroxide is added. The foetal blood remains red/ pink for at least 2 minutes and turns green/brown after 10-20 minutes due to resistance to alkali in formation of alkaline haematin. Spectrophotometer: Foetal haemoglobin shows different ultraviolet absorption than adult haemoglobin. Differential Diagnosis of Antepartum Haemorrhage Placenta Praevia Marginal Haemorrhage Abruptio Placentae (I) History: Painless, causeless, recurrent. These two conditions usually start between the 4th and 6th weeks of pregnancy and improves or disappears about the 12 th week. Hyperemesis gravidarum: the vomiting is not confined to the morning but it is repeated throughout the day until it affects the general condition of the patient. Brain: congestion and petechial haemorrhages in the brain stem resembling that of Werniches encephalopathy. Finally, there is manifestations of Werniches encephalopathy as drowsiness, nystagmus and loss of vision then coma. Differential diagnosis: Other causes of vomiting as: cholecystitis, appendicitis, pyelonephritis, gastroenteritis, gall bladder diseases, complicated ovarian tumours. Management (A) Hospitalisation: For observation, fluid therapy and competition of neurosis. Antihistaminics that have antiemetic effect as meclozine hydrochloride 25-50 mg twice daily. A preparation contains both meclozine hydrochloride + pyridoxine hydrochloride (vit. Phenothiazine (chlorpromazine=largactil) 5-10 mg three times daily has a tranquilliser and antiemetic effect. Urine analysis: specific gravity, albumin, ketone bodies, chloride and bile pigments. Pulse is persistently above 100/min, temperature persistently above 38oC or the systolic blood pressure is persistently below 100 mmHg. Use nitrous oxide + oxygen for anaesthesia but not agents that affect liver as halothane. Aetiology Increased production or decreased consumption of amniotic fluid will result in polyhydramnios. Clinical Varieties (I) Acute hydramnios: q Very rare, q rapid accumulation of liquor, q occurs before 20 weeks, q the commonest cause is uniovular twins but foetal anomalies are also common. Pressure symptoms: dysponea, palpitation, indigestion, haemorrhoids, oedema and varicosities of the lower limbs. El-Mowafi (B) Signs: 1-General examination: may reveal pregnancy-induced hypertension. Management (A) Acute hydramnios: Termination of pregnancy by high artificial rupture of membranes. This allows gradual escape of liquor thus shock and separation of the placenta are avoided. El-Mowafi Shock results from rapid accumulation of blood in the splanchnic area after sudden drop of intrauterine pressure. Separation of the placenta occurs due to sudden drop of intrauterine pressure and shrinkage of the placental site following this. Termination of pregnancy by high artificial rupture of membranes if the foetus is dead or malformed. However, the amniotic fluid is rapidly reaccumulating and there is risk of premature labour, injury to the foetus or umbilical cord vessels.
Order cheap prandin on line
All measure pregnancy diabetic urine smell cheap prandin 1 mg fast delivery, or had a stillbirth were included only if ments of nuchal translucency were performed and confirmatory genetic testing was performed; those serum samples collected within the gestational without genetic analysis were excluded. For study purposes, one of the authors of aneuploidy if no confirmatory genetic testing used a standard algorithm5 to recalculate risk was performed. A risk of 1 in 100 or higher was the testing for trisomy 13 included only patients who laboratory-designated threshold for classifying a were enrolled after the introduction of the analysis sample as high risk. Our study included pregnant women of all risk levels, and 76% were In this large, multicenter cohort study, we found under the age of 35 years. It has been noted found that such samples were obtained from that the marginal cost for each additional de participants with a higher body weight. If we screening, which means that fewer invasive tests had included in the "not detected" category would have been performed to detect each case. As empha perimental conditions in which previously re sized by professional societies,23-26 the use of ported data were collected. Sinai Hospital, Canada University of California, San Francisco (Miriam Kupperman, (David Chitayat, M. J R Stat Soc D 1976;25:295 sex chromosome aneuploidy using direct G, Birdir C, Touzet G. Gestational age and Board of the International Society for Pre Press, 2010:771-818. Thus, it is important to determine the best cutoff point of the primary screen to optimize the overall cost-effectiveness of a contingent screening policy. Several studies have examined the cost effectiveness of contingent screening policies. Therefore, the optimal cutoff point of a contingent screening policy depends on the economic perspective. We based the cost effectiveness analysis upon a hypothetical cohort, and it is therefore exempt from institutional review board approval. Perspective and time horizon Our analysis included a societal perspective as recommended by many cost-effectiveness guide lines. The societal perspective included immediate costs of screening and the direct and indirect life time costs. The government perspective included the immediate screening costs and direct life time medical and education costs. The payer perspective included only the immediate costs associated with screening. For this, we used a 2 trimester risk cutoff of 1:270 for trisomy 21 and 1:100 for trisomy 18 and 13. Optimization of risk cutoff We determined the optimal cutoff by minimizing the expected total cost by simultaneously varying the decision thresholds for all three tests subject to the constraint that the detection rate had to be at least equivalent to conventional material screening. Because costs varied by perspective, optimal risk cutoffs were determined for each perspective. Once we identi ed the neighborhood of the optimum, we created successively ner grids to identify the optimum risk thresholds. Screen results were classified as "positive" if the post-test risk was equal to or greater than the specified risk cutoff and negative otherwise. Based on those results, age-specific detection and false-positive rates for the risk cutoffs were calculated. During each iteration of the probabilistic sensitivity analysis, the model costs and probabilities were ran domly drawn and a micro-simulation was completed using the drawn values. Following stan dard practice, the costs were drawn from gamma distributions while the probabilities were drawn from beta distributions. The micro-simulations were conducted by simulating 1,000,000 pregnant women at 12 weeks of pregnancy. For each simulated woman, a maternal age was assigned based upon the maternal age distribution reported in the 2012 National Vital Statistics birth data. As standard practice, normal distributions of probabilities were approximated with beta distributions. Lifetime costs represent the average differ ence in direct medical and educational costs between trisomy and an average individual in addition to the indirect costs of lost productivity due to morbidity and mortality associated with this syndrome. We therefore assumed that the survival for trisomy 13 was the same as the survival for trisomy 18 past the first year. We adjusted the medical portion of lifetime costs using the health care component of the personal consumption expenditure index. The list price can serve as an indicator of cost, but list prices show wide variation. Therefore, the variation in price is more likely an indication of variation in profit margins rather than variation in costs. Gamma cost distributions were estimated using the mean and standard deviation values. For contingent screening, we assumed that all primary screens exceeding the risk threshold. Sensitivity analysis Sensitivity analysis was performed using one-way and probabilistic sensitivity analysis. One way sensitivity analyses were conducted to determine the individual impact of each input parameter value on cost-effectiveness ratios. Probabilistic sensitivity analysis was conducted to determine the overall uncertainty in the cost effectiveness due to the combined impact of uncertainty in the underlying model inputs. The objectives and, therefore, the parameters, of a one-way sensitivity analysis differ from the objectives of a probabilistic sensitivity analysis. For example, a one-way analysis may be designed to determine the point at which the best strategy changes (which are not necessar ily plausible), whereas a probabilistic sensitivity should investigate the sensitivity over plausible ranges of the input variables. A screening policy is said to be strictly dominated by another policy if it is both more costly and more expensive. Results the prevalence at 12 weeks was approximately 1 in 301 for trisomy 21, 1 in 1,170 for trisomy 18, and 1 in 3,627 for trisomy 13. In the absence of screening, this resulted in a lower birth prevalence of 1 in 528, 1 in 4,174, and 1 in 7,084 live births for trisomy 21, 18, and 13 respec tively due to spontaneous fetal loss. Societal perspective Both direct and indirect lifetime costs were included in the analysis from a societal perspective. Government perspective Indirect costs were not included in the government perspective. Payer perspective When all lifetime costs were excluded from the analysis, the optimal risk cutoffs resulted in detection rates of 85. The figure below plots the incremental cost and effectiveness results from 1,000 simulations. We conducted our analysis from three different perspectives: societal, government, and payer. The optimal risk cutoff of the primary stage decreased when more downstream costs were included in the analysis. The risk cutoffs were low est when optimized for the societal perspective and highest when optimized for the payer perspective. Under this perspective, the optimized risk cutoffs would result in a 12% increase in the number of total cases detected and a 2. In contrast to a societal per spective, the government perspective excluded the indirect costs from the analysis. Women would only be given the final result and would not be informed of the preliminary false positive result. This approach would spare women the anxiety associated with false positive results. Previous studies have examined the cost effectiveness of changing the risk cutoff in the pri mary screen; however, none of these studies included the downstream costs of trisomy births that result from false negative results. The relevant cost in a cost-effectiveness analysis is the resource cost, or the cost to perform the test. Although prices cannot be used directly, we used prices to estimate underlying costs. We reasoned that the producer with the lowest price is most likely making a profit and the variability in price most likely represents variation in profit margins rather than variation in costs. Further, if the variation in prices reflects variation in costs, the lowest cost producer will eventually dominate and is the most relevant cost for the analysis.
LNA (Alpha-Linolenic Acid). Prandin.
- How does Alpha-linolenic Acid work?
- What is Alpha-linolenic Acid?
- What other names is Alpha-linolenic Acid known by?
- Reducing the risk of heart disease and heart attacks.
- High blood pressure.
- Dosing considerations for Alpha-linolenic Acid.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96991
Purchase prandin us
The role of the echocardiogram in diagnosis and determining the hemodynam ics of various categories of anomalies was considered earlier brain diabetes in dogs generic prandin 1 mg fast delivery. Certainly, a general knowledge of pediatric conditions, especially genetic, is invaluable in identifying a possible etiology for the cardiac anomaly. Therefore, the examiner should not focus initially on the heart but obtain an overall impres sion of the patient. Some syndromes associated with a cardiac malformation, such as Down syndrome, are generally easily recognized because of the features and the frequency of the condition. Although genetic testing has become more widely available and is able to test for a broader range of genetic abnormalities, appro priate application is still uncertain in many instances. The role of genetic testing is evolving and, as time progresses, there may be broader use in patients with a cardiac anomaly. In most patients, there is no obvi ous sign or symptom that suggests a known etiologic agent and they do not need more detailed analysis. In others, there is a readily identi able coexistent condi tion that does not need further testing. As a result of a thorough evaluation, the examiner can usually make a diagnosis and describe with reasonable accuracy the hemodynamics and their severity. Chapter 4 Anom alies w ith a left-to-right shunt in children Shunts at ventricular or great vessel level 96 Ventricular septal defect 97 Large ventricular septal defect 98 Small or medium ventricular septal defects 114 Patent ductus arteriosus 118 History 119 Physical examination 120 Electrocardiogram 121 Chest X-ray 123 Natural history 125 Echocardiogram 125 Treatment 126 Atrial septal defect 127 History 129 Physical examination 130 Electrocardiogram 131 Chest X-ray 132 Natural history 134 Echocardiogram 134 Cardiac catheterization 135 Operative considerations 136 Atrioventricular septal defect 137 History 139 Physical examination 139 Electrocardiogram 140 Chest X ray 141 Pediatric Cardiology: the Essential Pocket Guide, Third Edition. Four cardiac defects account for most instances of left-to-right shunt and half of all instances of congenital heart disease: (1) ventricular septal defect, (2) patent ductus arteriosus, (3) atrial septal defect of the ostium secundum type, and (4) atrioventricular septal defect (also called endocardial cushion defect). In the rst two conditions (ventricular septal defect and patent ductus arte riosus), the direction and magnitude of the shunt are governed by factors that in uence shunts at these sites: relative resistances if the defect is large and rel ative pressures if the communication is small. In most cases, the resistances and pressures on the right side of the heart and pulmonary arterial system are less than those on the left side of the heart, so that a left-to-right shunt occurs. In the last two conditions (atrial septal defect and atrioventricular septal defect), since the shunt occurs at the atrial level in these defects, ventricular compliances in uence the shunt. The left-to-right shunt occurs because the right ventricle nor mally is more compliant than the left. In an atrioventricular septal defect with a large ventricular component, vascular resistances are a major in uence on pul monary blood ow. In certain circumstances, the shunt in each of these four malformations ulti mately may become right-to-left because of the development of pulmonary vas cular disease. This hemodynamic state, sometimes called Eisenmenger syndrome, will be discussed more fully later. The clinical and laboratory ndings of these conditions vary considerably with the volume of pulmonary blood ow, the status of pulmonary vasculature, and the presence of coexistent cardiac anomalies. A tendency for frequent respiratory infections and episodes of pneumonia is common in those with a large shunt. In this chapter, the factors governing ow in a ventricular septal defect and in a patent ductus arteriosus will be discussed in greater detail. This information should be carefully studied and mastered, as it can be applied for understanding 4 Anomalies with a left-to-right shunt in children 97 more complex anomalies that also have a communication between the two sides of the circulation. Overall, a ventricular septal defect is a component in half of all patients with a cardiac malformation. Less frequently they are found either above the crista supraventricularis or in the muscular portion of the septum. Small defects in the muscular ventricular septum create characteristic murmurs in neonates and young infants as pulmonary resistance falls. It is the most common cardiac "defect" (reported in as many as 5% of neonates, as detected by echocar diography). Most small muscular defects close spontaneously within the rst few months of life. When the size of the defect approaches the size of the aortic annulus, ow is governed by the relative pulmonary and systemic vascular resistances. When the defect is smaller, blood ows from the left to the right ventricle because of the higher left ventricular systolic pressure. Because two physiologic mechanisms in uence the shunt, the clinical ndings, natural history, and operative considerations for the two different sizes (large and small) of ventricular septal defects will be considered separately. Large ventricular septal defect In patients whose ventricular septal defect approaches the diameter of the aortic annulus, the resistance to out ow from the heart is determined primarily by the caliber of the arterioles of the systemic and pulmonary vascular beds. Since the systemic arterioles have a thick muscular coat and narrow lumen and the pulmonary arterioles have a thin coat and wide lumen, the systemic resistance is greater than the pulmonary resistance. In an individual with a normal heart, the difference in systemic and pulmonary resistances is re ected by systemic arterial pressure in the region of 110/70mmHg and by pulmonary arterial pressure of 25/10mmHg. Because the pulmonary and systemic blood ows are identical in a normal person, the resistance in the pulmonary arteriolar bed is therefore a fraction of that in the systemic vasculature. Since the ow through a large defect is governed by resistances, any condition that increases resistance to left ventricular out ow, such as coarctation of the aorta or aortic stenosis, increases the magnitude of the left-to-right shunt, whereas any abnormality that obstructs right ventricular out ow, such as coexistent pulmonary stenosis, as in tetralogy of Fallot, or pulmonary arteriolar disease, decreases the magnitude of the left-to-right shunt. If the resistance to right ventricular out ow 4 Anomalies with a left-to-right shunt in children 99 exceeds the resistance to left ventricular out ow, the shunt is in a right-to-left direction. Prior to birth, the pulmonary vascular resistance is elevated and is greater than the systemic vascular resistance. In a neonate, the pulmonary arterioles are thick walled and histologically resemble systemic arterioles. The elevation of pulmonary vascular resistance before birth is supported by observations of the fetal circulation: the right ventricular output enters the pulmonary artery, the major portion ows into the aorta through the ductus arteriosus, and only a small portion enters the gasless high-resistance lungs. The systemic vascular bed has relatively low resistance because of the highly vascular placenta. The proportions of ow in utero to each vascular bed depend on the relative resistances. Immediately after birth, the lungs expand, the pulmonary vascular resistance decreases, and as the placenta is disconnected from the systemic circuit, the systemic resistance nearly doubles. Thus, the pulmonary vascular resistance falls, almost reaching adult levels by the time the child is about 8 weeks of age. Although this sequence occurs in every individual, this decrease in pulmonary vascular resistance has profound effects on patients with a ventricular septal defect. In those with a large ventricular septal defect, the medial layer does not undergo regression either as quickly or to the extent of an normal individual. Therefore, at any age the pulmonary vascular resistance is higher than normal yet lower than the systemic resistance. In patients with a large isolated ventricular septal defect, the systolic pressures in both ventricles and both great vessels are the same, with the right-sided systolic pressures elevated to the same levels as those normally present on the left side of the heart. Because the aortic systolic pressure is regulated at a constant level by baroreceptors, the pulmonary artery pressure (P) is also relatively xed. At birth, ow through the defect is limited, but as the neonate and then young infant grows, the pulmonary blood ow progressively increases. Large ventricular septal defects place two major hemodynamic loads upon the ventricles: increased pressure load on the right ventricle and increased volume load on the left ventricle. In a large defect, the right ventricle develops a level of systolic pressure equal to that of the left ventricle. The right ventricular workload is proportional to the level of pulmonary arterial pressure (P = R Q); pulmonary arterial hypertension results from either increased pulmonary arterial resistance or increased pulmonary blood ow. Since the pressure remains elevated postna tally, the normal evolution of the right ventricle to a thin-walled, crescent-shaped chamber does not occur. The right ventricle is able to tolerate and to maintain these levels of pressure without the development of cardiac failure. In a large ventricular septal defect and left-to-right shunt, volume overload of the left ventricle exists because this chamber not only maintains the systemic blood ow but also ejects blood through the ventricular septal defect into the pulmonary vascular bed. When the ventricles contract, the ow from the left ventricle through the ventricular septal defect is directed almost entirely into the pulmonary artery, and the right ventricle has little additional volume load. The augmented pulmonary blood ow returns through the left atrium to the left ventricle. To accommodate the increased pulmonary venous return, the left ventricle dilates (Figure 4. As dilation occurs, the radius and circumference of the left ventricle increase and the myocardial bers lengthen. Therefore, as the left ventricle dilates and increases its radius, it must develop increased wall tension to maintain ventricular pressure.
Purchase generic prandin from india
Similarly diabetes symptoms yawning discount prandin 0.5mg otc, initially medical assistants applied the varnish at the very beginning of the visit, concurrent with family education. However, the application process upset some children, making subsequent interactions between the child, parent, and provider more challenging for other important well-child visit activities, such as developmental screening; and this lead some care teams to skip applying varnish. Care teams then experimented with applying varnish at the very end of the visit (after the provider had left the room) and after immunizations or other services had been completed. Both changes resulted in an increase in the proportion of eligible patients receiving family oral health education, an oral exam, and fuoride varnish at well-child care visits. Medicaid and private insurance reimbursement amounts are suffcient to cover the cost of our time and equipment, including self-care products for patients who cannot afford them. You will see an impact within just a few years, and youll have all the validation you need to keep going. The Wenatchee Clinics Pediatric Department, which serves primarily Medicaid patients, began delivering integrated preventive oral health care in 2014. Today, they provide fuoride varnish for patients birth through 18 as well as oral health evaluation and family education for patients 5 and under. In this case example, John Donaghy, Practice Manager for Wenatchee Clinics Pediatric Department, shares his practices motivators, success factors, and plans for spread. Motivation "A key motivator for our organization is preventive care, and we saw integrating oral health as a way to help our youth," explains Donaghy. They had testimony from a provider and a staff member who shared how easy this was to do," recalled Donaghy. When we identifed oral health as something we could provide to our patients, I didnt have to make the staff do it; they wanted to do it, and they were willing to be accountable without needing an incentive. A lot of our staff have children, and they know exactly what they would want if they were going to come to an offce," shared Donaghy. A lot of our staff have children, and they know exactly what they would want if they were going to come to an offce. We had to understand the Medicaid reimbursement model and fgure out specifc processes," shared Donaghy. Oral health disparities as determined by selected Healthy People 2020 oral health objectives for the United States, 2009-2010. Surveillance for dental caries, dental sealants, tooth retention, edentulism, and enamel fuorosis United States, 1988-1994 and 1999-2002. Impact of periodontal therapy on general health evidence from insurance data for fve systemic conditions. An overview of childrens oral health-related quality of life assessment: From scale development to measuring outcomes. Burden of oral disease among older adults and implications for public health priorities. Outcome of hospitalizations attributed to periapical abscess from 2000 to 2008: a longitudinal trend analysis. Medicaid Policy Brief: Utilization of dental services among Medicaid-enrolled children. Oral bacterial cultures in nontraumatic brain abscesses: results of a frst-line study. Periodontal infection and preterm birth: successful periodontal therapy reduces the risk of preterm birth. Obstetric outcomes after treatment of periodontal disease during pregnancy: systematic review and meta-analysis. Average time per car (24 hours) taken from time provided by Toyota (18 hours), Honda (21 hours), Ford, (24 hours), and Corvette (32 hours). An Examination of Periodontal Treatment, Dental Care, and Pregnancy Outcomes in an Insured Population in the United States. Medicaid costs associated with the hospitalizations of young children for restorative dental treatment under general anesthesia. Anesthesia for the young child undergoing ambulatory procedures: current concerns regarding harm to the developing brain. Long-term differences in language & and cognitive function after childhood exposure to anesthesia. Causes, treatment, and prevention of early childhood caries: a microbiologic perspective. Invasive dental treatment and risk for vascular events: A self-controlled case series. State Medicaid Payment for Caries Prevention Services by Non-Dental Professionals. Shortage designation: health professional shortage areas & medically underserved areas/populations. Dental care use among children varies widely across states and between Medicaid and commercial plans within a state. The Medical Neighborhood: Integrating primary and specialty care for ambulatory patients. Qualis Health | Oral Health: An Essential Component of Primary Care | White Paper 65 68 Patient-Centered Primary Care Collaborative. Issued by the American Academy of Family Physicians, American Academy of Pediatrics, American College of Physicians, and the American Osteopathic Association. Closing the Divide: How Medical Homes Promote Equity in Health Care: Results From the Commonwealth Fund 2006 Health Care Quality Survey. Initial lessons from the frst national demonstration project on practice transformation to a patient-centered medical home. The Group Health Medical Home at year two: cost savings, higher patient satisfaction, and less burnout for providers. The Future of Patient-Centered Medical Homes: Foundation for a Better Health Care System. The Patient-Centered Medical Homes Impact on Cost and Quality, Review of Evidence, 2013-2014. The development of joint principles: integrating behavioral health care into the patient-centered medical home. Further described in, Patient-Centered Primary Care Home 2014 Recognition Criteria Quick Reference Guide. Accuracy of pediatric primary care providers screening and referral for early childhood caries. Preventing dental caries in children younger than 5 years old: Systematic review to update the U. The role of cultural competency in health disparities: Training of primary care medical practitioners in childrens oral health. Despite increasing optimism about treatment, todays cancer landscape can be challenging as patients have access to an unprecedented amount of information. There are literally millions of cancer-related webpages, blogs, and videos available at your fngertips. A cancer diagnosis can be disorienting, and for many, the overwhelming volume of information available can be more of a burden than an aid. This guide focuses all of the information available about contemporary prostate cancer research, treatment, and lifestyle factors into one consolidated resource. Beyond that, its for any loved one or caregiver who wants to cut through the information noise and get directly to need-to-know information for prostate cancer patient navigation. The Prostate Cancer Foundation is the worlds leading philanthropic organization funding and accelerating prostate cancer research. Since being founded in 1993, the Prostate Cancer Foundation has funded key research leading to many of the treatments used by doctors today to improve the lives of patients, with the mission that someday, soon, no man will die of this disease. Ive never let anything interfere with my treatments, but Ive continued to live the life I want to lead. Prostate cancer starts in the prostate gland, a small gland located below the bladder, that In general, the earlier the cancer is caught and is responsible for secreting one of the components of treated, the more likely the patient will remain semen. The older you are, the more likely you are to be Approximately 95% of all prostate cancers are detected diagnosed with prostate cancer. The 5-year survival rate in the United be diagnosed, the rate shoots up to 1 in 52 for ages States for men diagnosed with prostate cancer is 99%.
Cheap prandin online visa
The anterior surface of the uterus is cut open to show a purplish growth invading the myometrium blood glucose 84 buy online prandin. This 37 years old parous lady was admitted with irregular bleeding P/V following a miscarriage. How the selection of Lesion is seen to invade the myometrium chemotherapy regimen is done The tubes of both sides are coiled, wall How infertility could be explained with genital is thickened and matted with the ovaries. The ovarian cysts (right) are cut Frequency of bilaterality and association with open to show inspissated sebaceous material, hair and pregnancy (p. Excision of the tumor (ovariotomy) causes rapid fall in the serum level of serotonin and disappearance of 5-hydroxy indole acetic acid in the urine. The ascites and pleural effusion resolve spontaneously when the ovarian tumor is removed. The right ovary is hugely enlarged and cut opened to show its solid texture islands of yellow tisue separated by fibrous septa. Malignant: Primary ovarian carcinoma, dysger minoma, immature teratoma, mesonephroma (p. It is a triad of findings including ascites, pleu What are the hormone producing tumors of the ral effusion and benign ovarian fibroma. It is helpful with a known case of ovarian Principles of surgical approach (guidelines) in a cancer: (i) To know the response of treatment. There is exophytic growth Self-assessment on the surface that infiltrates the surrounding organs. The ovaries are found enlarged with lobulated appearance and are free of adhesions. A hugely enlarged cyst is attached to the fimbrial end of the left tube which is stretched out. Pelvic lymph Advantages and disadvantages of radiotherapy adenectomy done (one enlarged node on either side is (p. Self-assessment the anterior surface is cut open to show a fungating Clinical presentation (p. The vulva shows a large exophytic growth and biopsy revealed squamous cell carcinoma. The upper margin of incision is interspin ous, the lower margin is along the inguinal skin creases and the labiocrural folds. As the tubes are patent, the couple should be investigated to assess the ovulatory status and male factors for infertility (Ch. Management if tubes are normal: To assess the male factors and ovarian factors for infertility. Endometrial receptivity is Does the presence of hydrosalpinx impair the reduced resulting in implantation failure. Hysterosalpingogram showing a radio-opaque shadow Metroplasty or unification (Strassman or Tomp filling both the horns of the uterus. There is peritoneal Reproductive behavior in a woman with uterine spillage on both the sides. Symptoms due to metastases are: and epigastric pain, jaundica for liver metastases. In postmenopausal women, the contrast between the junctional zone and the myometrium decreases. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, electronic, mechani cal, photocopying, recording, or otherwise, without prior written permission from the publisher. Enders for 12 years, and together, they developed the attenuated measles virus vaccine, which was licensed in the United States in 1963 and which has resulted in a dramatic decline in the incidence of measles. By 2011, more than a billion chil dren had received the measles vaccine as a key part of the initiative to eliminate measles worldwide. In addition to his investigations of measles, Sam has been involved in studies of smallpox, polio, rubella, infuenza, pertussis, and Haemophilus infuenzae type b vaccines. He is a giant in the feld of immunizations and has served on virtually every committee or panel in the United States and internationally dealing with vaccine development, licen sure, and policy. Davison Professor of Pediatrics from 1972 to 1997, and he currently is the Wilburt C. He has an enviable memory, both for medical facts and for names and attributes of his generation of "medical children," and he often is seen at meetings giving handshakes, hugs, smiles, and personal greetings. Sam and Cathy raised 8 sons and daughters and now share the joys of spend ing time with their many grandchildren. Sam is devoted to his family, his students, his patients, and his friends and is a true gentleman and scholar. Sam Katz has left a huge mark on the feld of pediatrics and vaccinology and is a giant of 20th century medicine. This edition of the Red Book is dedicated to Sam to thank him on behalf of all the children and pediatricians whose lives are better through his contributions. With the limited time available to the practitioner, the ability to quickly obtain up-to-date infor mation about new vaccines and vaccine recommendations, emerging infectious diseases, new diagnostic modalities, and treatment recommendations is essential. The Committee on Infectious Diseases relies on information and advice from many experts, as evidenced by the lengthy list of contributors to Red Book. Most important to the success of this edition is the dedication and work of the edi tors, whose commitment to excellence is unparalleled. This edition of the Red Book is based on information available as of February 2012. Information is provided in hard copy and as digital versions, which can be downloaded to mobile devices and contain links to supplemental information, including visual images, graphs, maps, and tables. Seemingly unanswerable scientifc questions, the complexity of medical practice, ongoing innovative technology, continuous new information, and inevitable differences of opinion among experts all are addressed when preparing the Red Book. In some cases, other committees and experts may differ in their interpretation of data and resulting recommendations. In certain instances, no single recommendation can be made because several options for management are equally acceptable. In making recommendations in the Red Book, the committee acknowledges differences in viewpoints by use of the phrases "most experts recommend. Inevitably in clinical practice, questions arise that cannot be answered easily on the basis of currently available data. For many conditions, an expert in the feld of infectious diseases should be consulted. Through this process of lifelong learning, the committee seeks to provide a practical and authoritative guide for physicians and other health care professionals in their care of infants, children, and adolescents. New data inevitably will outdate current information in the Red Book, so health care professionals need to remain informed of ongoing developments and resulting changes in recommendations. Throughout the Red Book, Web site addresses enable rapid access to new information. Special appreciation is given to Tanya Lennon, assistant to the editor, for her work, patience, and support. I thank Mimi for always being there and for her patience, understanding, and never-ending support. All Web sites are in bold type for ease of reference, and all have been verifed for accuracy and accessibility. Direct links to visual images have been added throughout the electronic version of the Red Book. These include images of clinical manifestations, maps showing geo graphic locations of specifc diseases, graphs and tables of disease rates, and micro biologic fndings. Reference to use of tetracycline and fuoroquinolone agents in children has been standardized throughout the book, with reference to a standardized approach to use in children. Policy updates released after publication of this edition of the Red Book will be posted on Red Book Online. The table includes hepatitis A, hepatitis B, invasive pneumococcal disease, rotavirus hospitalizations, and varicella.
Discount prandin 1mg with amex
Cases in prepubertal children must be investi-1 gated to determine the source of infection diabetes mellitus type 2 and obesity 2mg prandin fast delivery. Use of this approach always should be accompanied by efforts to educate partners about symptoms and to encourage partners to seek clinical evaluation. Lesions usually involve genitalia, but anal infections occur in 5% to 10% of patients; lesions at distant sites (eg, face, mouth, or liver) are rare. Cases still are reported in Papua, New Guinea, and parts of India, southern Africa, central Australia, and to a much lesser extent, the Caribbean and parts of South America, most notably Brazil. The incidence of infection seems to correlate with sustained high temperatures and high relative humidity. The period of communicability extends throughout the duration of active lesions or rectal colonization. The microorganism also can be detected by histologic examination of biopsy specimens. Diagnosis by poly merase chain reaction assay and serologic testing is available only in research laboratories. Doxycycline should not be given to children younger than 8 years of age or to pregnant women. Ciprofoxacin, which is not recommended for use in pregnant or lactating women or children younger than 18 years of age, is effective. Erythromycin or azithromycin is an alternative therapy for pregnant women or women who are infected with human immunodefciency virus. Antimicrobial therapy is continued for at least 3 weeks or until the lesions have resolved. Relapse can occur, especially if the antimicrobial agent is stopped before the primary lesion has healed completely. Patients should be evaluated for other sexually transmitted infections, such as gonor rhea, syphilis, chancroid, chlamydia, hepatitis B virus, and human immunodefciency virus infections. Immunization status for hepatitis B and human papillomavirus should be reviewed and documented and then recommended if not complete and appropriate for age. Encapsulated strains express 1 of 6 antigenically distinct capsular polysaccharides (a through f); nonen capsulated strains lack capsule genes and are designated nontypable. The mode of transmission is person-to-person by inhalation of respiratory tract droplets or by direct contact with respiratory tract secretions. In neonates, infection is acquired intrapartum by aspiration of amniotic fuid or by contact with genital tract secretions containing the organism. Pharyngeal colonization by H infuenzae is relatively common, especially with nontypable and nontype b capsular type strains. The peak incidence of inva sive Hib infections occurred between 6 and 18 months of age. Historically, invasive Hib was more common in boys; black, Alaska Native, Apache, and Navajo children; child care attendees; children living in crowded conditions; and children who were not breastfed. In the United States, invasive Hib disease occurs primarily in underimmunized children and among infants too young to have completed the pri mary immunization series. Nontypable H infuenzae now causes the majority of invasive H infuenzae disease in all age groups. From 1999 through 2008, the annual incidence of invasive nontypable H infuenzae disease was 1. Gram stain of an infected body fuid specimen can facilitate presumptive diagnosis. In vitro susceptibility testing of isolates from middle-ear fuid specimens help guide therapy in complicated or persistent cases. Careful observation of exposed, unimmunized, or incompletely immunized children who are household, child care, or nursery school contacts of patients with invasive Hib disease is essential. The risk of invasive Hib disease is increased among unimmu nized household contacts younger than 4 years of age. In households with a person with invasive Hib disease and at least 1 household member who is younger than 48 months of age and unimmunized or incompletely immunized against Hib, rifampin prophylaxis is recommended for all household con tacts, regardless of age. Similarly, in households with a contact younger than 12 months of age who has not received the 2 or 3-dose primary series of Hib conju gate vaccine, depending on vaccine product, all household members should receive rifampin prophylaxis. Given that most secondary cases in households occur during the frst week after hospitalization of the index case, when indicated, prophylaxis (see Table 3. When 2 or more cases of invasive Hib disease have occurred within 60 days and unimmunized or incompletely immunized children attend the child care facility or preschool, rifampin prophylaxis for all attendees (irrespective of their age and vaccine status) and child care providers should be considered. In addi tion to these recommendations for chemoprophylaxis, unimmunized or incompletely 1 American Academy of Pediatrics, Subcommittee on Management of Acute Otitis Media. Data are insuffcient on the risk of secondary transmission to recommend che moprophylaxis for attendees and child care providers when a single case of invasive Hib disease occurs; the decision to provide chemoprophylaxis in this situation is at the discretion of the local health department. Treatment of Hib disease with cefotaxime or ceftriaxone eradicates Hib colonization, eliminating the need for prophylaxis of the index patient. Patients who are treated with ampicillin, meropenem, or another antibiotic regimen and who are younger than 2 years of age should receive rifampin prophylaxis at the end of therapy for invasive infection. Rifampin should be given orally, once a day for 4 days (20 mg/kg; maxi mum dose, 600 mg). The dose for infants younger than 1 month of age is not estab lished; some experts recommend lowering the dose to 10 mg/kg. Two single-antigen (monovalent) Hib conjugate vaccine products and 2 combination vaccine products that contain Hib conjugate are available in the United States (see Table 3. Conjugate vaccines vary in composition and immunogenicity, and as a result, recommendations for their use differ. Depending on the vaccine, the recommended primary series consists of 3 doses given at 2, 4, and 6 months of age or 2 doses given at 2 and 4 months of age (see Recommendations for Immunization, p 350, and Table 3. The monovalent Hib conjugate vaccines available in the United States are considered interchangeable for primary and booster immunization. Pain, redness, and swelling at the injection site occur in approximately 25% of recipients, but these symptoms typically are mild and last fewer than 24 hours. For accelerated immunization in infants younger than 12 months of age, a minimum of a 4-week inter val between doses can be used. Recommendations for children who have had a lapse in the schedule of immunizations are based on limited data. Whether these children will beneft from additional doses after completion of the primary series of immunizations and the booster dose at 12 months of age or later is unknown. These children should be immunized according to the age-appropriate schedule for unimmunized children and as if they had received no previous Hib vaccine doses (see Table 3. Immunization should be initiated 1 month after onset of disease or as soon as pos sible thereafter. Extensive bilateral interstitial and alveolar pulmonary edema and pleural effusions are the result of a diffuse pulmonary capillary leak and appear to be caused by immune response to hantavirus in endothelial cells of the microvasculature. The severe myocardial depression is different from that of septic shock; cardiac indices and stroke volume index are low, pulmonary wedge pressure is normal, and systemic vascular resistance is increased. Humans acquire infection through direct contact with infected rodents, rodent drop pings, or nests or inhalation of aerosolized virus particles from rodent urine, droppings, or saliva. At-risk activities include handling or trapping rodents; cleaning or entering closed, rarely used rodent-infested structures; cleaning feed storage or animal shelter areas; hand plow ing; and living in a home with an increased density of mice in or around the home. Weather conditions resulting in exceptionally heavy rainfall and improved rodent food supplies can result in a large increase in the rodent population. Increased rodent population results in more frequent contact between humans and infected mice and may account for increase human incidence. Most cases occur during spring and summer, and geographic location is determined by the habitat of the rodent carrier. Hantavirus-specifc immunoglobulin (Ig) M and IgG antibodies are present at the onset of clinical disease. A rapid diagnostic test can facilitate immediate appropriate supportive therapy and early transfer to a ter tiary care facility.